Article Text

Abstract
Objectives Conventional MRI at term age has been reported to be superior to cranial ultrasound (cUS) in detecting white matter (WM) abnormalities and predicting outcome in preterm infants. However, in a previous study cUS was performed during the first 6 weeks only and not in parallel to MRI at term age. Therefore, the aim of the present work was to study brain injuries in preterm infants performing concomitant cUS and MRI at full-term age.
Methods In a population-based cohort of 72 extremely low gestational age infants paired cUS and conventional MRI were performed at term age. Abnormalities on MRI were graded according to a previously published scoring system. On cUS images the lateral ventricles, the corpus callosum, the interhemispheric fissure and the subarachnoidal spaces were measured and the presence of cysts, grey matter abnormalities and gyral folding were scored.
Results Moderate or severe WM abnormalities were detected on MRI in 17% of infants and abnormalities of the grey matter in 11% of infants. Among infants with normal ultrasound (n=28, 39%) none had moderate or severe WM abnormalities or abnormal grey matter on MRI. All infants with severe abnormalities (n=3, 4%) were identified as severe on MRI and cUS.
Conclusions All severe WM abnormalities identified on MRI at term age were also detected by cUS at term, providing the examinations were performed on the same day. Infants with normal cUS at term age were found to have a normal MRI or only mild WM abnormalities on MRI at term age.
Statistics from Altmetric.com
Introduction
Cranial ultrasound (cUS) is the most commonly used brain imaging technique in the neonatal intensive care of preterm infants. It reliably detects major intracranial lesions such as intraventricular haemorrhage, parenchymal haemorrhagic infarctions or cystic periventricular leukomalacia, all strongly predictive for the development of cerebral palsy and severe cognitive impairment.1,–,3 The advantages of cUS are that it is a fast and cheap bedside technique that allows scanning directly after birth and sequentially as often as clinically indicated until term age. However, its sensitivity to detect subtle non-cystic white matter (WM) injuries has been matter of debate.1,–,6
In contrast, conventional MRI has been shown to also allow the detection of microstructural (non-cystic) WM injury in a high number of extremely preterm infants.3,–,9
cUS and conventional MRI have previously been compared in preterm cohorts. In a recent study, Woodward et al demonstrated that abnormal findings on cerebral MRI at term equivalent age predict adverse neurodevelopmental outcome at 2 years of age significantly better than cUS.4 This finding raises the question of whether MRI at term should be introduced as a screening tool for all extremely preterm infants. However, in Woodward et al's study cUS scans were performed only during the first 6 weeks of life and not in parallel to the MRI at term. Hence potentially important information generated from cUS at term age was not taken into account.10 Moreover, it has to be considered that MRI is an expensive, time-consuming and resource-consuming technique that usually requires transport and sometimes sedation. Furthermore, MRI is not available in all hospitals and, if available, waiting lists are usually long.
What is already known on this topic
▶. Brain abnormalities are common in preterm infants with low gestational age.
▶. Cranial ultrasounds (cUS) reliably detects major brain abnormalities that are predictive for neurological outcome.
▶. MRI at term has been shown to be superior to early (≤6 weeks) US in predicting outcome at 2 years of age.
What this study adds
▶. Our study presents population-based data on brain abnormalities in extremely preterm infants detected by cUS and conventional MRI, both performed at term age.
▶. Approximately 40% of extremely low gestational age infants have a normal US at term age. In the subgroup of infants with normal US at term age conventional MRI adds marginally clinically relevant information.
The aim of the present study was to compare cUS and conventional MRI, performed on the same day at term equivalent age, in a population-based cohort of extremely low gestational age (ELGA) infants (below 27 weeks) and to determine what proportion of infants with completely normal cUS findings have clinically significant MRI abnormalities.
Patients and methods
Patients and perinatal data
From August 2004 to November 2006 all infants born with a GA below 27 weeks in the Stockholm region of Sweden were included. A cUS and an MRI scan of the brain were performed on the same day at term equivalent age (38–42 weeks postmenstrual age). The study was approved by the regional ethical committee. Informed consent was obtained from all parents of infants included in the study. Perinatal data and clinical courses were prospectively collected. Infants with chromosomal disorders, congenital abnormalities, congenital infections and proven metabolic or malignant disorders were excluded from further analysis.
MRI imaging
All MRI scans were performed at the Astrid Lindgren Children's Hospital at Karolinska University Hospital in Stockholm, Sweden, using a 1.5 T magnetic resonance system (Philips Intera; Philips, Best, Holland). According to our standard clinical protocol for neonatal MRI, infants were fed and given chloral hydrate (30 mg/kg orally or rectally) 15–30 min prior to the examination. However, if infants were already deeply asleep prior to the examination or if the parents did not give consent to the use of sedative medication, infants were scanned during natural sleep.
In order to reduce acoustic noise we used a combination of three passive hearing protections: commercially available dental putty (Affinis dental putty soft, Coltene, Altstätten, Switzerland) and paediatric ear muffs (Bilsom Junior, Bacou-Dalloz Nordic, Helsingborg, Sweden) as well as an in-house developed acoustic hood that reduces noise levels by 16–22 dBA depending on the pulse sequence.11
Our conventional MRI protocol consisted of anatomical high-resolution imaging including a T1-weighted turbo spin echo scan, an inversion recovery scan and a 3D gradient echo sequence (TR/TE/flip=40 ms/4.6 ms/30°, voxel size=0.7×0.7×1 mm3). Further, T2-weighted turbo spin echo images were acquired in sagittal and coronal slice orientations.
MRI scoring system
MRI images were evaluated independently by three observers blinded to the clinical course of the infants. We used a previously described scoring system to grade grey and WM abnormalities.4 7 8 We have previously reported an interobserver agreement of >98% using this scoring system with the same observers.8 Remaining discrepancies were resolved by discussion and consensus was thus reached in all cases. Five different WM variables were assigned a score 1, 2 or 3: (1) WM signal abnormality (on T1 and/or T2 images), (2) reduction in WM volume, (3) cystic abnormalities, (4) lateral ventricular size and (5) corpus callosum size/myelination stage. WM abnormalities were further classified by the composite score of these five categories (potential range in scores, 5–15) into no WM abnormality (scores 5–6), mild WM abnormality (scores 7–9), moderate WM abnormality (scores 10–12) or severe WM abnormality (scores 13–15). Further, three different grey matter abnormalities were assigned a score 1, 2 or 3: (1) cortical grey matter signal, (2) cortical gyration maturation and (3) size of the subarachnoidal spaces. Scores were added and grey matter appearance was divided into two groups: normal (scores 3–5) or abnormal (scores 6–9) grey matter.
cUS
cUS was performed the same day as the MRI scan. Infants were scanned by one of two examiners (SH and BS) experienced in neonatal cUS using the ACUSON Sequoia ultrasound system (Siemens Medical Solutions, Erlangen, Germany) equipped with a multifrequency sector transducer (5–8 MHz). cUS was performed in coronal and sagittal/parasagittal planes through the anterior fontanelle obtaining sequential images according to Levene et al.12 The images were stored digitally. From these, three independent observers measured the size of lateral ventricles, the corpus callosum, the interhemispheric fissure and the subarachnoidal spaces. The presence of cysts, abnormal echogenicity in the cortical grey matter and gyral folding was also evaluated. Details on how measurements and scoring were performed are presented in the supplementary appendix.
The cUS was considered normal if none of the eight measured or scored items (frontal horn size, ventricular midbody size, interhemispheric fissure, subarachnoidal spaces, cysts, corpus callosum size, gyral folding, abnormal echogenicity in the cortical grey matter; details of the measurements are given in the supplementary appendix) was abnormal/outside the normal range.
Severe abnormalities were predefined as cystic periventricular leukomalacia, cystic defects/WM loss after periventricular haemorrhagic infarctions and global white and/or grey matter loss without focal lesion usually coinciding with severe ventriculomegaly.
All ultrasound findings that were neither normal nor severely abnormal according to the definitions above were classified as mild to moderate abnormalities.
Results
During the study period 132 infants were live born with a GA below 27 weeks in the Stockholm region. In all, 20 infants (17 with GAs of 22 weeks, 3 with GAs of 23 weeks) died in the delivery room after receiving comfort care only. Five infants (four with GAs of 24 weeks, one with a GA of 26 weeks) died in the delivery room despite active treatment. In addition, 23 infants died after admission to the NICU before term age (2 with GAs of 22 weeks, 2 with GAs of 23 weeks, 6 with GAs of 24 weeks, 7 with GAs of 25 weeks and 6 with GAs of 26 weeks). Of the surviving infants (n=84) three infants met the exclusion criteria (one meningomyelocele, one oesophageal atresia, one haemophagocytic lymphohistiocytosis). For five infants the parents did not give consent. In all, 76 infants were scanned, representing 94% of all eligible survivors. In four infants full data analysis was not possible, due to motion artefacts on MRI (n=2) or incomplete cUS (n=2) leaving 72 infants for analysis. Patient characteristics are presented in table 1.
Patient characteristics
MRI scoring results
No or only mild abnormalities were found in 83% of infants, while 17% had moderate or severe WM abnormalities. In more detail, no WM abnormalities were found in 31/72 (43%) infants, mild WM abnormalities in 29/72 (40%), moderate in 9/72 (13%) and severe in 3 infants (4%) Representative images are presented in figure 1. Abnormal grey matter was found in eight (11%) infants (see figure 2). These incidences confirm earlier reported low incidences of moderate and severe WM disease in the Stockholm cohort.8 Four infants had a small punctate cerebellar haemorrhage. Three of the four infants with cerebellar haemorrhage had also supratentorial abnormalities. In one infant the cerebellar haemorrhage was the only pathological finding.

Representative images of infants with severe brain abnormalities. Panel 1: coronal MRI (A) and cranial ultrasound (cUS) (B,C) images of an infant with shunt-dependent posthaemorrhagic hydrocephalus and periventricular cysts. Panel 2: sagittal MRI (A) and cUS (B) images of an infant with a large porencephalic cyst after extensive periventricular haemorrhagic infarction and white and grey matter loss. Panel 3: coronal MRI (A) and cUS (B) images of an infant with cystic defect after periventricular haemorrhagic infarction.
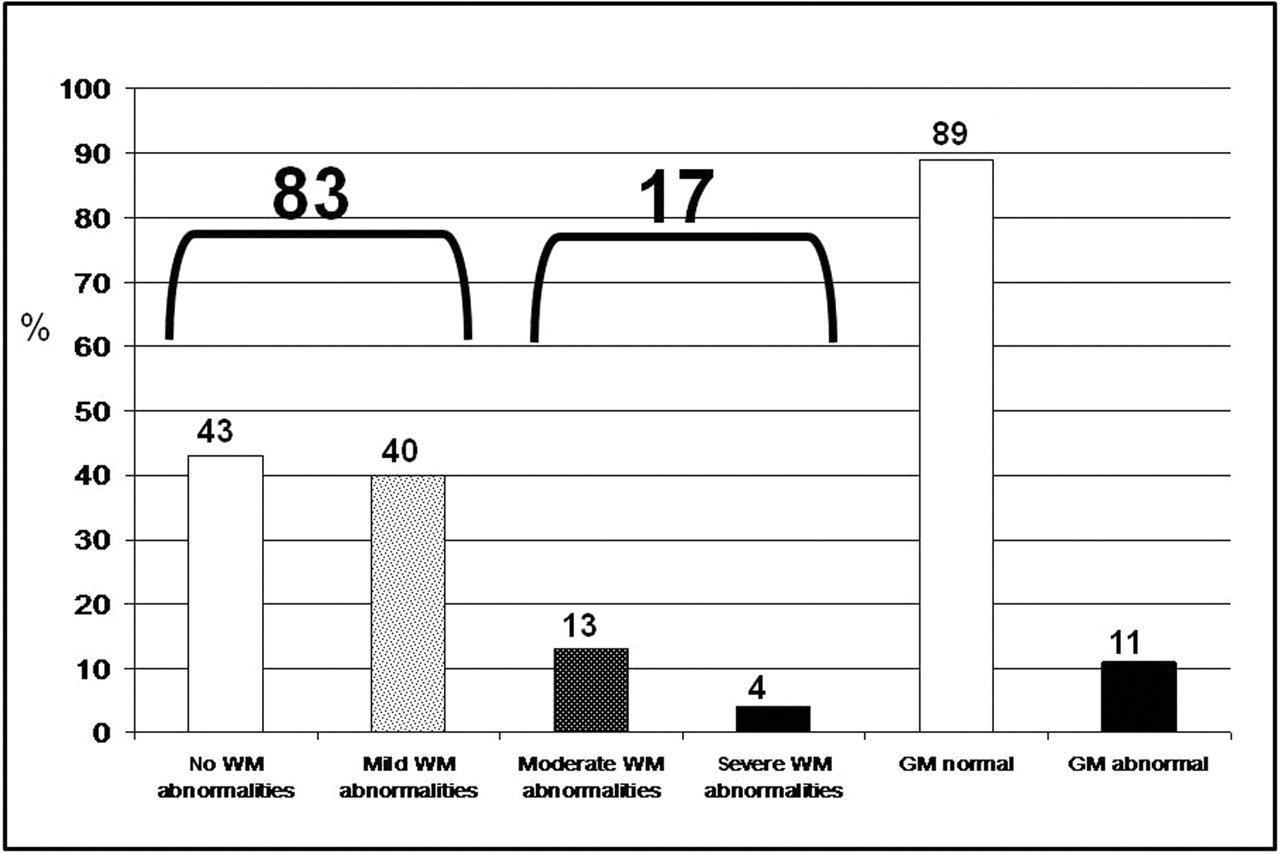
MRI scoring result. WM, white matter.
Ultrasound results
In 28/72 (39%) of infants the cUS at term age was found to be normal. Mild to moderate abnormalities (not normal, not severe) were found in 41/72 infants (57%) and severe abnormalities in 3 infants (4%). Representative images are presented in figure 1.
MRI and ultrasound comparison
All infants with severe abnormalities (n=3) were scored as severely abnormal on cUS and MRI. Out of 28 infants with normal ultrasound at term age, 18 (64%) had a completely normal MRI and 10 (36%) had only mild WM abnormalities on MRI. Thus, none of the infants with normal cUS had moderate or severe WM abnormalities or abnormal grey matter (figure 3). Representative images are presented in figure 1. In all, 10 infants who were scored as normal on MRI were scored as mild to moderate (not normal/not severe) in cUS.

{kind=link}
{kind=link}
{kind=link}
MRI results of infants with normal cranial ultrasound (cUS) at term (n=28). WM, white matter.
In four infants small punctate cerebellar haemorrhage was diagnosed using MRI. None of the cerebellar haemorrhages were diagnosed using cUS via the anterior fontanelle.
Discussion
In this study we present population-based data on paired cUS and conventional MRI performed on the same day at term age in a cohort of ELGA infants. Our two main findings were: first, infants with normal ultrasound at term age had a normal MRI (64%) or only mild (36%) WM abnormalities on MRI. Thus, none of the infants with a normal ultrasound at term age had moderate to severe WM abnormalities or abnormal grey matter on MRI. Second, all infants with severe abnormalities were scored as severe with conventional MRI and ultrasound.
cUS and conventional MRI have been systematically compared before. Both, Woodward et al4 and Mirmiran et al,3 found conventional MRI to be superior to ultrasound in predicting adverse neurodevelopmental outcome at 2 years and cerebral palsy, respectively. This has initiated an ongoing discussion as to whether conventional MRI should be introduced as a screening tool for preterm infants at term age.
However, in both these studies the sensitivity of ultrasound for predicting cerebral palsy (sensitivity/specificity: Woodward et al 18%/95%; Mirmiran et al 29%/86%) was inferior compared to results published by other groups, for example De Vries et al (79%/95%).1 This is likely due to a major difference in study design. While De Vries et al scanned infants weekly from birth until term age, Woodward et al performed only three ultrasound scans within the first 6 weeks of life and Mirmiran et al two scans in the first 2 weeks of life. Thus, information generated from cUS after 6 (2) weeks of life was not taken into account in Woodward et al's or in Mirmiran et al's study. Late cUS can provide information about impaired brain growth, diffuse grey and WM loss (also referred to as signs of brain atrophy) and it has been shown that signs of poor brain growth/brain atrophy are related to adverse neurodevelopmental outcome at 3 years.10 Therefore, we argue that the superiority of MRI at term to sequential cUS from birth to term age still needs to be proven.
We here show that severe abnormalities are equally well diagnosed via both methods, which is coherent with earlier studies.1,–,3 More important, our data show that approximately 40% of extremely low gestation age infants had a completely normal cUS at term age and that none of these infants had moderate or severe WM abnormalities or abnormal grey matter on conventional MRI. Consequently, all infants with normal cUS have either a normal MRI (64%) or only mild (36%) WM abnormalities on MRI.
This raises the question of whether mild WM abnormalities on MRI found in one-third of infants are of clinical relevance; does the knowledge about these mild WM abnormalities change our clinical decision making and/or parental counselling?
Woodward et al demonstrated that infants with mild WM abnormalities had a 7.2 points lower mean mental developmental index (MDI) and a 3.9 points lower mean psychomotor developmental index (PDI) score compared to infants with normal WM.4 However, the specificity for predicting severe cognitive and motor delay, cerebral palsy and neurosensory delay decreased from 82% to 84% (for moderate to severe WM abnormalities) to 30% to 31% when all WM abnormalities, including mild WM abnormalities, were taken into account. Considering that these data were acquired in centres of excellence in neonatal MRI, it must be assumed that sensitivity and specificity might be reasonably lower in centres with less experience in neonatal MRI.
From our results, we hypothesise that in infants with normal cUS at term age, conventional MRI adds marginally clinically relevant information. Consequently, it is unlikely in this group of infants that MRI at term age will change clinical decision making or parental counselling. This implies that ultrasound can be used as a screening method to identify infants with low risk of severe disability and thereby reduce the number of MRIs. This is important as MRI is, at this moment, an expensive technique with limited access that sometimes also presents logistical challenges (transport, sedation).
Nevertheless, it has to be emphasised that our results refer to conventional MRI in preterm infants at term in a clinical setting only. The high impact of neonatal MRI in a research setting is certain and undisputed. Conventional MRI and more advanced MRI methods (including image postprocessing techniques) such as diffusion tensor imaging, volumetry, tractography, MRI spectroscopy and functional MRI have and will greatly enhance our knowledge about the physiology and pathophysiology of the developing newborn brain.9 13,–,16 Implementing these more advanced techniques into the clinical setting might improve the information gained by an MRI at term age in the future.
One limitation of the study is that cUS was performed through the anterior fontanel only. Ultrasound examinations that add the view through the posteriolateral and posterior fontanel to the view through the anterior fontanel have been found to be superior in the detection of posterior fossa abnormalities.17 18 In our study four infants had small punctate cerebellar haemorrhages not seen on cUS but diagnosed on MRI images.
A strength of the present study is that we compare cUS and conventional MRI performed on the same day at term age. Furthermore, the cohort is population based, thus, the data represent the true spectrum of brain abnormalities in the high-risk group of ELGA infants. Moreover, we focus on clinical point of view in order to determine the clinical advantages of MRI compared to the cheaper and faster ultrasound examination in daily routine.
In conclusion, we compared cUS and conventional MRI performed on the same day at term age in ELGA infants and suggest that, in a clinical setting, cUS can be used as a screening method to identify infants in whom conventional MRI adds marginally clinically relevant information to the cUS result.
References
Supplementary materials
Web Only Data adc.2009.161547
Files in this Data Supplement:
{kind=link}
Footnotes
-
Funding The present study was supported by the following grants: ESPR Young Investigator Exchange Program, Jerring Foundation, Sällskapet Barnavård, Märta och Gunnar V Philipsson Foundation, Swedish Medical Research Council, Foundation Samariten, Free Masonry Foundation Barnhuset in Stockholm, Åke Wiberg Foundation, Jeansson Foundation, Karolinska University Hospital. These funding sources financed the research activity of SH and BS.
-
Competing interests None.
-
Ethics approval The study was approved by the regional ethical committee in Stockholm, Sweden.
-
Provenance and peer review Not commissioned; externally peer reviewed.