Article Text

Abstract
Objective The purpose of the study was to investigate the trends and causes of regional disparities of infant mortality rate (IMR) in rural China from 1996 to 2008.
Design A population-based, longitudinal study.
Setting The national child mortality surveillance network.
Population Population of the 79 surveillance counties.
Main outcome measure IMR, leading causes of infant death and the RR of IMR.
Results The IMR in coastal, inland and remote regions declined by 72.4%, 62.9% and 58.2%, respectively, from 1996 to 2008. Compared with the coastal region, the RR of IMR were 1.7 (95% CI 1.6 to 1.9), 1.9 (95% CI 1.7 to 2.0) and 1.8 (95% CI 1.6 to 2.0) for inland region and 2.6 (95% CI 2.4 to 2.7), 3.2 (95% CI 3.0 to 3.5) and 3.1 (95% CI 2.7 to 3.4) for the remote region during 1996–2000, 2001–2005 and 2006–2008, respectively. The regional disparities existed for both male and female IMRs. The postneonatal mortality showed the highest regional disparities. Pneumonia, birth asphyxia, prematurity/low birth weight, injuries and diarrhoea were the main contributors to the regional disparities. There were significantly more infants who did not seek healthcare services before death in the remote region relative to the inland and coastal regions.
Conclusion The results indicated persistent existence of regional disparities in IMR in rural China. It is worth noting that regional disparities in IMR increased in the remote and coastal regions during 2001–2005 in rural China. These disparities remained unchanged during 2006–2008. The results indicate that strategies to reduce mortality caused by pneumonia, birth asphyxia and diarrhoea are keys to reducing IMR.
This paper is freely available online under the BMJ Journals unlocked scheme, see http://adc.bmj.com/info/unlocked.dtl
Statistics from Altmetric.com
Introduction
Over the past two decades, the survival, health and development of children have aroused global concern. Child health disparities have become a considerable problem in global public health. The Millennium Development Goals (MDGs) aim to reduce inequality between countries and within countries.1 Reducing infant mortality and narrowing the child health disparity gap are the national goals of many countries, including China.2 ,3
Infant mortality rate (IMR) is a common indicator for measuring the standard of child health.4 Health condition of Chinese children has remarkably improved. Between 1991 and 2008, IMR fell from 51.2 to 14.9 per 1000 live births.5 This mortality is lower than a majority of the developing countries.6 However, geographical variations in IMR have always been a challenge for Chinese government because of the geographical divergence and imbalanced economical development. This regional variation is more substantial between the poorly developed remote rural western regions and the well-developed rural coastal regions.7 However, there have been no publications regarding the trends and causes of IMR between the two regions in China. There also have been no reports regarding IMR variations in rural China since 2004. In this study, we carried out a nationwide analysis with data from 1996 to 2008 in rural China. The specific aim of this study was to investigate the trends and causes of the geographical disparities of IMR in rural China in order to guide policies aimed at prevention of issues contributing to a high IMR.
What is already known on this subject
▶ Infant mortality rate (IMR) is a common indicator of the level of child health.
▶ The health condition of Chinese children has remarkably improved between 1991 and 2008.
▶ The regional disparities of IMR were substantial in China between the poorly developed remote rural regions and the well-developed coastal rural regions before 2004.
What this papers adds
▶ The regional disparity of IMR increased between the remote and coastal regions in 2001–2005. However, the increasing trend was not observed in 2006–2008.
▶ Pneumonia, birth asphyxia and diarrhoea were the three main contributors of the regional disparities.
▶ The healthcare accessibility is significantly lower in the western remote region relative to the other two regions.
Methods
Data source
The data for this study was based on the national children mortality surveillance network. The network monitors a population of 13 million that covers 116 representative districts/counties across 31 provinces using stratified sampling strategies. Details on data collection in the surveillance network have been published previously.8 ,9 Each child death was investigated and reported by doctors and then reviewed by the county-level women and child healthcare institute and the county general hospitals to ensure data accuracy. In addition, quality control of data collection was routinely conducted at all levels of the surveillance network. The causes of death were classified according to the International Classification of Diseases-10 (ICD-10).10
Regional categories
The 31 provinces were divided into coastal, inland and remote regions based on geographical locations and economic conditions. The coastal region includes Beijing, Tianjin, Liaoning, Shanghai, Jiangsu, Zhejiang, Fujian, Shandong and Guangdong. The inland region includes Hebei, Shanxi, Heilongjiang, Jilin, Anhui, Jiangxi, Henan, Hubei, Hunan, Guangxi, Hainan, Shaanxi, eastern Sichuan and Chongqing. The remote region includes inner Mongolia, Yunnan, Guizhou, Tibet, Gansu, Qinghai, Ningxia, Xinjiang and western Sichuan. Based on the economic conditions, Sichuan Province was divided into eastern Sichuan and western Sichuan which were assigned to the inland and remote region, respectively (figure 1).

Geographical distribution of coastal, inland and remote regions in China.
Among the 116 representative districts/counties, 79 were in rural areas. Of those in the rural areas, 19 were in the coastal region, 38 in the inland region and 22 in the remote region. All the data used in this study were from the rural regions.
Statistical analysis
The IMR was calculated as the number of deaths within one year of birth per 1000 live births. IMR was further broken down into early neonate mortality rate (ENMR) (0–6 days of birth), late neonate mortality rate (LNMR) (7–27 days of birth) and post-neonate mortality rate (PNMR) (28–364 days of birth).
Premortality healthcare services were categorised into inpatient, outpatient and untreated groups based on the healthcare encountered 24 h before death. Healthcare services that the infants received 24 h before the death were divided into five levels based on the Chinese healthcare system. They are provincial/municipal hospital, county/district hospital, township/neighbourhood hospital, village doctor and no healthcare seeking. For this study, the hospital at the highest level was recorded as the level of hospital visited before death if two or more hospitals had been visited. Accessibility to healthcare was indicated by premortality treatment, the proportion of each category of hospitals visited and the proportion of infants not seeking healthcare. Injury-related death is not included due to the low hospital visiting rate after incidence of injury.
We artificially assigned the whole observational period from 1996 to 2008 into three periods (1996–2000, 2001–2005 and 2006–2008) for statistical purposes because the annual number of deaths was too low to precisely calculate the mortality.
SAS 9.0 (SAS Institute, Carey, North Carolina, USA) was used for the data statistical analysis. Cases that had missing information in the categories analysed were excluded for statistical analysis, but were included in other categories that had complete information. The Cochran-Armitage test was conducted to calculate the IMR and the causes-specific IMR over time within each region. The Woolf method was used to calculate the RR and 95% CI between different regions. Consistency for RR of the mortality or cause-specific IMR between regions during the three time periods was tested by Woolf's Consistency Test. If the RR were inconsistent between different periods, the interaction exists between region and time periods.11 ,12
Results
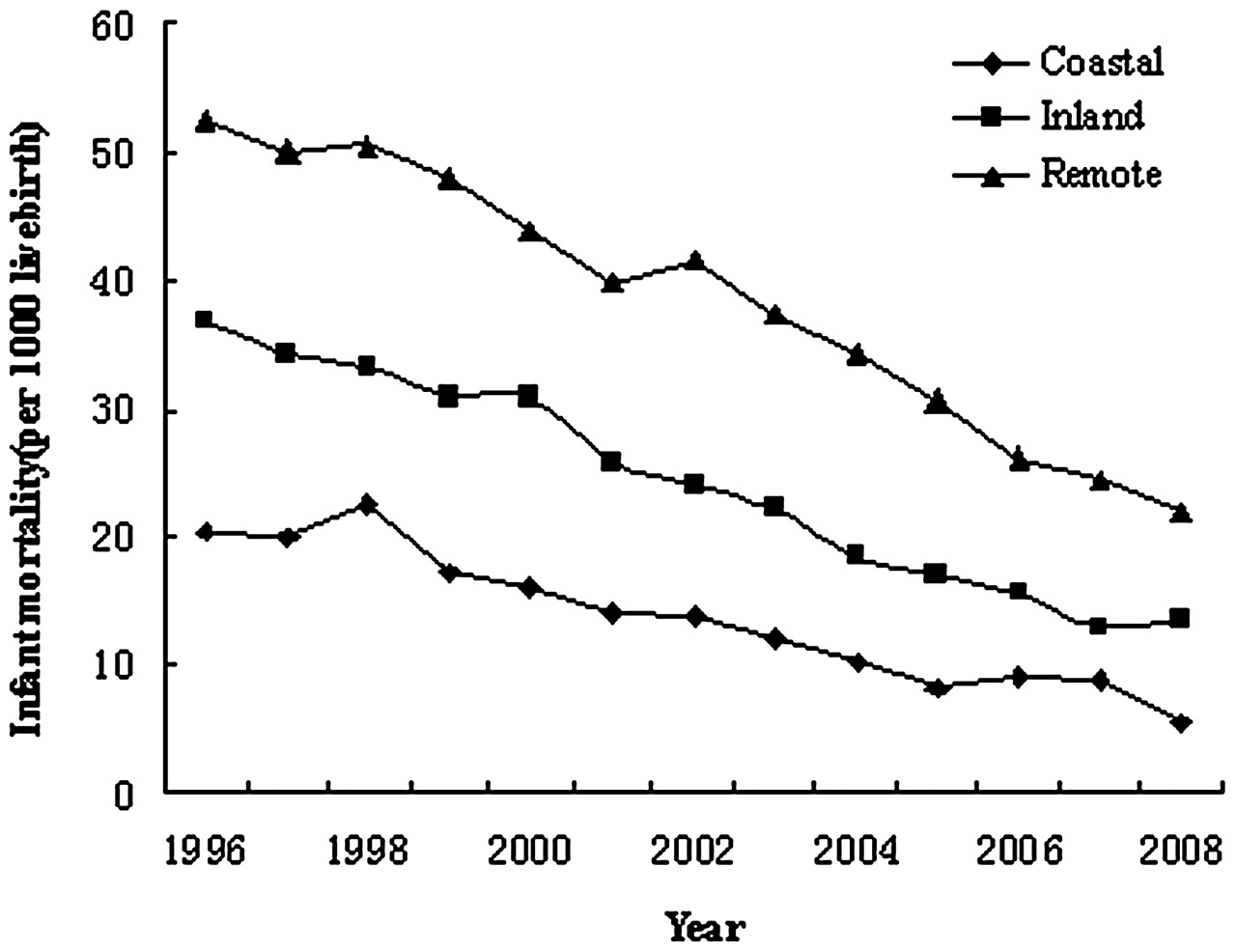
From 1996 to 2008, the reduction of IMR in the coastal, inland and remote regions were 72.4%, 62.9% and 58.2%, respectively (p<0.01), with a significantly less decline in the remote region (figure 2). The ENMR was the highest, followed by PNMR and then LNMR. Compared with the coastal region, the RR of ENMR, LNMR and IMR increased from 2.0 (95% CI 1.8 to 2.2), 2.4 (95% CI 2.1 to 2.9) and 2.6 (95% CI 2.4 to 2.7), respectively, during 1996–2000 to 2.8 (95% CI 2.5 to 3.1), 3.6 (95% CI 2.9 to 4.5) and 3.2 (95% CI 3.0 to 3.5) during 2001–2005 in the remote region (p<0.01) . These rates stayed flat during the 2006–2008. The RR of the abovementioned mortalities were not changed when comparing the inland region with the coastal region during 1996–2008 (p>0.05) (table 1).

Trend of infant mortality in rural China during 1996–2008.
IMR in different regions in rural China
As of the gender impact on IMR, first we examined the regional difference in each gender. Both genders had higher IMRs in the inland and remote regions than in the coastal region. Then next, we examined the IMR difference between the two genders. The RRs presented here were the IMR of male infants relative to the female infants. The RRs were greater than 1 during periods 1996–2000 and 2006–2008, with the exception of period 2001–2005. The 95% CI of RR were 0.9 to 1.3, 1.0 to 1.3 and 0.9 to 1.1 during 2006–2008 in the coastal, inland and remote regions, respectively (table 2).
IMR in different genders in rural China
The main diseases that caused infant deaths were pneumonia, birth asphyxia, prematurity/low birth weight (LBW), diarrhoea, injuries and congenital anomalies, which accounted for 80% of the total infant deaths. Most of the cause-specific mortalities declined within each region (p<0.01) with the exception that there were no significant changes for diarrhoea-caused IMR in the coastal region and congenital anomaly-caused IMR in the remote region (table 3).
Risks of cause-specific infant mortality in the three regions in rural China
Compared with the coastal region, the inland and remote regions had higher IMRs resulted from pneumonia, birth asphyxia, prematurity/LBW, injuries and diarrhoea during the entire study time period with the exception of the diarrhoea-caused IMR in inland region during 2006–2008. Compared with the coastal region, the RR of IMRs caused by pneumonia, birth asphyxia, prematurity/LBW, diarrhoea and congenital anomalies increased during 2001–2005 for the remote regions (p<0.05). There was no significant change during 2006–2008. The RR of the abovementioned cause-specific IMR, except congenital anomalies between inland and coastal region, had no significant change during the three time periods (p>0.05) (table 3).
A high accessibility was considered when the infants visited the provincial/municipal or county/district hospitals before death. Individuals seeking treatment at hospitals in these two levels significantly increased throughout all three regions. However, during 2006–2008, the percentage of individuals going to higher-levelled hospitals was significantly lower in the remote region (56%) relative to the coastal region (84%) (table 4).
Proportion of premortality treatment and premortality healthcare service among the three regions in rural China
There was a steady increase in inpatient care throughout the three regions. A persistent decrease of infants who did not seek healthcare service was also seen, with the greater proportion of infants who did not visit doctors in the remote region (25%) relative to the coastal region (5%) (p<0.01) (table 4).
Reasons behind the lack of healthcare-seeking behaviour before infant death were explored. We analysed data from 2003 to 2008 because the network only collected information regarding this matter during this time period. The time period was divided into 2003–2005 and 2006–2008 for statistical purposes. In the coastal region, the main reasons for no healthcare seeking were delayed hospital visits and others (parents gave up treatment due to severe congenital anomalies of infants) during these two time periods. For the inland and remote region, the main reasons included delayed hospital visits, lack of knowledge of the severity of the diseases among the parents, religious or ethnic beliefs and financial difficulties. In the remote region, the cases of infant death due to the parent's lack of knowledge were significantly higher during 2006–2008 than 2003–2005. Other main reasons also included financial difficulties (11%) and transportation issues (9%) in the remote region (figure 3). There were some missing data in this study. But the bias can be ignored since only less than 0.5% data were missing.

{kind=link}
{kind=link}
{kind=link}
The proportion of reasons behind the lack of healthcare-seeking behaviour before infant death in the three regions during the period of 2003–2005 and 2006–2008.
Discussion
In rural China, the regional disparities of ENMR, LNMR, PNMR and IMR are still an issue although IMRs are remarkably declined. Disparities in PNMR were higher than ENMR and LNMR. Regional disparities in IMR exist in both genders. Between the remote and the coastal regions, disparities in IMR were significantly higher during 2001–2005 and remained flat during 2006–2008. Liu et al reported that the IMR was significantly higher in six provinces in the western region relative to the four provinces in the coastal region and two inland provinces from 1990 to 2000.7 Our results showed a similar trend, but on a much larger scale and over a longer time period. Furthermore, it has been demonstrated that the regional disparities in IMR in China are not improved. Disparities in children's health have not been significantly reduced in developed or underdeveloped countries. The disparities in children's health challenge the Chinese government and a majority of the countries globally.13,–,19
Our findings showed that more than 60% of infant deaths happened during the neonatal period and more than 75% of neonatal deaths happened during the early neonatal period. Our results are similar to reports published by a number of other countries.20 Tomashek et al reported that the neonatal mortality rate (NMR) among American Caucasian was counted for 62.0% of the IMR.21 During the past two decades, the NMR has been declining very slowly in a majority of countries. To achieve the MDGs and reduce the mortality of children and infants, the United Nations' Children's Fund stresses strategies that efficiently reduce NMRs.22 Our results indicate that the PNMR had the highest regional disparities. This is similar to what the reports by Bladwin showed that the adjusted OR for PNMR between American Indians and Alaska natives and rural Whites was higher than that for NMR between them (1.46 vs 0.85).23
During 2006 to 2008, the 95% CI of RR of male IMR versus female IMR in the coastal and inland regions were 0.9 to 1.3 and 1.0 to 1.3, respectively. Considering that the range of this RR between 1.2 and 1.3 was commonly accepted as a standard by a number of studies,24 our data suggested that there was no significant IMR difference between genders in the coastal and inland regions. The remote region had relative higher IMR in female than male infants, which was similar to the reports from east Asia and South Asia.25
The reason of variations in IMR, although not clear, may be complex and synergistic. It can be attributed to multiple factors such as socioeconomic circumstances, healthcare accessibility and fertility rate.26,–,30 The socioeconomic factor is probably one of the major contributors to the inequality in infant mortality in rural China. First, although the Chinese economy has been rapidly growing in the past 10 years, the gap of gross domestic product per person between the coastal and remote western regions in 2008 was increasing when compared with 2000.31 The imbalanced rapid economy growth may have contributed to the unchanged RR of IMR between 2001–2005 and 2006–2008 for the remote region relative to the coastal region. Secondly, among the 592 poorest counties, 366 were in the remote regions where 66% of the population was in poverty.32 Third, 10.7% of the infant death in the untreated group in the remote region in our study was due to financial difficulties.
Our results indicated that lack of accessibility to health services and lack of knowledge of care-seeking/warning signs among parents may be the main impact to the regional disparities of IMR. Healthcare accessibility is negatively correlated with infant mortality (Shi et al).27 Limited healthcare resources could be one of the major contributors to the limited accessibility of healthcare. A national healthcare survey in 2008 showed that the number of healthcare workers in township hospitals and village clinics was 1.37 and 1.22 per 1000 rural populations in the coastal region, while 0.95 and 0.91 in the remote region, respectively.33 In this study, the significantly lower number of visits to provincial/municipal and county/district hospital before infant death in the remote region relative to the other two regions further supports the importance of the healthcare accessibility. The analysis on the reasons for dead infants without treatment before death during 2006–2008 indicated that 39% were caused by unawareness of the severity of the disease among parents and 26% by delayed hospital visiting. Both of the two main reasons may suggest a relative lower education level of the parents.
IMR is positively correlated with total fertility rate.21 The total fertility rate dropped from 2.9 in 1979, when the one-child policy started, to 1.7 in 2004.34 ,35 The one-child policy actually allows two children per family if you are a minority. These individuals mostly live in the remote region of China (73.15% in 1990). The average fertility rate is 2.0–2.5 in the remote region, while the rate is more than 3.0 for over 50% of the minorities.36,–,38 This indirectly supported the relationship of fertility rate to IMR.
Pneumonia, birth asphyxia, prematurity/LBW, injuries and diarrhoea were the main diseases that caused an increased RR in IMR in the remote region compared with the coastal region. This indicates that certain procedures are able to facilitate the improvement of regional disparities in infant mortality such as resuscitation training to decrease birth-asphyxia-related mortality.39 ,40
The limitations of our study included the following: (1) we did not have data related to household income and maternal education and age, which prevented us from researching the direct relationship between these factors and IMR. (2) We did not have data of healthcare service for the whole population. Our analysis was based on the healthcare provided to the infants before death. Therefore, our results about the healthcare accessibility were biased.
To summarise, this study indicated remarkable declines in IMR in rural China in the past 13 years with the preservation of regional variations. It is worth noting that regional disparities in IMR increased between the remote and coastal regions in 2001–2005. However, the increasing trend was not observed in 2006–2008. Pneumonia, birth asphyxia and diarrhoea were the three main contributors to the regional disparities. This data may provide a basic information and may help direct Chinese government to reduce the geographical disparities by increasing healthcare accessibility, by formulating related policies and by enhancing doctor training on neonate resuscitation.
Acknowledgments
The authors would like to thank all health workers in this surveillance system for providing the data and investigating the cause of death.
References
Footnotes
-
Funding This work was supported by the Ministry of Health, China (grants QT2003-009 and 05 wsb-02) and UNICEF (grant YH601-11-1141) and Program for Changjiang Scholars and Innovative Research Team in University (IRT0935).
-
Competing interests None.
-
Provenance and peer review Not commissioned; externally peer reviewed.