Article Text

Abstract
Background Invasive fungal infections are a major cause of morbidity and mortality in preterm infants. The authors conducted the first prospective, randomised controlled trial of nystatin compared with fluconazole for the prevention of fungal colonisation and invasive fungal infection in very low birth weight (VLBW) neonates.
Methods During a 12-month period, all VLBW neonates were assigned randomly to receive nystatin (1 ml suspension, 100 000 U/ml, every 8 h), fluconazole (3 mg/kg body weight, every third day) or placebo from birth until day 30 of life (day 45 for neonates weighing <1000 g at birth). The authors performed weekly surveillance cultures and systemic fungal susceptibility testing.
Results During the study period, 278 infants (fluconazole group, n=93; nystatin group, n=94; control group, n=91) weighing <1500 g at birth were admitted. There were no differences in birth weight, gestation, gender or risk factors for fungal infection among the groups. Fungal colonisation occurred in 11.7% of the nystatin group and 10.8% of the fluconazole group, as compared with 42.9% of the control group. The incidence of invasive fungal infection was 4.3% in the nystatin group and 3.2% in the fluconazole group, as compared with 16.5% in the control group. There were no differences in fungal colonisation and invasive fungal infection between the nystatin and fluconazole groups.
Conclusions Prophylactic nystatin and fluconazole reduce the incidence of colonisation and invasive fungal infection in VLBW neonates. The authors believe that nystatin is an alternative to fluconazole, because nystatin is safe, inexpensive, well tolerated and effective.
Statistics from Altmetric.com
Introduction
Invasive fungal infections are associated with significant morbidity and mortality among preterm infants cared for in the neonatal intensive care unit (NICU). Fungal organisms account for 12% of first-episode, late-onset sepsis in very low birth weight (VLBW) infants weighing <1500 g; half of these cases are caused by Candida albicans.1 Invasive fungal infection in VLBW infants is associated with significant morbidity and mortality. In a review article, Chapman reported that Candida bloodstream infection in neonates has a crude mortality of ∼30%. The prevention of candidaemia may reduce this mortality and morbidity.2
What is already known on this topic
▶ Very low birth weight (VLBW) infants are at high risk of developing invasive fungal infections.
▶ Fluconazole prophylaxis reduces the incidence of invasive fungal infection and fungal colonisation in VLBW infants.
▶ Oral nystatin prophylaxis is associated with a lower incidence of fungal infection compared with no antifungal prophylaxis.
What this study adds
▶ Both fluconazole and nystatin prophylaxis reduce the incidence of invasive fungal infection and fungal colonisation in VLBW infants.
▶ Nystatin prophylaxis is similar in efficacy to fluconazole prophylaxis in VLBW infants.
▶ Nystatin is a good alternative to fluconazole for antifungal prophylaxis in VLBW infants.
The efficacy and safety of fluconazole prophylaxis in preterm infants has been reported in four randomised controlled trials (RCTs) and a systematic review, with no significant adverse effects reported.3,–,7
There is evidence of reduced fungal colonisation and infection in VLBW infants after the introduction of nystatin prophylaxis.8 9 In a recently reported randomised trial of nystatin prophylaxis, Ozturk et al10 found a reduced incidence of invasive fungal infection.
This paper presents the results of the first prospective, RCT of nystatin compared with fluconazole for the prevention of fungal colonisation and invasive fungal infection in VLBW neonates in the NICU.
Materials and methods
We conducted a prospective, randomised controlled clinical trial to compare the efficacy and safety of fluconazole and nystatin for the prevention of fungal colonisation and invasive fungal infection in VLBW neonates. From June 2008 to June 2009, all infants with birth weights <1500 g admitted to the NICU at Zekai Tahir Burak Maternity Hospital (Ankara, Turkey) were eligible for the study. Patients were enrolled within the first 72 h of life. Exclusion criteria were parental refusal, admission after 72 h of life, congenital defects requiring surgical intervention, fatal chromosomal defects and liver failure defined as aspartate transaminase (AST) and alanine transaminase (ALT) levels that were three times the upper limit of normal.
The primary objective was to evaluate the effectiveness of fluconazole and nystatin in the prevention of fungal colonisation and infection. Secondary objectives were the assessment of the incidence of bacterial sepsis, necrotising enterocolitis, threshold retinopathy of prematurity requiring surgery, severe intraventricular haemorrhage, bronchopulmonary dysplasia and mortality.
The study was approved by the hospital ethics committee, and informed written consent was obtained from the parents or guardians before enrolment.
Using computer-generated randomisation, the drugs were assigned to the infants randomly to form three groups in a 1:1:1 ratio, and the daily drug doses were prepared. Infants received fluconazole, nystatin or placebo. In the first group, the infants received intravenous fluconazole (Triflucan; Pfizer) 3 mg/kg/dose, every third day. Extremely low birth weight (ELBW) infants received prophylaxis for 6 weeks; neonates weighing 1000–1500 g received prophylaxis for 4 weeks as described by Manzoni et al. The administration of fluconazole began on day 3 with one daily dose intravenously (when a catheter was present) or through an orogastric tube (when enteral feeding was established).3 In the second group, the infants received nystatin (Micostatin; Bristol-Myers Squibb)suspension (100 000 U/ml) every 8 h. The oral cavity was coated with ∼0.5 ml of nystatin, and the rest was given through an orogastric tube. In the third group, the infants received placebo consisting of equal volumes of intravenous or oral normal saline. The administration of the study drugs (fluconazole, nystatin and placebo) and collection of surveillance cultures were discontinued before the end of the 4–6-week prophylaxis period if (1) antifungal therapy was initiated for the treatment of a documented or presumed invasive fungal infection, (2) the infant was discharged from the hospital or transferred to another facility or (3) the infant died.
Liver function, including serum AST, ALT, alkaline phosphatase (ALP), γ-glutamyltransferase (GGT) and bilirubin levels, was surveyed weekly.
Invasive fungal infection was diagnosed as a positive culture from blood (peripheral venipuncture), urine (≥10 000 or more colony-forming U/ml from sterile bladder catheterisation or suprapubic aspiration) or cerebrospinal fluid. Systemic treatment for invasive fungal infections consisted of intravenous liposomal amphotericin B at the recommended dose. Invasive fungal infection was considered to have caused mortality when death occurred within 3 days of a positive blood culture or when there was autopsy evidence of disseminated candidiasis.
Fungal isolation, identification and fluconazole-susceptibility testing
Fungal surveillance cultures of the skin (intertriginous and, when present, moist areas), gastrointestinal tract (gastric aspirate, stool or rectum) and respiratory tract (tracheal secretions if intubated and nasopharyngeal sample if not intubated) were obtained by three study personnel at study enrolment and then weekly during the 4-week (6-week in <1000 g infants) prophylaxis period.
Stool, gastric aspirate and nasopharyngeal samples and tracheal secretions were submitted in sterile transport containers, and skin and rectal specimens were obtained using swabs. All specimens were inoculated on Sabouraud dextrose agar, and the plates were incubated at 37°C for 48 h. Identification tests were performed using ID 32C (BioMérieux, France). The susceptibility of Candida isolates to the antifungal agent fluconazole was tested using an ATB-Fungus-3 system (BioMérieux) according to the manufacturer's instructions. The susceptibilities of Candida species to fluconazole that were determined with the ATB instrument (mini API, BioMérieux) were identical to the minimum inhibitory concentration (MIC) of ≤8 µg/ml as recommended by the National Committee for Clinical Laboratory Standards. The interpretative breakpoint of fluconazole resistance was defined as at least 64 µg/ml.11
Side effects and patient safety
Hepatic (AST, ALT, ALP, GGT and total and direct bilirubin), haematologic (white cell count and differential, platelet count, haematocrit) and renal (blood urea nitrogen, creatinine) functions were screened weekly while the infants were receiving the study drugs. Fluconazole was discontinued if the AST and ALT levels were >250 IU/l.
Statistical analysis
Demographic variables are expressed as frequency counts and percentages. χ2 Tests were used to compare ratios. Non-parametric comparisons between the patient groups were made with the Kruskal–Wallis test. Survival rates were calculated with the Kaplan–Meier method, and the differences between groups were assessed with the log-rank test. Logistic regression analysis was used to determine the OR of potential risk factors for invasive fungal infection. All independent variables with p<0.20 in the univariate analyses were included in the multivariate analysis. A two-tailed p<0.05 was considered statistically significant. Statistical analyses were done using SPSS V.15.0.
Results
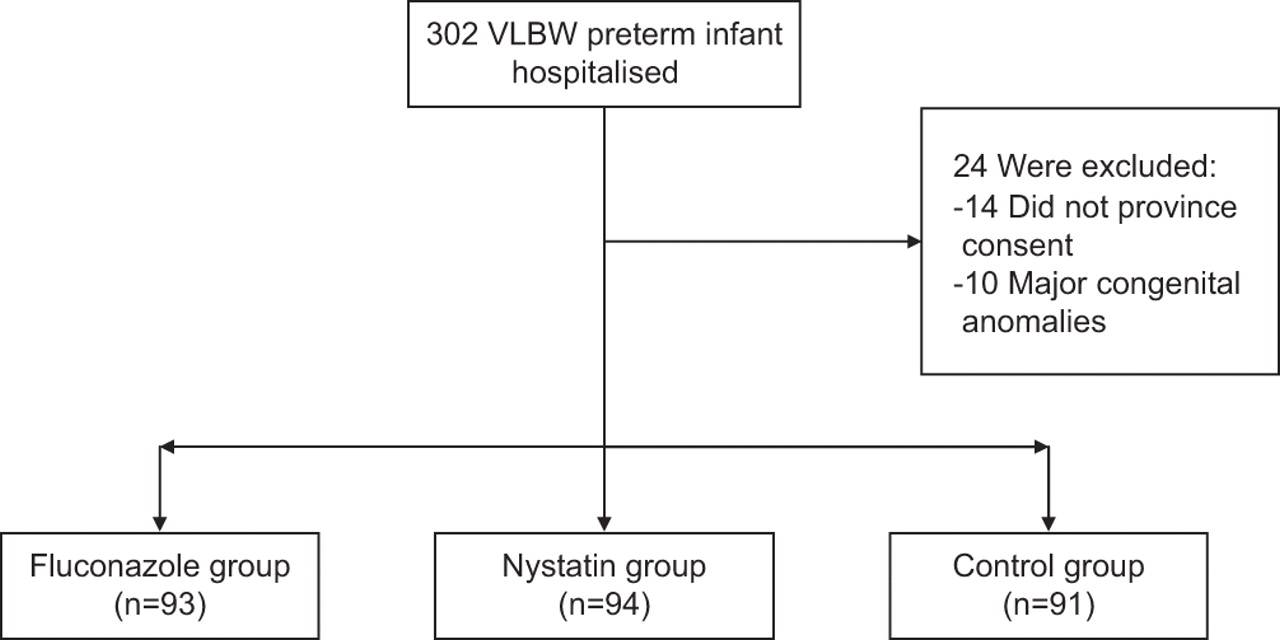
A total of 302 VLBW neonates were hospitalised in the study period. Of these neonates, 24 were excluded (14 of them did not provide consent, 10 of them had major congenital defects). A total of 278 VLBW neonates survived for at least 3 days and were assigned randomly to the fluconazole (n=93), nystatin (n=94) or control groups (n=91) (figure 1). The demographic and neonatal characteristics and major risk factors for fungal infections are listed in table 1. There were no significant baseline differences in risk factors for invasive fungal infection among the groups. Multivariate logistic analysis adjusted for the most important risk factors is summarised in table 2.

{kind=link}
Flowchart of the participants.
Characteristics of the patients and major risk factors for invasive fungal infection*
Multivariate logistic analysis adjusted for the most important risk factors for invasive fungal infection
Secondary outcomes
There were no significant differences in secondary outcomes (table 3). No serious adverse effects of the fluconazole or nystatin therapy were documented. Specifically, there was no appreciable adverse effect of fluconazole therapy on the levels of AST, ALT, ALP, GGT, total bilirubin or direct bilirubin. No infant was withdrawn from the study because of changes in liver function tests.
Secondary end points, rates of invasive fungal infection, progression from colonisation to invasive infection, previous colonisation and mortality*
Fungal colonisation and invasive fungal infection
Data on fungal colonisation, invasive fungal infection and the distribution of fungal species and colonisation sites and infection are shown in tables 3 and 4. Fungal colonisation occurred less frequently in the fluconazole (10.8%) and nystatin (11.7%) groups than in the control group (42.9%; p<0.001). Fungal colonisation at two or more sites occurred in six of the infants in the fluconazole group (6.5%) and five of the infants in the nystatin group (5.3%) versus 28 of those in the control group (30.8%; p<0.001).
Distribution of candida fungal species and sites of colonisation and infection
In addition, invasive fungal infection was less frequent in the fluconazole (3.2%) and nystatin groups (4.3%), as compared with in the control group (16.5%; p<0.001). The 22 episodes of invasive fungal infection were caused by C albicans (17 patients), Candida parapsilosis (four patients) and Candida pelliculosa (one patient) (table 4).
Fluconazole and nystatin did not have any effect on the association between colonisation and subsequent progression to invasive fungal infection, which occurred in 30% of the infants in the fluconazole group and 36% in the nystatin group, as compared with 38% in the control group (p=0.48).
Mortality
The overall mortality was similar among the three groups (8.6% in the fluconazole group and 8.5% in the nystatin group, as compared with 12.1% in the control group; p=0.64). Mortality attributable to fungal infection was also similar among all three groups (1.1% in the fluconazole group and 1.1% in the nystatin group, as compared with 3.3% in the control group; p=0.42; table 3).
Isolates natively resistant to fluconazole
There were no infections with Candida krusei or Candida glabrata and no significant between-group differences in the incidence of colonisation with C krusei or C glabrata. Overall, one of these species was isolated in the fluconazole group (C glabrata) and two in the control group (C krusei and C glabrata) (table 4).
Antifungal susceptibility
The sensitivity to fluconazole did not vary during the study period. In addition, all infecting and colonising isolates were sensitive to amphotericin B and flucytosine.
Discussion
We performed the first prospective, RCT comparing nystatin with fluconazole for the prevention of fungal colonisation and invasive fungal infection in VLBW infants. This study demonstrated that nystatin prophylaxis is similar in efficacy to fluconazole prophylaxis in VLBW infants. The incidences of fungal colonisation and invasive fungal infection were similar for both drugs.
No previous prospective, randomised controlled study has examined fluconazole versus nystatin prophylaxis in reducing the incidence of invasive fungal infection in VLBW infants. Previous studies have reported on the efficacy of a single antifungal agent in the prevention of invasive fungal infection by reducing fungal colonisation. The efficacy of using prophylactic intravenous fluconazole during the first 6 weeks of life to prevent fungal colonisation and invasive fungal infection in ELBW infants was first reported by Kaufman et al.4 Kicklighter et al showed that the prophylactic administration of fluconazole to VLBW infants for the first 28 days of life is safe and results in a decreased risk for Candida colonisation.6 Fluconazole was given intravenously until oral feedings were tolerated. Kaufman et al5 demonstrated that twice-weekly dosing with prophylactic intravenous fluconazole can decrease Candida colonisation and invasive infection in high-risk ELBW infants. Recently, Manzoni et al3 reported that prophylactic fluconazole reduced the incidence of colonisation and invasive infection in VLBW neonates. In our study, fluconazole prophylaxis reduced the incidence of fungal colonisation (10.8%) and invasive fungal infection (3.2%), compared with no prophylaxis (42.9% and 16.5%, respectively), in VLBW infants. There were no differences in overall mortality between the fluconazole and control groups. We think high invasive fungal infection incidence among our control group is due to injudicious and long-term administration of antibiotics such as cephalosporins, carbapenems and vancomycin. Our NICU is a tertiary care referral centre. Frequent and long term usage of total parenteral nutrition and invasive procedures such as catheterisation, intubation may be another reason for this high infection and colonisation rate.
The first RCT of nystatin prophylaxis (100 000 U orally, three times daily) was conducted in ventilated preterm infants weighing less than 1250 g until 1 week after they were extubated; significant reductions in invasive fungal infection were observed, with no difference in mortality between the treatment and control groups.8 Ozturk et al10 conducted a prospective study of nystatin prophylaxis (100 000 U, three times daily, orally or via an orogastric tube) in both preterm and term NICU patients and demonstrated that nystatin prophylaxis reduced the incidence of invasive candidiasis in both ELBW and VLBW infants. Recently, a sequential study reported by Ganesan et al9 showed that the introduction of a prophylactic nystatin administration policy for babies born before 33 weeks was associated with a significant reduction in fungal colonisation and invasive fungal infection. In a more recent prospective surveillance study reported by Howell et al,12 oral nystatin prophylaxis was associated with a significantly lower incidence of fungal infection, as compared with no prophylaxis. Our study demonstrated that nystatin prophylaxis reduced the incidence of fungal colonisation (11.7%) and invasive fungal infection (4.3%) as compared with no prophylaxis (42.9% and 16.5%, respectively) in VLBW infants, and there was no difference in overall mortality between the nystatin and control groups.
In our study, there is no statistically significant reduction in either invasive fungal infection related or overall mortality with usage of both drugs. But our study groups are small to evaluate the mortality difference.
Recently, Violaris et al13 compared the safety and efficacy of oral fluconazole and nystatin prophylaxis in VLBW infants in a prospective trial and found that mortality was higher in the nystatin group than in the fluconazole group. However, their results did not support any conclusions about the relative efficacy of fluconazole versus nystatin in preventing invasive fungal infection. In their study no data regarding colonisation, surveillance cultures and MICs to obtain antifungal resistance were available. Our study found no differences in fungal colonisation, invasive fungal infection or overall mortality between the nystatin and fluconazole groups.
The use of antifungal prophylaxis is associated with a potential risk for selection of resistant organisms. This may take the form of either a subtle increase in the MICs for previously sensitive species or an increased incidence of natively resistant species (C krusei and C glabrata).3 No increase in either the incidence or isolation of resistant species or in the MIC for Candida was observed with either drug in our study, although our study was too short to determine the risk for selection for resistance. Furthermore, it is important to note that susceptibility testing of fungal isolates is imperfect and that MIC breakpoints may not accurately predict in vivo susceptibility.14
Some authors have reported that fluconazole prophylaxis can be associated with hepatotoxicity14 or mild, transient increases in liver enzymes without clinical complications.4,–,6 No adverse effects or liver function impairment related to fluconazole were detected in the fluconazole group, and prophylaxis was not discontinued in any of the 93 infants.
In a multicentre RCT, Manzoni et al3 found that fluconazole dosages of 3 and 6 mg/kg were equally effective. However, dosing with 3 mg/kg is preferable for two reasons: the drug concentrations in the skin, lung and mucous membranes are greater than the plasma levels, and the use of higher doses may foster the development of fungal resistance. Kaufman et al5 reported that twice weekly fluconazole prophylaxis was similar in efficacy to the more frequent dosing in their first study in high-risk preterm infants. In our study, fluconazole was administered in doses of 3 mg/kg, initially intravenously and then via the orogastric route, every third day until 4 or 6 weeks.
In conclusion, prophylactic nystatin and fluconazole reduced the incidence of colonisation and invasive fungal infection in neonates weighing less than 1500 g at birth. There were no effects on mortality with either drug. Further study in a much larger study cohort is needed to evaluate the effects of nystatin and fluconazole prophylaxis on mortality. We believe that nystatin is a good alternative to fluconazole, because nystatin is safe, easy to use, inexpensive, well tolerated and effective. Nystatin is certainly a better option than no prophylaxis.
References
Footnotes
-
Competing interests None.
-
Ethics approval This study was conducted with the approval of the Zekai Tahir Burak Maternity Hospital Local Ethics Committee.
-
Patient consent Parental consent obtained.
-
Provenance and peer review Not commissioned; externally peer reviewed.