Article Text

Abstract
Background: Pasteurellosis is an uncommon infectious disease in humans mainly caused by Pasteurella multocida infection in neonates and has been rarely reported.
Objectives: To review the literature and address the mode of transmission, clinical presentation, laboratory diagnosis, treatment, outcome and potential risk factors related to neonatal pasteurellosis.
Methods: A Medline all-languages database search for neonatal (birth–1 month) pasteurellosis cases after 1950 was conducted. Individual references from each publication were also reviewed to identify additional cases.
Results: Thirty-two cases were found, but detailed information was available for this review in only 25 cases. The median age was 14 days (range: birth–30 days). All were infected with P multocida. Animal exposure to cats and/or dogs was the major risk of infection: non-traumatic exposure in 11 (44%) cases, and traumatic exposure in 2 (8%) cases. Infections in 11 (44%) cases were classified as vertical transmission. The clinical features were most commonly bacteraemia with or without meningitis. The age at onset of 72 h or older was significantly associated with meningitis (⩾72 h of age: 13/14 vs <72 h of age: 3/11, p = 0.002). The most used antibiotics were β-lactam with or without aminoglycoside or chloramphenicol. The overall mortality was 20% (5/25). The age at presentation of <72 h, birth weight of <2500 g, and vertical transmission were independently associated with death.
Conclusion: Pasteurellosis is a rare bacterial infection in neonates and should be considered in the cases of sepsis with history of exposure to domestic animal in either the patient or the mother.
Statistics from Altmetric.com
Pasteurellosis is an uncommon infectious disease in humans and caused mainly by Pasteurella multocida.1 2 Pasteurella spp. is Gram-negative coccobacilli oral flora found in many kinds of animals, especially cats (70–90%), dogs (50–66%) or pigs (51%).1 P multocida infection in neonates is a serious systemic disease, leading to meningitis, septicaemia, pneumonia, conjunctivitis, and osteoarticular infection.3 4 5 6 7 8 9 10 11 12 13 14 15 16 17 18 19 20 21 22 23 24 25 26 27 The infections are mostly acquired through scratches and bite wounds from domestic animals.1 28 Vertical transmission is another route of infection reported in neonates.4 5 8 11 12 13 15 16 17 24 27
This article reviewed the literature of neonatal pasteurellosis from 1953 to the present, to address the mode of transmission, clinical presentation, laboratory diagnosis, treatment, outcome and potential risk factors related to mortality.
What this study adds
Sepsis and meningitis are common in neonatal pasteurellosis. Most of the infections in neonates occurred without traumatic exposure to domestic animals.
Early-onset sepsis, birth weight, and vertical route of infection are significant factors related to mortality in neonatal pasteurellosis.
Methods
We searched the PubMed bibliographic database (US National Library of Medicine, Bethesda, Maryland, USA) in the period of 1950 to March 2008 using the key words “newborn: birth-1 month”, “pasteurellosis”, “pasteurella infection” and “Pasteurella spp.”, with no language restrictions. After this initial series of reports was reviewed, the individual references listed in each publication were again reviewed to find additional case reports.
For this analysis, diagnosis of a definite case of pasteurellosis required isolation of Pasteurella spp. in organ(s) and/or body fluid in a neonate. Vertical transmission was defined as documented evidence of Pasteurella spp. infection in organ(s) and/or body fluid in the mothers, and/or the patients developed pasteurellosis within 72 h of age and without history of neonatal exposure to animals. Traumatic exposure was defined as being bitten or scratched by the animals, and non-traumatic exposure was defined as direct contact and/or indirect contact with animals without evidence of bite or scratch. The demographic parameters, clinical presentations, treatments and outcomes of the patients were collected from each case report, and extracted onto a data extraction form by two independent investigators (N. Narongwit and A. Thitiya). Relevant data from French and German language articles were extracted in the presence of a translator. The SPSS program (V.11.5, SPS Inc, Chicago, Illinois, USA) was used to develop a database of categorical and continuous variables. Statistical evaluation of differences in proportions was performed by Fisher’s test. A p value of less than 0.05 indicated statistical significance.
The Hat Yai Research Ethics Committee was contacted and declared that no ethical approval was required for this research.
Results
A total of 32 cases were identified in the original search, but detailed clinical data were available of the analysis in only 25 cases. The earliest case was reported in 1953, and the last case reported in February 2008. Table 1 summarises the main features of the 25 reported neonatal cases. All were infected by P multocida.
Demographic and clinical characteristics of 25 reported cases of neonatal pasteurellosis sorted by year of publication
Mode of transmission
Of the 25 reported cases, 23 reported the information of animal exposure. Non-traumatic animal exposure was a major risk of infection, and was reported in 11 (44%) cases (six, two and three cases exposed to cats, dogs and both, respectively). Traumatic animal exposure was reported in two cases, one of those (case 8) had developed meningitis and brain abscess following a dog bite at the scalp, while another (case 16) was bitten by a cat, resulting in scalp injury (table 1).
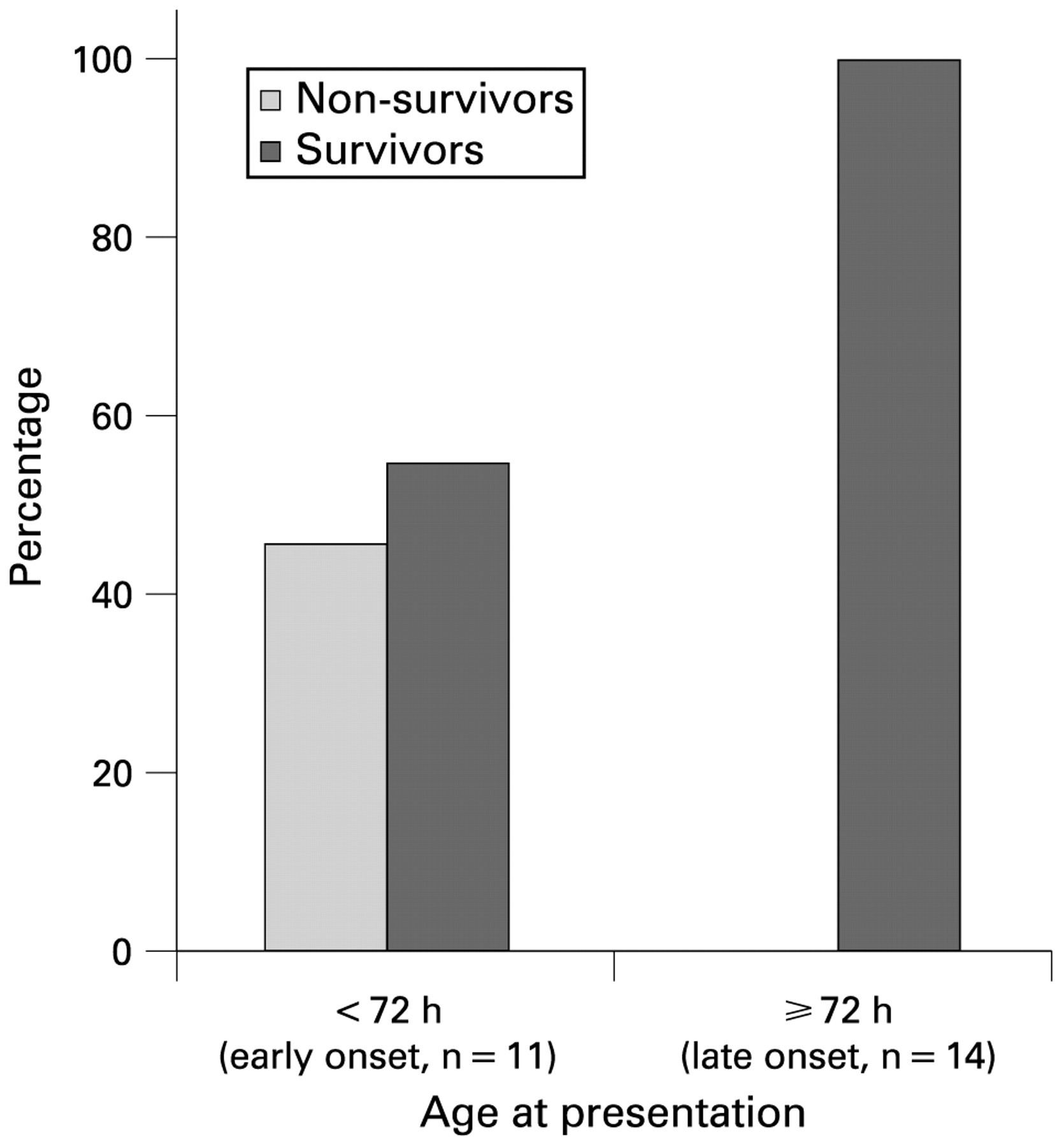
As shown in table 1, 11/25 cases (44%) were from vertical transmission. Five of 11 cases (45%) with onset before 72 h of life died, while no patients (0/14) with onset after 72 h of life died (fig 1). The mothers of eight cases had a positive culture for P multocida in body fluid, and all had history of cats and/or dogs exposure (traumatic exposure to cats or dogs in three cases (cases 3, 10 and 13), and non-traumatic exposure in five cases (cases 6, 9, 11, 14 and 15)) (table 1). Of these, four had a positive vaginal culture (cases 10, 11, 14 and 15), two had positive vaginal and blood cultures (cases 6 and 13), one had positive amniotic fluid culture (case 9) and one had positive endometrium culture (case 3). The other three cases with vertical transmission (cases 2, 22 and 25) had no evidence of maternal infection, but without evidence of animal exposure in the neonates before the onset of within 72 h of age. Of these, only the mother of case 25 had history of exposure to dog.
{kind=link}
Distribution of age at presentation with early and late onset of neonatal pasteurellosis (n = 25).
Clinical presentations
The clinical presentations of neonatal pasteurellosis were typical for neonatal sepsis. The common signs and symptoms were fever (20/25, 80%), and irritability/lethargy (18/25, 72%). The most common clinical diagnosis was bacteraemia with meningitis (12/25 cases, 48%), followed by bacteraemia only in four cases (16.0%), and meningitis only in four cases (16.0%). Other sites of infection were pneumonia (three cases), osteomyelitis (two cases) and conjunctivitis (one case) (table 2). Meningitis was found in 13 of 14 (93%) cases with age of onset of ⩾72 h, significantly higher than in those with age of onset of <72 h (3/11 cases, 27%, p = 0.002).
Characteristics of 25 reviewed cases of neonatal pasteurellosis
Laboratory diagnosis
A white blood cell (WBC) count was reported in 19 cases (median: 10 690 cell/mm3, range: 1500–35 600 cell/mm3), and the median percentage of polymorphonuclear cells was 59% (range: 10–84%). Of the 20 cases that reported having blood culture, 17 were positive and three were negative. Five cases were not mentioned.
Of 25 reported cases, 18 underwent lumbar puncture, while four (cases 1, 6, 13 and 25) were not reported, and three (cases 3, 9 and 11) died without lumbar puncture. Of these, two had normal cerebrospinal fluid (CSF) examination (cases 14 and 22), and 16 were diagnosed with meningitis. The detailed CSF examinations were available in 13 diagnosed meningitis cases. The median WBC count in CSF was 4780 cells/mm3 (range: 0–11 200 cells/mm3), and the median percentage of polymorphonuclear cells was 83% (range: 0–92%). Gram stain findings of CSF specimens revealed Gram-negative coccobacilli or bacilli in 10 cases. The organism was isolated from CSF in 14/16 (88%) cases. Another two cases (cases 19 and 21) reported a pleocytosis with negative CSF culture probably due to partial treatment. One case (case 12) reported no WBC in CSF but had a positive CSF culture for P multocida.
Treatment
Treatment of P multocida infection in reported cases was mainly antibiotic therapy. Surgical debridement of the brain and fractured skull was required in one case (case 8) following a penetrating injury from a dog bite. The doses and durations of antibiotic therapy of reported cases were not specified. The most frequently used antibiotics were ampicillin (16 cases), aminoglycoside (16 cases) and cefotaxime (11 cases) (table 1).
Outcome
Of the 20 survived cases, 11 cases (case 4, 7, 8, 15, 16, 18, 19, 20, 21, 24 and 25) were completely recovered at the end of follow-up (4–22 months), four cases (case 5, 6, 10 and 12) reported clinical normal at discharge from hospital, and five cases (case 1, 13, 14, 17 and 23) were not reported.
Five cases died, resulting in an overall mortality rate of 20% (table 2). In univariate analysis of factors potentially associated with death, age at presentation of <72 h, birth weight of <2500 g, and vertical transmission were found to be associated with death (p = 0.009, 0.009 and 0.011, respectively, table 3).
Univariate analysis for risk factors associated with death in neonatal pasteurellosis
Discussion
This is the first published review of pasteurellosis in neonates. We found that P multocida was the only species reported. Most cases presented with bacteraemia with or without meningitis. The mortality rate of neonatal pasteurellosis was 20%, and the age at presentation, birth weight, and vertical transmission were significantly associated with death.
Pasteurella spp is known to infect humans, and P multocida is the most common pathogen organism.1 28 Diagnosis of pasteurellosis required isolation of the organism from cultures. Pasteurella grows readily on blood agar and generally appears as Gram-negative coccobacilli, therefore, was sometimes mistaken for Hemophilus spp.29 P multocida was the cause of 75–100% of cat bite wound infection and 50–55% of dog bite wound infection.2 28 Half of all neonatal reported cases had a history of exposure to domestic animals. We found that non-traumatic exposure was more common than traumatic exposure in neonatal infection. We hypothesise that contact of respiratory droplets from animals was likely the route of infection in non-traumatic exposure cases. The organism has been known to be transmitted through animal saliva without a bite or scratch.30
This review showed that vertical transmission is an important route of infection in the neonatal population, and was a significant factor associated with death. This study found that eight of 10 mothers of infants with vertical transmission had P multocida infections in blood and/or genital tract fluid including placenta. Transplacental haematogenous infection, particularly intrauterine transmission, and infection in the mother at time at birth can play a significant role in the development of infection in the neonates.31 32
The presenting features of P multocida infection in neonates were sepsis-like. Similar to other neonatal bacterial sepsis, neonatal pasteurellosis could be classified into early- and late-onset forms. The results of this study revealed that early onset (age at presentation within 72 h of age) was associated with death, and less likely involved the central nervous system (CNS) than late onset. The neonates with early onset had more severe infection and might have died before the lumbar puncture was performed, and missed the diagnosis of meningitis. The neonates with late onset, could be from a smaller inoculum amount of bacteria, had a longer time to offset the infection and allow dissemination of bacteria to multiple organs including the CNS, similar to other late-onset neonatal sepsis.31 When compared with a report of Kimura et al,33 in which the majority of patients were adults, the proportion of CNS infections in neonates was higher (64% vs 14%, respectively). Cellulitis was the most common clinical presentation in adults. Immature immunity could explain the more severe form of infections in neonates.31 32 34
The antibiotic therapy of choice for pasteurellosis in children is penicillin. In neonates, a high dose of penicillin should be used to treat CNS infections. Aminoglycoside should also be administered for synergistic mechanisms. The recommended duration of treatment was 7–10 days for local infections, and extended to 2 weeks for neonatal bacteraemia and meningitis. Treatment of bone and/or joint infections should be 4–6 weeks. Surgical drainage or debridement may be necessary in patients with site abscess or bite wound.35
Our study found that age at presentation of <72 h, birth weight of <2500 g, and vertical transmission were independent factors associated with mortality. This result was similar to other bacterial neonatal sepsis in that early-onset and low birth weight infants had a higher mortality rate.31 32 Furthermore, vertical infection may have a higher inoculum size and therefore cause a more serious infection.
In conclusion, neonatal pasteurellosis was a rare infectious disease, but with a relatively high mortality rate. We hope this report alerts general paediatricians and neonatologists to consider pasteurellosis as a possible cause of sepsis in neonates, especially in patients and mothers with a history of domestic animal exposure.
Acknowledgments
The authors thank Mr David Patterson for editing the manuscript.
REFERENCES
Footnotes
Competing interests None.