Article Text

Abstract
Background Management of pneumothorax in neonates requiring retrieval poses unique challenges, including decision to insert an intercostal catheter (ICC). We aimed to report the proportion and characteristics of neonates transported with and without ICC insertion and the incidence of deterioration in neonates transported with pneumothorax.
Methods A retrospective cohort study of neonates transported with pneumothorax between 2016 and 2020 in Victoria, Australia. Univariate analysis was performed on patient and clinical characteristics, followed by multivariate analysis to identify risks independently associated with ICC insertion.
Results 174 neonates were included. Mean (SD) gestational age (GA) was 37.5 (2.8) weeks. Eighty-two neonates (47%) had ICC inserted. On multivariate analysis, risk factors independently associated with ICC insertion were mechanical ventilation (MV) preceding retrieval team arrival (OR 12, 95% CI 3.1 to 46.6, p<0.001) and radiographical mediastinal shift (MS) (OR 6.2, 95% CI 2.4 to 16.2, p<0.001). Increasing GA is negatively associated with ICC insertion (OR 0.66, 95% CI 0.5 to 0.8, p<0.001). No significant difference in incidence of deterioration between the ICC group and the no-ICC group was observed (8.5% vs 5.4%, p=0.55). Ninety-five neonates were treated with needle aspiration (NA); 40 (42%) subsequently avoided ICC insertion. Twelve (13%) neonates transported without ICC had insertion within 24 hours following transport.
Conclusion Many neonates with pneumothorax are transported without ICC, with low incidence of deterioration and ICC insertion within 24 hours after transport. More than a third of neonates managed with NA avoided ICC insertion. The likelihood of ICC insertion is increased by lower GA, MV prior to retrieval team arrival and radiographical MS.
- Neonatology
- Intensive Care Units, Neonatal
- Emergency Care
Data availability statement
All data relevant to the study are included in the article or uploaded as supplementary information.
Statistics from Altmetric.com
WHAT IS ALREADY KNOWN ON THIS TOPIC
Approximately 45% of neonates with pneumothorax in the neonatal intensive care unit can be initially managed without intercostal catheter (ICC) insertion.
Up to 78% of neonates requiring retrieval with pneumothorax have an ICC inserted prior to transport.
WHAT THIS STUDY ADDS
Many neonates with pneumothorax are retrieved without ICC insertion, with low incidence of deterioration in transport and subsequent need for ICC within 24 hours.
Needle aspiration prevents ICC insertion prior to transport in a selected group of neonates.
Lower gestational age, need for mechanical ventilation preceding retrieval team arrival and presence of radiographical mediastinal shift are associated with increased likelihood of ICC insertion prior to transport.
HOW THIS STUDY MIGHT AFFECT RESEARCH, PRACTICE OR POLICY
This study demonstrates that there is a clinically important group of neonates with pneumothorax who can be transported without ICC insertion.
This highlights an opportunity to improve practice by reducing the insertion of an ICC in a carefully selected group.
Using preliminary data from this study, a risk scoring tool could be developed and validated to guide retrieval clinicians in the decision to insert ICC prior to transport.
Background
Pneumothorax, a collection of air in the pleural space, occurs in up to 9.2% of neonates in the neonatal intensive care unit (NICU).1 2 Although most pneumothoraces are associated with risk factors including hyaline membrane disease, meconium aspiration syndrome, transient tachypnoea of newborn, pulmonary hypoplasia or positive pressure ventilation (PPV), some occur spontaneously in the absence of primary lung disease.1 3 4 Pneumothorax can cause respiratory and haemodynamic compromise, and is associated with intraventricular haemorrhage, prolonged hospitalisation and death.1 2 Consequently, prompt recognition and management are critical.
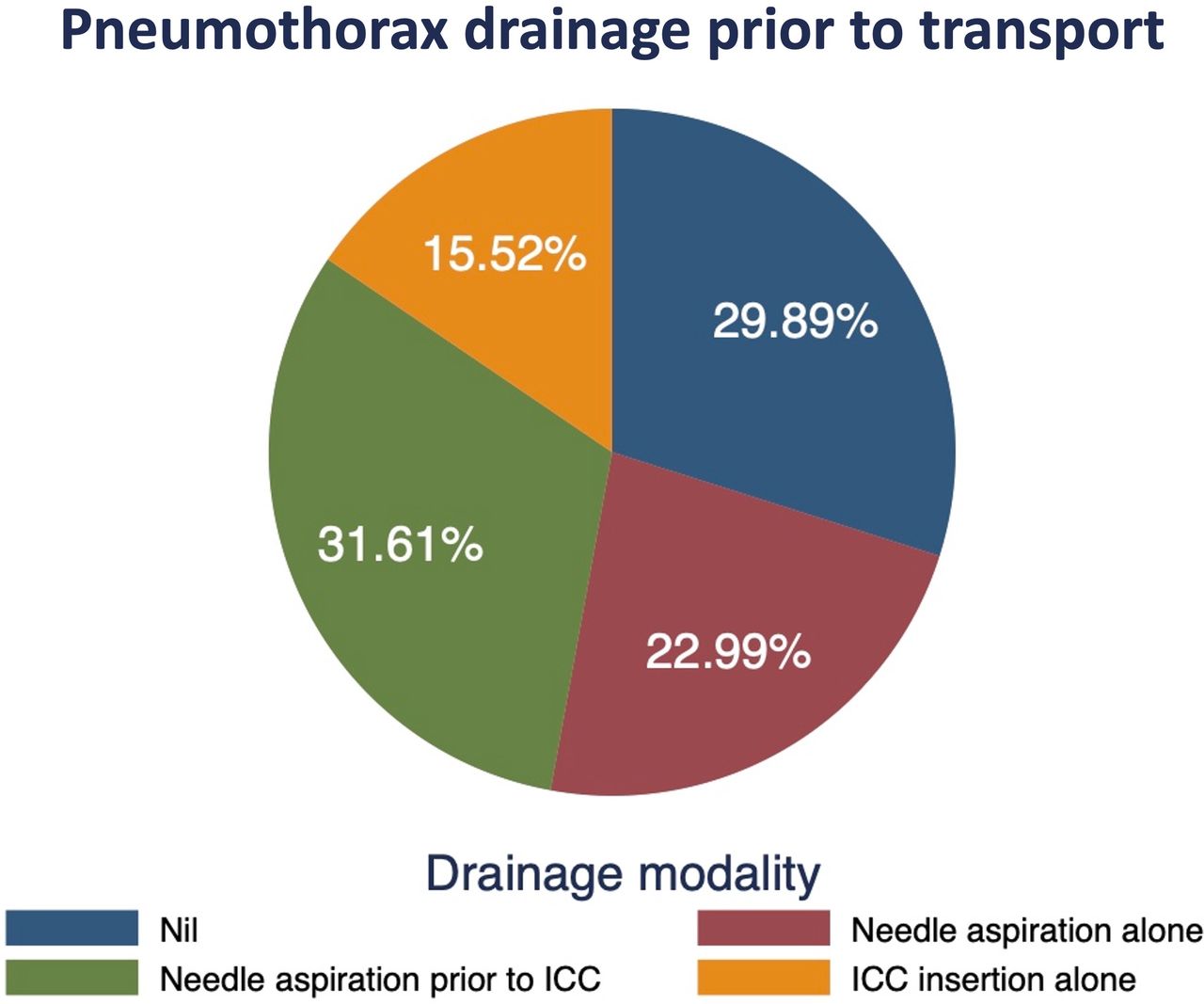
Options for management of neonatal pneumothorax include (1) conservative management with no drainage, (2) drainage with needle aspiration (NA) by temporary insertion of a needle into the pleural space5 or (3) definitive drainage by insertion of an intercostal catheter (ICC) left in situ until resolution of the air leak.4
Clinicians decide on treatment strategy based on severity of clinical signs, radiographical features, comorbidities and level of respiratory support required. Pneumothorax can expand, so a pneumothorax initially managed conservatively could rapidly require ICC insertion. Recent evidence indicates that up to 45% of neonates with pneumothorax in NICUs can be initially managed without ICC insertion.6 7 The use of NA as initial treatment reduces the need for ICC insertion in the NICU environment.8 9
In retrieval, pneumothorax management requires additional logistic and safety considerations. Retrieval clinicians must decide on a treatment strategy during initial stabilisation, considering clinical factors, available resources and anticipated transport conditions. Aeromedical retrieval poses a further challenge, as increasing altitude and reduction in atmospheric pressure causes expansion of trapped gas,10–12 an effect which varies by the type of aircraft due to differences in cabin pressurisation.13
Insertion of ICC mid-transport is practically challenging. It is therefore not surprising that more neonates with pneumothorax requiring retrieval have ICC inserted compared with those in NICUs.14 However, ICC insertion is time-consuming, invasive, and associated with risk of complications including pain, bleeding and scarring.15–17 In Australia, primary transport clinicians are commonly neonatal trainees. Given conservative management of pneumothorax is now common in NICU18 and neonatal trainees less frequently insert ICCs,19 procedural inexperience is increasing. In view of these risks, insertion of ICC in retrieval needs to be considered in the context of anticipated benefits.
The Paediatric, Infant and Perinatal Emergency Retrieval (PIPER) service is an emergency retrieval service based at the Royal Children’s Hospital (RCH), Victoria, Australia. PIPER provides specialist advice and retrieval services for unwell neonates in Victoria. Approximately 1400 emergency retrievals are conducted annually of infants ranging from birth to 8 weeks’ corrected age. Transport is undertaken by ambulance, rotary-wing (helicopter) or fixed-wing flight. Rotary-wing flights are non-pressurised, while fixed-wing flights are pressurised to a maximum of 500 feet above mean sea level. PIPER retrieves approximately 50 neonates with pneumothorax annually.
There are no published data on treatment strategies for neonates with pneumothorax requiring retrieval. Adults with traumatic pneumothorax can be transported in non-pressurised aircraft without ICC insertion.20 Increasing evidence supporting treatment without ICC insertion in the NICU, combined with limited research specific to neonatal retrieval indicates a need to better understand which neonates are transported safely without an ICC.
Aims
We aimed to report the proportion and characteristics of neonates transported with and without ICC insertion, incidence of in-transport deterioration, proportion of neonates treated with NA and those transported without ICC who have one inserted within 24 hours of transport. Further, we aimed to undertake exploratory analysis to identify risk factors for ICC insertion.
Methods
We performed a retrospective cohort study of neonates with pneumothorax retrieved by PIPER. Records were accessed through a retrieval database and the electronic medical records at RCH.
Patients
Inclusion
All patients retrieved by PIPER aged ≤28 days between January 2016 and December 2020 with a recorded diagnosis of pneumothorax were included in the study.
Exclusion
Neonates with ICC inserted prior to being referred to PIPER, those with erroneous diagnosis or those diagnosed after transport, neonates with complex congenital anomalies, referrals not transported and neonates with inadequate clinical documentation to determine treatment were excluded from the study.
Outcomes
Primary outcome
The primary outcome was the the proportion and characteristics of neonates with pneumothorax transported without and with ICC.
Secondary outcomes
Incidence of deterioration in neonates transported without and with ICC, and their characteristics.
Proportion of neonates treated with NA.
Proportion of neonates transported without an ICC who had an ICC inserted within 24 hours after transport.
Patient characteristics included gestational age (GA), sex, birth weight (BW), birth mode, 5 min appearance, pulse, grimace, activity and respiration score, and need for PPV at birth. Referral characteristics included distance from Melbourne (where all tertiary NICUs are located), hospital remoteness as defined by the Australian Institute of Health and Welfare,21 referring unit care capability level as defined by the Victorian Department of Health,22 transport duration and transport mode. Clinical characteristics include presence of lung disease, age at diagnosis, diagnostic modality and presence of radiographic mediastinal shift (MS). Clinical parameters including respiratory support (mode and fraction of inspired oxygen (FiO2)), haemodynamic support (volume expansion and inotropes), pneumothorax drainage method, stabilisation time and most recent blood gas analysis were also collected. Stabilisation time was defined as the duration between arrival at the referring unit and departure; travel time was defined as the duration between departure from the referring unit and arrival at the receiving unit. Deterioration was defined a priori by study investigators and listed in box 1.
Definition of deterioration
Definition of deterioration in transport
Respiratory.
Escalation of respiratory support modality.
Commencement of respiratory support where none was previously provided.
Change from low-flow oxygen to either high-flow oxygen, nasal CPAP or MV.
Change from high-flow oxygen to nasal CPAP or MV.
Change from nasal CPAP to MV.
Change from conventional ventilation to high-frequency oscillatory ventilation.
Increase in fraction of inspired oxygen requirement of >20% from time of departure to time of arrival at the receiving hospital.
Need for pneumothorax drainage through any method.
Haemodynamic.
Intravenous fluid bolus.
Commencement of inotropic support.
If already on inotropic support at time of departure, the commencement of secondary agent.
Diversion/return to referring hospital due to clinical instability.
Significant apnoea/bradycardia requiring positive pressure ventilation.
External cardiac massage.
Death.
CPAP, continuous positive airway pressure; MV, mechanical ventilation.
Statistical analysis
Data were analysed using Stata V.16.1. The Shapiro-Wilk test was used to assess for normality. Continuous variables were presented as mean with SD or median with IQR as appropriate. Group differences were assessed using Student’s t-test or Mann-Whitney U test. Categorical variables were presented as frequencies (%) and compared using the χ2 or Fisher’s exact test. Multivariate analysis was performed to determine independent associations between patient and clinical characteristics with ICC insertion. Significant risk factors on univariate analysis were selected to be included in multivariate analysis using an inclusion threshold of p<0.01. Multiple logistic regression with stepwise back elimination was then performed, with p<0.05 considered significant. BW was not included in the multivariate model to mitigate colinearity with GA. Results are presented as ORs with 95% CIs.
Results
Two-hundred and thirty neonates were screened for eligibility based on a recorded diagnosis of pneumothorax. Following exclusions, 174 neonates were included (figure 1).
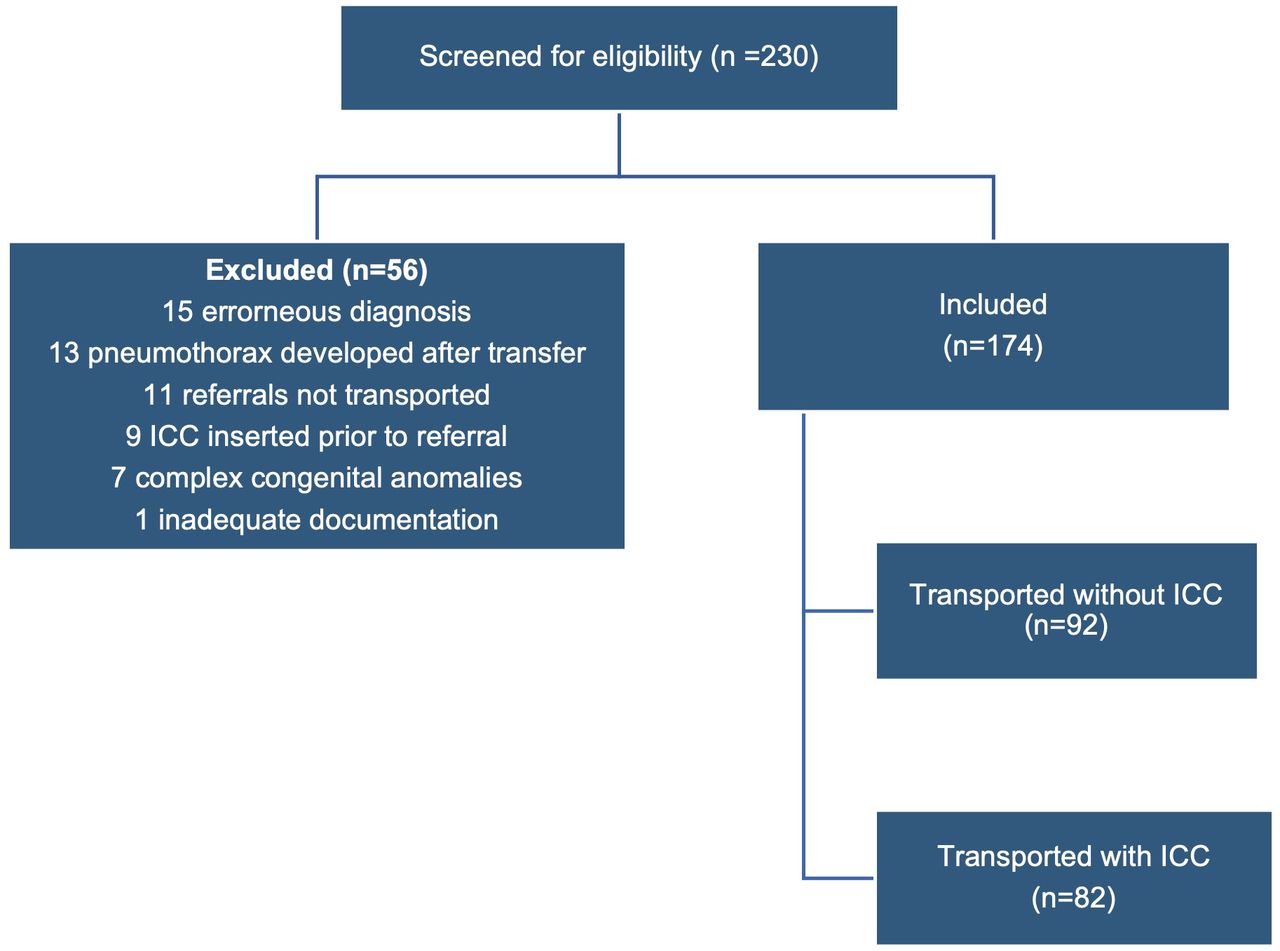
Flowchart of screening, inclusion and exclusion process. ICC, intercostal catheter.
Characteristics of included neonates are listed in table 1. The mean GA was 37.5 (SD 2.8) weeks and the mean BW was 3080 g (SD 723 g). Mean stabilisation time was 2 (SD 1) hours. Transport to the receiving unit was undertaken by road ambulance in 151/174 retrievals (89%), fixed-wing in 18/174 retrievals (10%) and rotary-wing in 5/174 retrievals (3%). The median travel time was 1 (IQR 0.6–1.8) hour. Most referrals originated from major cities (75%).
Characteristics of included neonates
Primary outcome
Eighty-two (47%) neonates had ICC inserted prior to transport by the retrieval team (figure 2). Differences in characteristics of neonates managed without and with ICC are compared in table 2. Those who had ICC inserted had a lower GA (mean 36.4 vs 38.7 weeks, OR 2.4, 95% CI 1.6 to 3.1, p<0.001), a lower BW (mean 2841 vs 3293 g, OR 453, 95% CI 246 to 659, p<0.001) and were older at the time of diagnosis (median age 22 vs 4 hours, p<0.001). Those who had ICC inserted were also more likely to have lung disease (71% vs 40%, OR 3.6, 95% CI 1.9 to 6.7, p<0.001), to be on mechanical ventilation (MV) prior to retrieval team arrival (30/82 vs 8/92, OR 4.9, 95% CI 2.3 to 10.7, p<0.001), receiving higher FiO2 (median of 45% vs 35%, p=0.003) and have MS on chest X-ray (36/73 vs 25/50, OR 4.9, 95% CI 2.3 to 10.7, p<0.001).

{kind=link}
{kind=link}
Pneumothorax drainage method prior to transport. ICC, intercostal catheter.
Comparison of features of neonates managed without and with ICC insertion prior to transport
On univariate analysis, ICC insertion was associated with lower GA, lower BW, later diagnosis, presence of lung disease, need for MV preceding retrieval team arrival, higher FiO2 requirement and presence of MS (table 2). These variables were used in the multivariate analysis, which demonstrated that MV preceding arrival of the retrieval team (OR 12, 95% CI 3.1 to 46.6, p<0.001) and presence of MS (OR 6.2, 95% CI 2.4 to 16.2, p<0.001) remained significant risks. Additionally, increasing GA reduced the likelihood of ICC insertion (OR 0.66, 95% CI 0.5 to 0.8, p<0.001). The predicted probability plot (online supplemental figure) demonstrates the interaction between these risks and likelihood of ICC insertion.
Supplemental material
Neonates who did not have ICC insertion had shorter stabilisation time (1.4 vs 2.6 hours, p<0.001). There were no significant differences seen in referring unit characteristics, duration of transport, blood gas parameters or level of haemodynamic support between neonates who did not have ICC inserted and those who did.
Secondary outcomes
Deterioration in transport
Twelve (7%) neonates deteriorated in transport, with no significant difference between groups (8.5% vs 5.4%, OR 1.6, 95% CI 0.5 to 5.1, p=0.55). Due to small numbers, comparative statistics were not performed (details in online supplemental material). No neonate transported by air without ICC (two by rotary wing, nine by fixed wing) deteriorated.
Interventions for deterioration included escalation in respiratory support (n=1), increase in FiO2 of >20% (n=7), drainage of pneumothorax from pre-existing ICC (n=4), intravenous fluid bolus (n=3), intermittent PPV (n=1) and need for diversion or return to referring hospital for stabilisation (n=2). No neonate required NA or insertion of ICC, commencement or addition of inotropic support or external cardiac massage during transport, and none died.
Needle aspiration
Ninety-five (55%) neonates underwent NA, and 40/95 (42%) subsequently did not require ICC insertion prior to transport.
ICC insertion within 24 hours of transport
Twelve (13%) neonates were transported without an ICC had insertion within 24 hours of arrival at the receiving unit. Two of these had deteriorated in transport. Of the neonates who underwent NA and avoided ICC insertion prior to transport, 33/40 (83%) remained without an ICC for 24 hours after transport.
Discussion
Neonatal pneumothorax is commonly managed by neonatal retrieval teams. Emerging evidence indicates that many pneumothoraces can be managed without ICC insertion in the NICU environment.6 7 9 Evidence pertaining to the management of pneumothorax in the neonatal retrieval setting is scarce. In this study, we described the characteristics of neonates with pneumothorax transported by a neonatal retrieval service, comparing those managed without and with ICC insertion.
To our knowledge, this is the first study in neonatal retrieval comparing the characteristics of neonates with pneumothorax by management strategy and describing risk factors for ICC insertion. We have demonstrated that selected neonates with pneumothorax are safely retrieved without ICC insertion.
In Victoria, Australia, tertiary NICUs, where most neonatal retrievals are brought to, are centralised in Melbourne. Lower acuity units with varying neonatal-care capability levels are spread across a geographical area of 227 000 km2. Despite this geographical spread, most (75%) neonates in our study cohort were retrieved from major cities with a relatively short travel time (median of 1 hour). Many of the referring units located within this area care for neonates from 32 weeks’ gestation who are moderately unwell but do not provide MV or ICC insertion. Care of these patients, who are at risk of developing pneumothorax, combined with limited resources for escalation of care, likely explains this referral bias.
Forty-seven per cent of neonates with pneumothorax had an ICC inserted prior to transport, lower than previously described.14 This difference may be attributable to the smaller proportion of neonates undergoing MV and those with MS in our cohort, but may also reflect more contemporary practice favouring less invasive treatment.
Murphy et al found that 45% of neonates in NICUs with pneumothorax treated with NA did not require ICC insertion within 6 hours.9 We found that the proportion of neonates who avoided ICC insertion prior to transport after NA was slightly lower (42%). This finding demonstrates a clinically significant proportion of neonates who were managed with NA alone prior to transport. With shorter stabilisation times, low incidence of deterioration and low likelihood of needing ICC in the first 24 hours of arrival at the receiving unit, the use of NA in selected neonates to manage pneumothorax in retrieval warrants further exploration.
Interestingly, many neonates without ICC were supported with continuous positive airway pressure (CPAP) (52%). Despite evidence that CPAP is associated with an increased risk of pneumothorax,3 our data indicate that in neonates with pneumothorax, CPAP requirement alone is not associated with the need for ICC. This finding is reassuring as CPAP is frequently used in neonatal retrieval.23
The incidence of deterioration in neonates transported with pneumothorax was low. Although the small numbers limited detailed analysis, it is reassuring that numbers are proportionate in both groups. Furthermore, no neonate required emergent NA or ICC insertion in transport. Notably, 11 neonates were transported by air without ICC, and none deteriorated. While this finding is not statistically significant, it suggests a need to further study the effects of altitude on neonates with pneumothorax.
In our cohort, neonates who did not have an ICC inserted prior to transport were unlikely to subsequently have ICC insertion within 24 hours of transport. This suggests that not inserting ICC prior to transport did not delay effective treatment, and the likelihood of being transported with an inadequately decompressed pneumothorax was low.
Our multivariate model demonstrated independent associations between ICC insertion and lower GA, need for MV preceding retrieval team arrival and presence of MS. These factors are evident prior to retrieval team dispatch and may predict ICC insertion, thus assisting in planning team composition, stabilisation tasks and anticipated stabilisation time. Future studies should aim to develop and validate a risk predictive score using these criteria, which could guide clinical decision making.
Our study has limitations. First, the retrospective design is susceptible to documentation and abstraction errors. To mitigate this, clear criteria were developed, and data abstraction was limited to two investigators. Second, neonates were included based on documented diagnosis of pneumothorax. As minor pneumothoraces can be challenging to diagnose, it is possible that a proportion of cases did not have clinically significant pneumothorax, leading to a conservative treatment strategy bias. As diagnostic images used by retrieval clinicians were not readily available, this could not be used to define the study population.
Lastly, as a retrospective study, it is not possible to infer causation between observed characteristics and outcomes. Some management decisions, such as using MV to facilitate analgesia and sedation in neonates requiring ICC, may affect our findings and cannot be controlled for through this study. Instead, a pragmatic, clinical approach was used by excluding neonates who already had ICC inserted prior to referral and examining MV needs preceding ICC insertion rather than following. Despite these limitations, our study has provided preliminary data and identified associations that can be further validated through a prospective study.
Conclusion
In retrieval, many neonates with pneumothorax are transported without ICC insertion. This is associated with shorter stabilisation times, low incidence of in-transport deterioration and a low likelihood of requiring ICC within 24 hours after retrieval. ICC insertion is avoided in over a third of neonates managed with NA. The likelihood of ICC insertion is increased by lower GA, MV prior to retrieval team arrival and radiographical MS. Clinical validation of these associations can be used to improve outcomes for neonates with pneumothorax requiring retrieval while improving the efficiency of retrieval services and warrants further exploration through prospective studies.
Data availability statement
All data relevant to the study are included in the article or uploaded as supplementary information.
Ethics statements
Patient consent for publication
Ethics approval
This study involves human participants and was approved by Royal Children’s Hospital (RCH) Ethics Committee (HREC/79078/RCHM-2021). The study involved anonymised data collection from retrospective chart review only, for the purposes of evaluation and improvement of health services. This can be done without consent as per Health Privacy Principles and approved by the RCH Ethics Committee.
Acknowledgments
We thank Dr Rosemarie A Boland (Royal Children’s Hospital, Royal Women’s Hospital, Murdoch Children’s Research Institute and University of Melbourne) for her contribution to study design, ethics application process and abstract review.
References
Supplementary materials
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Footnotes
Contributors IH, KH, ND, MS and AS conceived and designed the study. IH and FH conducted data collection, analysis and interpretation. IH drafted the manuscript and was responsible for the overall content as guarantor. AS and KH supervised the project. All authors critically reviewed the manuscript, provided the final approval for the final version to be published and agreed to be accountable for all aspects of the work.
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Competing interests None declared.
Provenance and peer review Not commissioned; externally peer reviewed.
Supplemental material This content has been supplied by the author(s). It has not been vetted by BMJ Publishing Group Limited (BMJ) and may not have been peer-reviewed. Any opinions or recommendations discussed are solely those of the author(s) and are not endorsed by BMJ. BMJ disclaims all liability and responsibility arising from any reliance placed on the content. Where the content includes any translated material, BMJ does not warrant the accuracy and reliability of the translations (including but not limited to local regulations, clinical guidelines, terminology, drug names and drug dosages), and is not responsible for any error and/or omissions arising from translation and adaptation or otherwise.
Linked Articles
- Highlights from this issue