Article Text

Abstract
Objective Remote ischaemic conditioning (RIC) improves the outcome of experimental necrotising enterocolitis (NEC) by preserving intestinal microcirculation. The feasibility and safety of RIC in preterm infants with NEC are unknown. The study aimed to assess the feasibility and safety of RIC in preterm infants with suspected or confirmed NEC.
Design Phase I non-randomised pilot study conducted in three steps: step A to determine the safe duration of limb ischaemia (up to 4 min); step B to assess the safety of 4 repeated cycles of ischaemia-reperfusion at the maximum tolerated duration of ischaemia determined in step A; step C to assess the safety of applying 4 cycles of ischaemia-reperfusion on two consecutive days.
Setting Level III neonatal intensive care unit, The Hospital for Sick Children (Toronto, Canada).
Patients Fifteen preterm infants born between 22 and 33 weeks gestational age.
Intervention Four cycles of ischaemia (varying duration) applied to the limb via a manual sphygmomanometer, followed by reperfusion (4 min) and rest (5 min), repeated on two consecutive days.
Outcomes The primary outcomes were (1) feasibility defined as RIC being performed as planned in the protocol, and (2) safety defined as perfusion returning to baseline within 4 min after cuff deflation.
Results Four cycles/day of limb ischaemia (4 min) followed by reperfusion (4 min) and a 5 min gap, repeated on two consecutive days was feasible and safe in all neonates with suspected or confirmed NEC.
Conclusions This study is pivotal for designing a future randomised controlled trial to assess the efficacy of RIC in preterm infants with NEC.
Trial registration number NCT03860701.
- neonatology
- gastroenterology
Data availability statement
Data are available on reasonable request. Individual deidentified participant data will not be made available.
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
What is already known on this topic
It has been demonstrated in preclinical models of NEC that remote ischaemic conditioning (RIC) effectively counteracts the intestinal damage due to NEC and prolongs survival by improving intestinal microcirculation.
RIC has never been investigated in preterm human neonates, the population that is at the highest risk for developing NEC.
What this study adds
This study demonstrates that it is safe, in preterm neonates with bodyweight between 840 and 2490 g, to apply four cycles of RIC each consisting of limb ischaemia (4 min) followed by reperfusion (4 min) and a 5 min gap, repeated on two consecutive days without any local or systemic adverse effects.
How this study might affect research, practice or policy
This research is pivotal for the design of a randomised controlled trial aimed to assess the efficacy of RIC in preterm infants with NEC.
Introduction
Necrotising enterocolitis (NEC) is one of the most common and severe gastrointestinal complications of prematurity. NEC affects 5%–10% of extremely preterm infants and is associated with high mortality (30%–50%).1 Survivors have increased comorbidity (ie, bronchopulmonary dysplasia, postnatal growth restriction) and neurodevelopment impairment rates compared with preterm infants without NEC.2 3
Current management is based on broad-spectrum antibiotics, bowel decompression and rest, analgesia, blood product transfusions and cardiovascular and respiratory support as required.1 In case of bowel perforation or clinical deterioration despite the implementation of adequate medical treatment, surgery is indicated.4 This has been the standard of care over the last three decades as there have not been significant changes in the management of NEC. However, NEC morbidity and mortality still remain high.5–7 Therefore, new preventive strategies and therapeutic options are urgently needed.
Remote ischaemic conditioning (RIC) is a manoeuvre that involves application of brief cycles of non-lethal ischaemia and reperfusion to a remote organ/site that conveys protection to distant organs withstanding ischaemic injury. We recently demonstrated that RIC promotes recovery from experimental NEC by reducing intestinal injury, inflammation and enhancing survival.8 The mechanism of action of RIC in NEC is dependent on improving intestinal microvascular blood flow by the vasodilatory action of hydrogen sulfide and nitric oxide.8
RIC has been applied to adults,9–11 children12–15 and neonatal patients >36 weeks of gestational age16 for different diagnoses. However, it has not been attempted in preterm neonates including those who had NEC, mostly due to concerns regarding feasibility and safety in this vulnerable population. Thus, our objective was to assess the feasibility and safety of RIC in preterm infants with suspected or confirmed NEC. We hypothesised that RIC (up to four cycles of 4 min of ischaemia repeated after 24 hours) would be feasible and safe in this vulnerable population.
Methods
Design and setting
We conducted a phase I feasibility and safety trial in the neonatal intensive care unit of the Hospital for Sick Children, Toronto (trial flow chart according to Consolidated Standards of Reporting Trials guidelines in online supplemental material). The trial was registered at ClinicalTrials.gov (NCT03860701).
Supplemental material
Participants
Patients with suspected or confirmed NEC (stages I–III as per the modified Bell’s classification)17 were eligible for this study if they weighed ≥750 g at the time of recruitment and were <36 weeks of gestational age at birth. Exclusion criteria were: (1) major congenital heart disease, (2) congenital diaphragmatic hernia, (3) gastroschisis, (4) antecedent of limb ischaemia/limb thrombotic events, (5) antecedent diagnosis of occlusive arterial or venous thrombosis and (6) haemodynamic instability (defined as two inotropes/vasopressors administration, or one inotrope/vasopressor and hydrocortisone administration or one inotrope/vasopressor with dose increased in previous 6 hours).
Intervention
Limb ischaemia-reperfusion cycles were applied by placing an appropriately sized blood pressure cuff around a limb, and inflating (until blood flow distal to the cuff was interrupted with no pulse detected by pulse oximetry) and deflating it using a manual sphygmomanometer (Tycos, Welch Allyn, Skaneateles Falls, New York, USA). Before and after each ischaemia-reperfusion cycle, cutaneous integrity and perfusion (colour, capillary refill time) were assessed. The presence of grasp reflex was ascertained immediately before, right after and again 24 hours after RIC. Urine output (mL/kg/hour) during the 24 hours before and 24 hours after RIC was also recorded. Pain was evaluated 30 s after each ischaemic phase and 6 hours after the last RIC cycle using the Premature Infant Pain Profile (PIPP score).18 19 According to the protocol, RIC was due to be stopped if there was no return of limb perfusion on clinical assessment and/or no return of oxygen saturation to baseline values±3% within 4 min in the hand or foot of the limb receiving RIC. If perfusion did not return, the limb was warmed and elevated for 10 min, followed by nitroglycerine patch application and Doppler ultrasound if necessary.
To determine tolerability of the ischaemia period up to a maximum of 4 min, as well as feasibility of applying repeated cycles of ischaemia-reperfusion on two consecutive days, the study was conducted in three steps.
Step A
Four cycles of limb ischaemia-reperfusion in 1 day, increasing the ischaemia time by 1 min in each cycle starting at 1 min in the first cycle to a maximum of 4 min in the last cycle. Each ischaemic cycle was followed by reperfusion (4 min) and rest (5 min) before the next cycle.
Step B
Four cycles of ischaemia-reperfusion in 1 day, consisting of the longest safe duration of ischaemia determined in step A, followed by reperfusion (4 min) and rest (5 min).
Step C
Four cycles of ischaemia-reperfusion as in step B but repeated on two consecutive days (24±2 hours apart).
Study outcomes
The primary outcomes were the feasibility and safety of RIC. Feasibility was defined as the ability to apply the RIC manoeuvre as planned in the protocol (available on request). Safety was defined as the return of limb perfusion to baseline within 4 min after cuff deflation assessed by clinical assessment of skin colour, pulse oximetry and capillary refill time.
Secondary outcomes included:
Peripheral nerve injury indicated by loss of grasp reflex after RIC.
Cutaneous injury identified as a new-onset skin breakdown, bruising, ecchymosis or petechiae within 24 hours after RIC.
Pain assessed by measuring the PIPP score before RIC, 30 s after each RIC cycle and 6 hours after the last cycle. This validated score ranges from 0 to 21 with 0–6 indicating no pain, 6–12 mild-to-moderate pain and >12 severe pain.19
Change in urine output (mL/kg/hour) measured over 24 hours before and after RIC.
The primary and secondary outcomes after each study step (A, B or C) were reviewed anonymously by an independent safety panel of experts including two neonatologists, one paediatric surgeon, one cardiologist and one nurse practitioner, not involved in the circle of care, trial design and execution. This panel determined whether it was appropriate (i) to proceed to the next study step, (ii) recruit more patients in the same step and (iii) stop the trial altogether.
Statistical methods
Data are presented as median (range) and n (%) as indicated. A two-way analysis of variance with main effects only and post hoc Tukey’s multiple comparisons test was used to compare pre-RIC and post-RIC oxygen saturation, capillary refill time (s) and PIPP score. A paired non-parametric Wilcoxon test was used to compare pre-RIC and post-RIC urine output (mL/kg/hour). P value <0.05 was considered statistically significant. GraphPad Prism 8 (GraphPad Software, San Diego, California, USA) was used for data analysis and presentation.
Results
Fifteen neonates were recruited, five in each step of the study (tables 1 and 2). All neonates were preterm with a birth weight ranging from 490 to 2010 g. NEC was diagnosed between 7 and 58 days and RIC was performed after a median of 4 days (2–33) from NEC diagnosis. Table 1 reports patients’ demographics and NEC Bell’s stage at the time of RIC. Thirteen (87%) patients were mechanically ventilated at the time of RIC. Five (33%) received medical treatment and 10 (67%) required an operation for NEC.
Characteristics of the study population
Safety outcomes of the RIC manoeuvre
The independent panel of experts confirmed the feasibility and safety after each study step, did not require recruitment of further patients and did not stop the trial at any step.
Primary outcomes
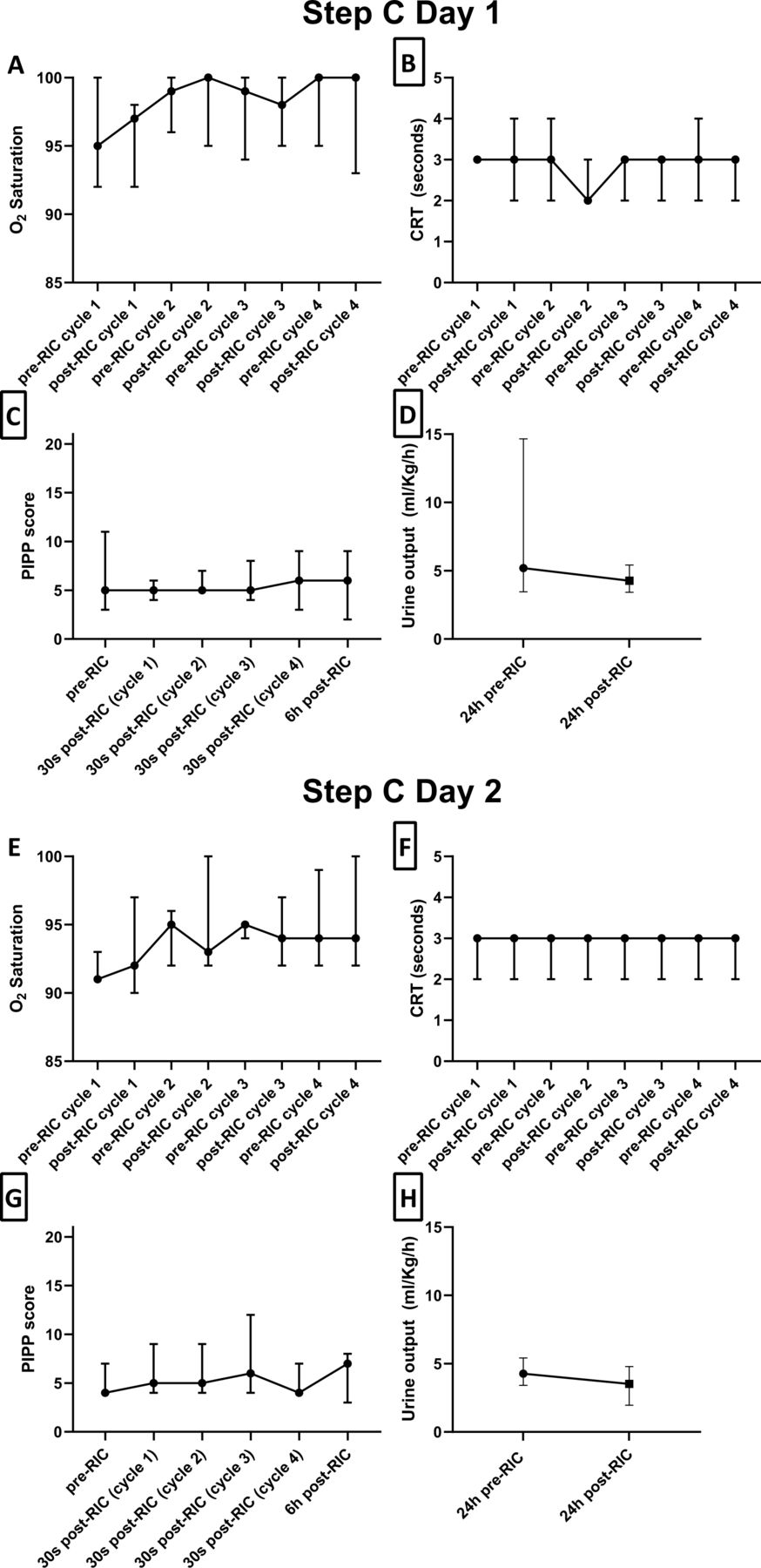
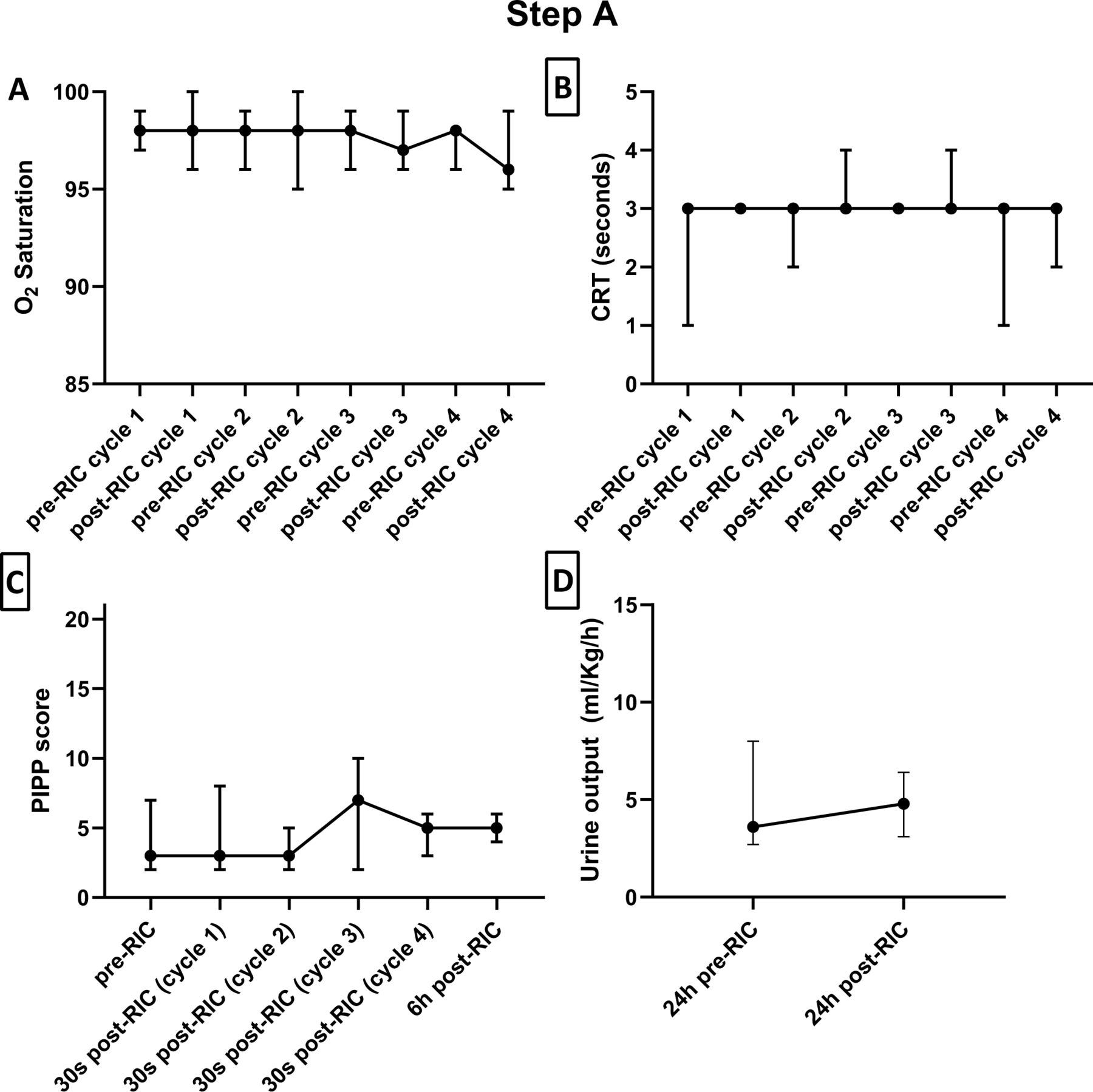
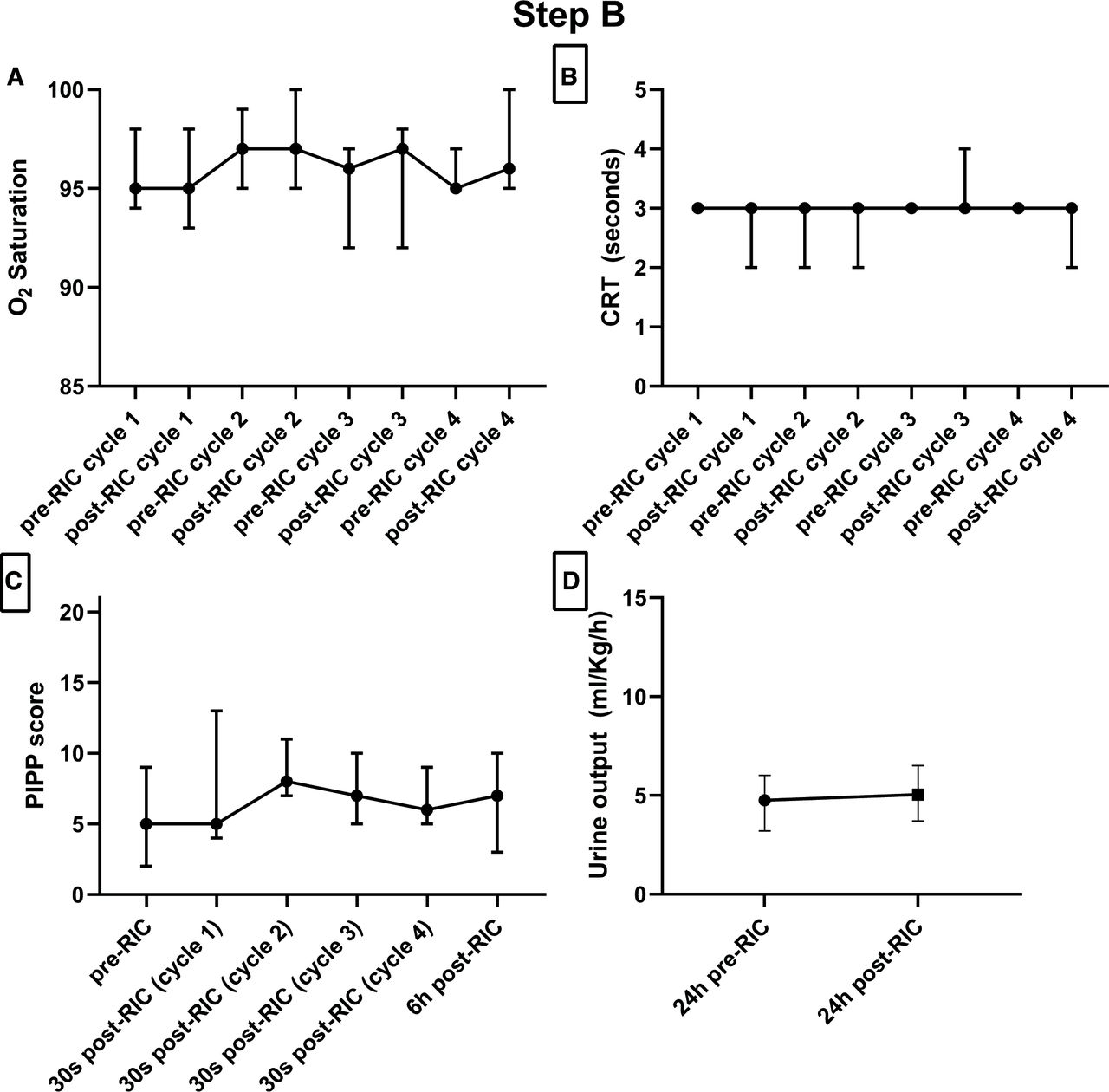
RIC was completed according to the protocol in all neonates (14 in the arm and 1 in the leg). Arterial flow and limb perfusion returned to baseline within 4 min in all patients, as confirmed by clinical assessment of limb, return of pulse waveform displayed by pulse-oximetry, return to peripheral oxygen saturation to pre-RIC value (figures 1A–3A and figure 3E) and capillary refill time preservation (figures 1B–3B and 3F). Two enrolled patients died before discharge; however, none of the deaths were attributed to the RIC procedure. One patient died due to septic shock 4 days after RIC and the other died due to multiorgan failure 2 months after RIC.

Physiological variables recorded to assess the safety of remote ischaemic conditioning (RIC) in step A (n=5). (A) Peripheral oxygen (O2) saturation and (B) capillary refill time (CRT in s) were assessed before and after every cycle of ischaemia. (C) Pain was assessed according to the Premature Infant Pain Profile (PIPP score) and measured before the first RIC cycle, 30 s after each cycle and 6 hours after the last cycle of ischaemia. (D) Urine output (mL/kg/hour) was measured 24 hours before and after RIC. Data are represented as median with range. A two-way analysis of variance with main effects only and post hoc Tukey’s multiple comparisons test was used to compare pre-RIC and post-RIC oxygen saturation, CRT (s) and PIPP score. A paired non-parametric Wilcoxon test was used to compare pre-RIC and post-RIC urine output (mL/kg/hour). There was no significant difference between pre-RIC and post-RIC values of any of the listed parameters.

Physiological variables recorded to assess the safety of remote ischaemic conditioning (RIC) in step B (n=5). (A) Peripheral oxygen (O2) saturation and (B) capillary refill time (CRT in s) were assessed before and after every cycle of ischaemia. (C) Pain was assessed according to the Premature Infant Pain Profile (PIPP score) and measured before the first RIC cycle, 30 s after each cycle and 6 hours after the last cycle of ischaemia. (D) Urine output (mL/kg/hour) was measured 24 hours before and after RIC. Data are represented as median with range. A two-way analysis of variance with main effects only and post hoc Tukey’s multiple comparisons test was used to compare pre-RIC and post-RIC oxygen saturation, CRT (s) and PIPP score. A paired non-parametric Wilcoxon test was used to compare pre-RIC and post-RIC urine output (mL/kg/hour). There was no significant difference between pre-RIC and post-RIC values of any of the listed parameters.
{kind=link}
{kind=link}
{kind=link}
Physiological variables recorded to assess the safety of remote ischaemic conditioning (RIC) in step C day 1 and 2 (n=5 in each day). (A, E) Peripheral oxygen (O2) saturation and (B, F) capillary refill time (CRT in s) were assessed before and after every cycle of ischaemia. The day 2 CRT for all patients is reported, although lines are superimposed. (C, G) Pain was assessed according to the Premature Infant Pain Profile (PIPP score) and measured before the first RIC cycle, 30 s after each cycle and 6 hours after the last cycle of ischaemia. (D, H) Urine output (mL/kg/hour) was measured 24 hours before and after RIC. Data are represented as median with range. A two-way analysis of variance with main effects only and post hoc Tukey’s multiple comparisons test was used to compare pre-RIC and post-RIC oxygen saturation, CRT (s) and PIPP score. A paired non-parametric Wilcoxon test was used to compare pre-RIC and post-RIC urine output (mL/kg/hour). There was no significant difference between pre-RIC and post-RIC values of any of the listed parameters.
Secondary outcomes
All patients had a normal grasp reflex both before and after RIC. No new-onset skin lesions (breakdown, bruising or ecchymosis) were observed. PIPP scores obtained before and after RIC are reported in figures 1C–3C and 3G. There was no significant difference in PIPP score comparing its value before and 6 hours after RIC (table 2). Compared with the assessment before RIC, the PIPP score did not change from ‘no pain’ or ‘mild-to-moderate’ to ‘severe’ pain 6 hours after the last ischaemic cycle. The PIPP score in five neonates (33%) increased from ‘no pain’ to ‘mild-to-moderate’ pain, and in two neonates (13%) decreased from ‘mild-to-moderate’ pain to ‘no pain’. No patient became oligo-anuric (defined as urine output <1 mL/kg/hour) after RIC (figures 1D–3D and 3H, table 2).
Discussion
In this phase I feasibility and safety trial, we demonstrated that RIC consisting of four consecutive cycles of 4 min ischaemia followed by 4 min reperfusion on two consecutive days is feasible in preterm infants with NEC. No significant adverse events related to RIC were detected. Reperfusion occurred promptly after RIC in all patients without any impairment in vascular flow and no cutaneous, nor nerve injury was observed.
To our knowledge, RIC has not been evaluated in preterm infants with NEC. Eighty-seven per cent of enrolled neonates in this phase I trial were born before 28 weeks gestation and 73% were extremely low birth weight (<1000 g), representing the population at higher risk of NEC. In this study, we assessed the feasibility and safety of RIC in fragile preterm neonates with either suspected or defined medical and surgical NEC, suggesting that RIC is safe and can be applied even during acute illness.
Prematurity and enteral formula feeding are two of the most important risk factors for NEC.1 8 20 21 Additionally, ischaemia plays a role in both NEC pathogenesis and pathophysiology.20–22 Physiologically, intestinal blood flow is known to increase above baseline to fulfil the increased intestinal oxygen demand after feeds.20 However, postprandial hyperaemia is remarkably compromised in premature infants that later developed NEC,23 and we have demonstrated that NEC in human preterm infants is associated with impairments in intestinal microcirculation.8 20 Furthermore, NEC risk is higher in infants with intrauterine growth restriction and circulatory impairment, respiratory distress syndrome and associated hypoxia requiring surfactant treatment or early onset sepsis.24 In addition, persistent ductus arteriosus can lead to bowel hypoperfusion25 and is also associated with NEC.26 Previous studies on splanchnic circulation using near-infrared spectroscopy showed that regional oxygen saturation is lower, especially after feeds in babies who later developed NEC.22 27 Lastly, at the disease onset, local bowel inflammation is associated with impaired microcirculation which leads to bowel wall ischaemia and eventually transmural necrosis.28 In fact, patched coagulative necrosis (a marker of ischaemia) is the main pathological finding in NEC patients, and hypoxia markers like hypoxia-inducible factor 1α and glucose transporter 1 are elevated in NEC intestinal resection specimens.29
Considering the role of ischaemia in NEC, modulating the immature intestinal microvasculature could prove to be a viable strategy to counteract the feeding-induced hypoxia and prevent the progression of NEC. For this reason, we evaluated RIC, a manoeuvre which can improve the blood supply to the intestine. RIC involves application of brief cycles of ischaemia and reperfusion to a limb to protect distant organs from sustained ischaemic damage—in this case the intestine. Prior to the current trial, experimental studies performed by our group demonstrated that RIC induced endothelium-dependent vasodilation, preserved bowel microcirculation and reduced gut injury and mortality due to NEC.8
RIC implies inflating a standard blood pressure cuff around a limb, aiming to interrupt distal arterial blood supply to produce transient skeletal muscle ischaemia. To assess safety of this procedure in the study population, potential complications/side effects were monitored including limb ischaemia, peripheral nerve damage, pain and change in urinary output.
First, limb ischaemia is a potential complication of peripheral or central arterial lines in neonates. Vascular obstruction is known to present as a pale and poorly perfused limb distal to the occluded point. We assumed RIC could have induced persistent limb ischaemia after cuff deflation secondary to arterial thrombosis or vasospasm. To prove this was not the case, limb perfusion was continuously monitored during the procedure and cautiously assessed after RIC, both visually and with pulse oximetry. During RIC, the limb became dusky (venous congestion), and the pulse wave was lost due to total arterial compression as expected and desired. Once the blood pressure cuff was deflated, we observed rapid reperfusion, usually with evident hyperaemia in visual inspection. Capillary refill time was assessed before and after every ischaemia cycle to quantify limb perfusion and always recovered within 4 min.
Second, to assess peripheral nerve integrity, palmar or plantar grasp reflex (depending on the limb used) was assessed before and after RIC as it is a useful clinical marker of potential nerve ischaemic injury involving both sensorial and motor fibres.29 The grasp reflex was preserved in all patients.
Third, RIC requires limb compression with pressure above systolic pressure affecting venous blood return and potentially leading to microhaemorrhage (petechiae, ecchymosis, bruising) and/or skin breakdown in this vulnerable patient population. However, none of the neonates developed cutaneous bleeding or changes in skin integrity after RIC.
Forth, pain has also been related to worsening neurodevelopment in preterm infants.30 NEC is a cause of pain, making it challenging to separate pain due to NEC from that due to RIC. To add objectivity to our prospective evaluation, pain was assessed before and after RIC using the validated PIPP score.19 There was no development of persistent or severe pain after RIC, and in none of the neonates, the RIC manoeuvre was discontinued due to pain.
At last, in theory, muscle ischaemia could have led to muscle necrosis and rhabdomyolysis.31 The most severe potential complication of rhabdomyolysis is oliguric acute kidney injury secondary to renal tubules obstruction with myoglobin affecting >50% of them. We did not find any difference in urine output 24 hours before and after RIC and none of the neonates studied became oligo-anuric after RIC. Moreover, without significant renal impairment, rhabdomyolysis is a self-resolving transient condition.
Two of our patients died, none of them of causes directly related to RIC but due to the underlying disease. Indeed, the study’s mortality was not higher than the mortality of NEC in preterm infants. Although there is no evidence of harm in this phase I preliminary trial, there may be beneficial or detrimental effects that can only become apparent in larger phase II–III trials. We acknowledge that the small sample size of the present study, although typical of phase I trials, did not allow us to rule out other potential complications. Specifically, the possibility that reactive oxygen metabolites can cause reperfusion injury in other organs and may worsen chronic lung disease, retinopathy of prematurity or other complications of prematurity, as well as potential effects of RIC on long-term neurological development will have to be assessed in future phase II and III trials.
RIC is simply performed by inflating and deflating a blood pressure cuff, similar to blood pressure measurement, and can be performed with minimal invasiveness and cost in preterm neonates with NEC, making it potentially applicable worldwide.
Conclusions
In this study, we demonstrated that RIC is feasible and safe in small and fragile preterm neonates with NEC. These novel findings are essential to embark on a multicentre randomised controlled trial to investigate the efficacy of RIC in reducing NEC progression, morbidity and mortality.
Data availability statement
Data are available on reasonable request. Individual deidentified participant data will not be made available.
Ethics statements
Patient consent for publication
Ethics approval
This study was approved by Institutional Research Ethics Board (REB) at the Hospital for Sick Children (REB: 1000061144). Participants gave informed consent to participate in the study before taking part.
Acknowledgments
We are very grateful to the members of the independent safety panel of experts who reviewed the results after every step of this study: Luc Mertens MD, PhD (Division of Cardiology, The Hospital for Sick Children, Toronto, Ontario, Canada); Yenge Diambomba MD, FRCP (Department of Pediatrics, Neonatal Intensive Care Unit, Mount Sinai Hospital, Toronto, Ontario, Canada), Eugene Ng, MD, FRCPC, FAAP (Department of Newborn and Developmental Paediatrics, Sunnybrook Health Sciences Centre, Toronto, Ontario, Canada), David Wesson MD (Pediatric Surgery Division, Texas Children’s Hospital, Houston, Texas, USA) and Irina Pashynskyy MScN, NP-PHC (Division of General and Thoracic Surgery, Toronto, Ontario, Canada).
References
Supplementary materials
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Footnotes
Correction notice This article has been updated since it was published online. An Orcid ID has been been added to one of the authors.
Contributors All authors approved the final manuscript as submitted and agree to be for all accountable aspects of the work. CZ was involved in the study design, performing the clinical procedures, acquisition of data, interpretation of data and writing of the paper. NG, MJL, BL, CL, YK, MO and EG were involved in interpreting the data and writing of the paper. SE and PSS were involved in the study’s design, interpretation of data and paper writing. AP was involved in the conceptualisation of study hypothesis, design of the study, interpretation of data, writing of the paper and study supervision, and is responsible for the overall content as the guarantor.
Funding SE acknowledges support from the NIHR Biomedical Research Centre at Great Ormond Street, London, UK. NG was the recipient of Restracomp Scholarship from the Hospital for Sick Children, Toronto, Ontario, Canada. AP was supported by the Canadian Institutes of Health Research (CIHR) Foundation Grant 353857. The other authors received no additional funding. The listed funding sources had no role in the design and conduct of the study.
Competing interests None declared.
Provenance and peer review Not commissioned; externally peer reviewed.
Supplemental material This content has been supplied by the author(s). It has not been vetted by BMJ Publishing Group Limited (BMJ) and may not have been peer-reviewed. Any opinions or recommendations discussed are solely those of the author(s) and are not endorsed by BMJ. BMJ disclaims all liability and responsibility arising from any reliance placed on the content. Where the content includes any translated material, BMJ does not warrant the accuracy and reliability of the translations (including but not limited to local regulations, clinical guidelines, terminology, drug names and drug dosages), and is not responsible for any error and/or omissions arising from translation and adaptation or otherwise.