Article Text

Abstract
Background: Extracorporeal membrane oxygenation (ECMO) remains the mainstay of management in neonates with severe but potentially reversible respiratory failure. In the UK, ECMO is available only as a supraregional service at four centres.
Objective: To explore regional variations in ECMO referrals and neonatal deaths due to severe respiratory failure in England, Wales and Northern Ireland.
Methods: In this retrospective study, data regarding ECMO referrals due to neonatal respiratory failure from January to December 2002 were obtained from the four UK ECMO centres and then subdivided according to the Government Office Regions. Anonymised data regarding neonatal deaths was obtained from Confidential Enquiry into Maternal and Child Health. Neonatal deaths were classified into four groups (group 1: deaths potentially avoidable by ECMO; group 2: deaths where it was unclear whether ECMO would have been of benefit; group 3: neonates not eligible for ECMO; and group 4: data inadequate to classify deaths).
Results: There was significant regional variation in the rates of both ECMO referral (0.10 to 0.46 per 1000 live births; (p<0.001)) and neonatal deaths (groups 1 and 2) (0.09 to 0.32 per 1000 live births; (p<0.001)). Regions with high referral rates for ECMO tended towards having higher group 1 plus group 2 neonatal death rates (correlation coefficient = 0.75).
Conclusion: It is possible that there are significant regional variations in the uptake of ECMO and in neonatal mortality due to severe respiratory failure. A confidential prospective study may further clarify these observations and identify the factors that might lead to these variations.
Statistics from Altmetric.com
The UK neonatal ECMO trial left little doubt about extracorporeal membrane oxygenation (ECMO) treatment as lifesaving for near term infants with acute respiratory failure (ARF).1 Clinical trials of ECMO-sparing treatments such as inhaled nitric oxide, surfactant and high-frequency oscillation, following the UK ECMO trial, suggest that ECMO remains the only option for some infants with ARF.2–6 The advent and widespread introduction of these “ECMO-sparing treatments” and the uncertain role of ECMO in managing infants with ARF secondary to congenital diaphragmatic hernia (CDH)7 has introduced a degree of uncertainty with regard to determining which children can be safely managed with non-ECMO treatments and which children are best managed in an ECMO centre.
The present study aimed to explore:
regional variations in the extent to which eligible newborn infants (<29 days of age) with ARF were referred for ECMO treatment
regional variations in rates of death among neonates potentially eligible for ECMO;
the relationship between regional patterns of ECMO referral and regional rates of death among neonates potentially eligible for ECMO.
METHODS
Box 1 Classification of deaths according to predefined criteria
Group 1
Neonatal deaths potentially avoidable by ECMO treatment
Neonates >35 weeks’ gestational age or >2.5 kg birth weight or with isolated CDH (>35 weeks gestational age or >2.5 kg birth weight) with none of the following:
a major cardiac defect;
a major chromosomal abnormality or congenital malformation;
an intraventricular haemorrhage.
Group 2
Neonatal deaths where it is unclear whether ECMO treatment would be of benefit
Neonates between 32 and 35 weeks’ gestational age and/or birth weight 2–2.5 kg with or >35 weeks’ gestational age/>2.5 kg birth weight with any of the following:
intraventricular haemorrhage;
sepsis and profound shock;
death within 6 h of birth;
data not clear to classify death.
Group 3
Neonates not eligible for ECMO
Neonates <32 weeks’ gestational age and/or weighing <2 kg at birth or >32 weeks’ gestational age/>2.5 kg birth weight with any of the following:
untreatable and major cardiac malformation where ECMO is not indicated (such as hypoplastic left heart syndrome), major chromosomal abnormality and/or untreatable congenital malformation (such as lung agenesis);
severe hypoxic ischaemic encephalopathy.
Group 4
Data not adequate to classify deaths
No data available.
ECMO referral pattern
For reasons of patient confidentiality, we obtained anonymised data regarding ECMO referrals for neonatal respiratory failure from the four UK ECMO centres (Glenfield Hospital, Leicester; Freeman Hospital, Newcastle; Great Ormond Street Hospital for Children, London; and the Royal Hospital for Sick Children, Glasgow) for the period January–December 2002. We subdivided the data according to the Government Office Regions, on the basis of the relevant child’s address. The regions used were: North East England, North West England, Yorkshire and the Humber, West Midlands, East Midlands, East of England, South West England, Greater London, South East England, Wales and Northern Ireland. To further preserve data anonymity, these regions were randomly coded 1–11. Regions 1, 3 and 4 have an ECMO centre. Referred patients who were eligible for ECMO and were accepted for ECMO were included in the analysis of outcome irrespective of whether they received ECMO treatment. The rate of referral for ECMO per 1000 live births was determined by using the number of births for the study period reported by the Office of National Statistics (ONS).
Neonatal mortality
We obtained anonymised data on all neonatal deaths in England, Wales and Northern Ireland during for the study period from the Confidential Enquiry into Maternal and Child Health (CEMACH). Data on neonatal mortality from Scotland were not available and hence these were excluded from this study.
For each death it was agreed the following data would be provided: birth weight; gestational age; main fetal disease or conditions; other significant fetal disease or conditions; Wigglesworth classification of neonatal death; fetal and infant classification of neonatal death; obstetric (Aberdeen) classification of neonatal death; geographical region of neonatal death; and age at death. On the basis of these data items, the deaths were classified into one of four groups as defined in box 1. The deaths were classified independently (RT and HP) and discrepancies were discussed with a third observer (DF) to arrive at a consensus. One region (region 10) had very few deaths in group 1, a large number of deaths in group 2 and a high proportion of data regarding cause of death that could not be classified (111/180). Data from this region are shown but are excluded from the statistical analyses. Deaths due to the diagnoses (table 1) that could lead to severe ARF were presumed to be due to severe respiratory failure and eligible for ECMO. Once classified, we determined the neonatal death rates (per 1000 live births) by region of death using birth rate data provided by the ONS.
Statistical methods
Rates of referral and death are expressed as rates per 1000 live births, with 95% confidence intervals. For each outcome overall differences between regions were investigated using Poisson log-linear models. The relationship between regional death rates and referral rates was quantified using the Pearson correlation coefficient (r). A 95% confidence interval was estimated for r using re-sampling methods. SAS version 8.2 was used for all analyses.
RESULTS
Regional variations in EMCO referrals
During the study period, 469 neonates born in England, Wales and Northern Ireland were referred to the four UK ECMO centres (Leicester 206; London 174; Newcastle 72; Glasgow 17). Of these referrals 288 (61.4%) were accepted for ECMO. The region-wise survival of neonates accepted for ECMO (irrespective of whether the neonate received ECMO) are presented in table 2. The overall survival rate of accepted referrals was 71% (table 2). The ECMO referral rate per 1000 live births including and excluding CDHs varied between the regions, ranging from 0.10 to 0.46 (p<0.001) (table 3). There was no significant difference in the proportion of ECMO referrals accepted when regions with ECMO centres were compared with regions without an ECMO centre (63% and 61%, respectively p = 0.65).
Regional variations in death rates among neonates potentially eligible for ECMO
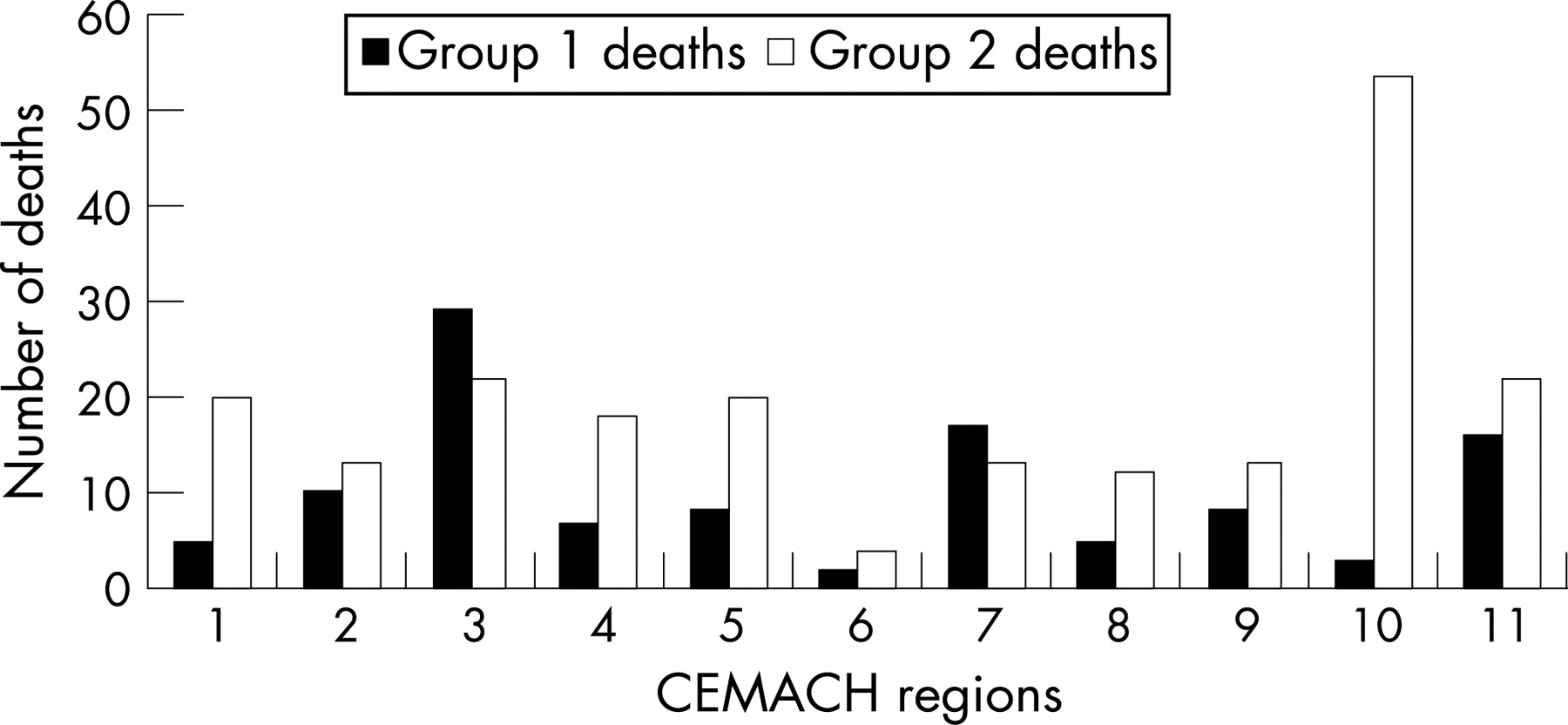
Over the study period, 6905 neonates died in England, Wales and Northern Ireland. Of these, 6405 would not have been eligible for ECMO (group 3) and there were insufficient data to classify another 180 (group 4). The deaths of the remaining infants were judged to probably or possibly avoidable by ECMO (110 group 1 and 210 group 2). Table 4 presents group 1 and 2 group deaths according to classification of neonatal deaths by CEMACH region. Figure 1 shows the number of deaths in these groups by region of death.
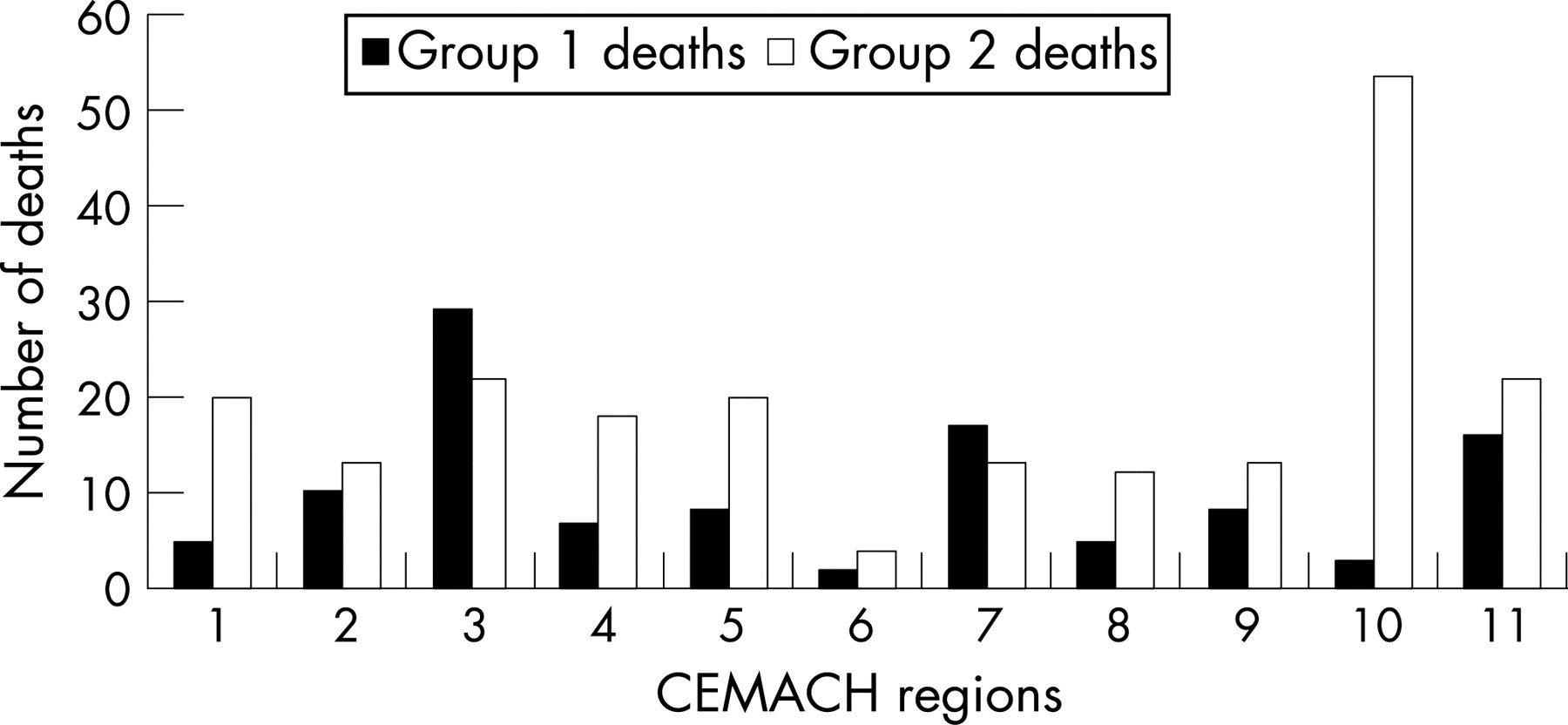
There was considerable variation between the regions in terms of death rates per 1000 births especially for group 2 deaths (p<0.001) as well as the combined rate of deaths in group 1 and group 2 (p<0.001 including and excluding CDHs) (table 4).
Relationship between regional patterns of ECMO referral and regional death rates among neonates potentially eligible for ECMO
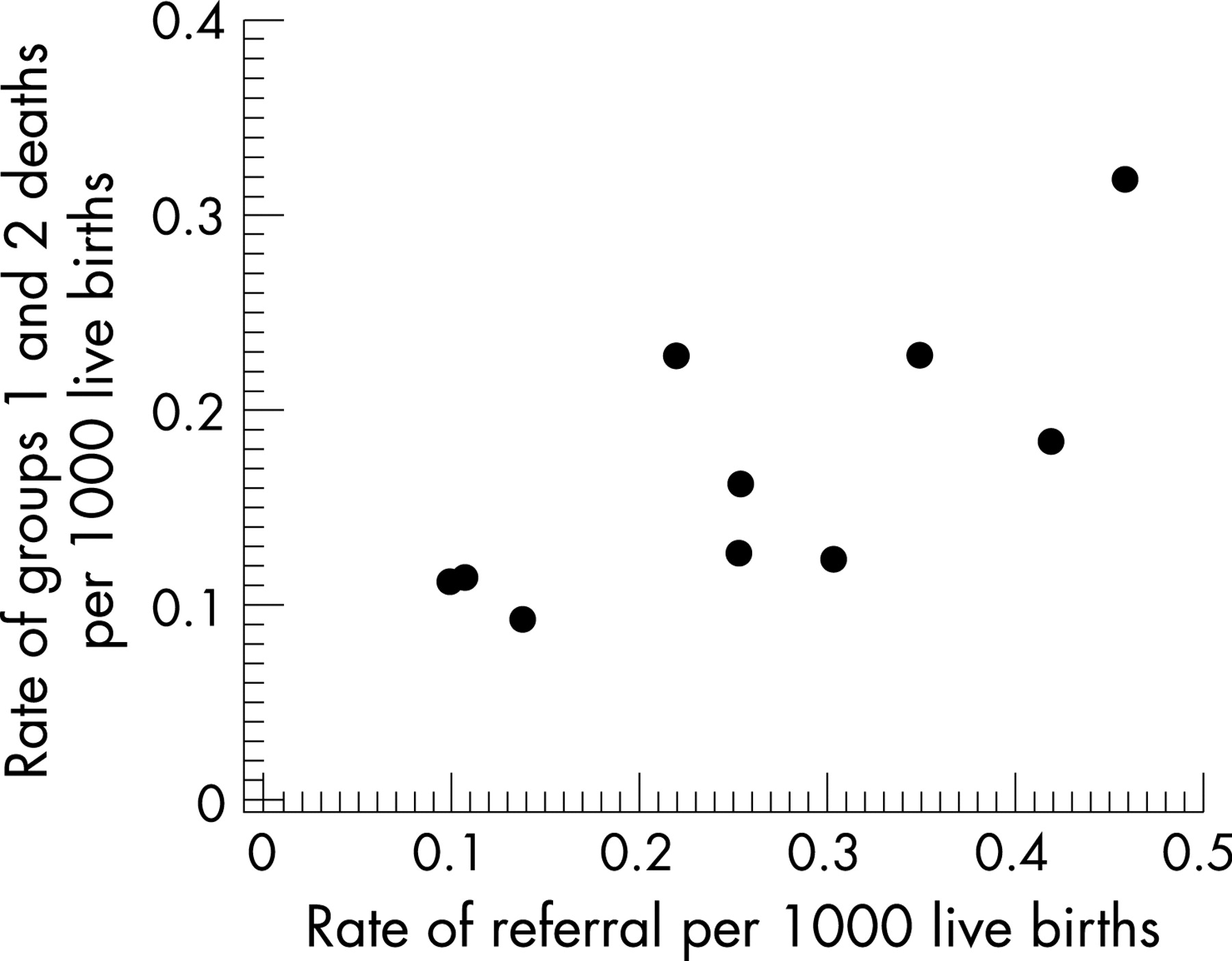
Regions with high rates of referral (per 1000 live births) for ECMO tended towards having higher combined (group 1 plus group 2) neonatal death rates (correlation coefficient r = 0.75 (95% CI 0.31 to 0.87), excluding region 10) (fig 2). The correlation was similar even if infants with CDH were excluded from the analysis (r = 0.77 (95% CI 0.32 to 0.88)).

{kind=link}
{kind=link}
DISCUSSION
What is already known on this topic
Extracorporeal membrane oxygenation (ECMO) is the mainstay of management in neonates with severe acute respiratory failure.
In the UK, ECMO is provided as supraregional service.
What this study adds
There are significant regional variations in the uptake of ECMO as a supraregional service and in neonatal mortality due to severe respiratory failure.
This study aimed to describe regional variation in ECMO referral rates in the UK and neonatal mortality rates for infants who might potentially have benefited from ECMO, and to explore the relationship between these rates. We have identified apparently quite marked variation in both these rates between the regions. Before considering possible interpretations for these findings, we first discuss some important limitations of the data.
There were some important gaps in the data available to us. Our information about the neonatal deaths was based on where the infant died rather than their place of residence or birth. In addition, we did not have information about neonatal mortality in Scotland, and we had to exclude one region with restricted information about the cause of death. Also, to comply with conditions of confidentiality, the study was based on anonymised data aggregated at regional level. We therefore could not use detailed information to explore explanatory variables at the level of individual infants. The results may therefore exhibit the so-called ecological fallacy, which assumes that all members of a group (region) exhibit characteristics of the group at large.8
We used the classifications of deaths as imperfect proxies for the clinical conditions that may have led to referral for ECMO or otherwise, but we recognise that this is post hoc information rather than reflecting the exact situation facing neonatologists at the point at which they might be considering referral. Also, by using deaths within 28 days of birth as proxy for referral in the neonatal period we may have missed potential referrals within the 28 days who died in the post-neonatal period. It is, however, unlikely that these issues would vary systematically between regions. There may also be some specific misclassification of deaths as data quality in relation to diagnoses on death certificates and diagnostic categories entered in CEMACH forms may vary between individuals in different health regions. We are, however, unaware of any systematic bias in reporting that could account for the scale of difference in neonatal death rate seen in this study.
Our study showed a 4.5-fold variation in the proportion of neonates referred by Government Office Regions for ECMO treatment, which raises the possibility that variation in service provision and/or access to specialist care may be a factor. The rate of referral for ECMO seems most likely to have been influenced by: (a) the number of babies reaching ECMO referral criteria (and hence a reflection of obstetric and neonatal care) and (b) the extent to which local neonatologists caring for those infants felt that such a referral was both in the best interests of the child and feasible in terms of ease of transfer. ECMO is an important example of this phenomenon as the evidence relating to its use is quite clear, especially in relation to infants without diaphragmatic hernia. What is not clear from these data is the extent to which these factors (ie environment vs the care package) were responsible for the variation in deaths in groups 1 and 2.
During the 3-year study period, almost 7000 neonatal deaths were recorded in the CEMACH database in a total birth cohort for the whole the England, Wales and Northern Ireland of nearly 1.86 million, and the neonatal death rate varied by a factor of 2 (2.7–5 deaths per 1000 births) between the Government Office Regions.9 Variations in UK regional neonatal death rates have been recognised for some time and have been attributed to a variety of factors.10 However, this is the first study to show that this variation may be associated with regional differences in the uptake of a particular intervention.
It is difficult to monitor the uptake of the UK ECMO supraregional service. A prospective study of infants meeting criteria for ECMO within one or two regions may clarify the extent of the correlation between ECMO referral rates and neonatal mortality rates for infants who might potentially have benefited from ECMO, but more importantly could highlight whether other “care”-related issues are responsible for some of the variation in neonatal mortality that exists in the UK.
Acknowledgments
We thank CEMACH for providing the data on neonatal deaths, ONS for providing the data on live births; and ECMO centres for providing the data on ECMO referrals.
REFERENCES
Footnotes
Competing interests: RT, HP, JS and ID are clinicians involved in ECMO.
Ethics approval: The Central Office for Research Ethics Committees (COREC) at Central Manchester Local Research Ethics Committee approved the study. The ethics committee requested formation of a formal independent steering group consisting of both clinical and epidemiological experts to review the protocol, discuss progress and approve any dissemination.
Linked Articles
- Fantoms