Article Text

Abstract
Objective To determine whether weaning from nasal continuous positive airway pressure (nCPAP) using heated humidified high flow nasal cannula (nHF) was non-inferior to weaning using nCPAP alone in relation to time on respiratory support.
Study design Single-centre, non-inferiority, randomised controlled trial.
Setting Neonatal Intensive Care Unit, Middlemore Hospital, Auckland, New Zealand.
Patients 120 preterm infants, <30 weeks’ gestation at birth, stable on nCPAP for at least 48 hours.
Interventions Infants underwent stratified randomisation to nHF 6 L/min or bubble CPAP 6 cm water. In both groups, stepwise weaning of their respiratory support over 96 hours according to a strict weaning protocol was carried out.
Main outcome measures Time on respiratory support from randomisation to 72 hours off respiratory support or 36 weeks’ postmenstrual age. The non-inferiority threshold was set at 15%.
Results 59 infants were randomised to weaning using nHF and 61 using nCPAP. The groups were well balanced in regards to baseline demographics. The restricted mean duration of respiratory support following randomisation for the nCPAP group, using per-protocol analysis was 401 hours (upper boundary, mean plus 0.15, was 461 hours) and 375 hours in the nHF group (upper 95% CI 413 hours). nHF weaning was, therefore, non-inferior to nCPAP weaning at the non-inferiority threshold. There was no significant difference in time to discharge.
Conclusion For infants ready to wean from nCPAP, the CHiPS study found that nHF was non-inferior to discontinuing nCPAP at 5 cm water.
Trial registration number Australia and New Zealand Clinical Trials Registry (ACTRN12615000077561).
- respiratory
- neonatology
Data availability statement
All data relevant to the study are included in the article or uploaded as supplementary information. Study data is not available
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
WHAT IS ALREADY KNOWN ON THIS TOPIC
Continuous positive airway pressure is the mainstay of non-invasive respiratory support in neonatal intensive care units. It does come with some complications including air leak and nasal septal damage.
Early weaning from nasal continuous positive airway pressure (nCPAP) is important, the best way to wean remains unclear.
There have only been a small number of randomised controlled trials which have explored weaning preterm infants from nCPAP using high flow nasal cannula (nHF).
WHAT THIS STUDY ADDS
Weaning from nCPAP using nHF was non-inferior to weaning from nCPAP alone in stable very preterm infants, when using strict weaning and failure criteria.
HOW THIS STUDY MIGHT AFFECT RESEARCH, PRACTICE OR POLICY
Further investigation is required into weaning extreme preterm infants born at <27 weeks’ gestation off nCPAP with the use of nHF.
The study provides evidence on the use of nHF in weaning stable preterm infants from nCPAP and may help inform decision-making.
Introduction
Nasal continuous positive airway pressure (nCPAP) has become the mainstay of non-invasive respiratory support for preterm infants.1 Reported benefits compared with mechanical ventilation include lower rates of combined death or chronic lung disease (CLD) at 36 weeks’ postmenstrual age (PMA).2 Potential complications of nCPAP include air leak,3 nasal septal damage4 5 and gaseous bowel distension.6 7 A recent study reported that despite an increase in the use of nCPAP over time, the duration of oxygen therapy and oxygen dependence at 36 weeks’ PMA have risen, compared with earlier periods.8
Early weaning from nCPAP is, therefore, important; however, there is a lack of consensus over how best to achieve this. Options include immediate removal of nCPAP at a predetermined pressure, removing nCPAP for a number of hours each day with increasing time off and stopping nCPAP and starting high flow nasal cannula (nHF) or cycling infants between different modalities of non-invasive support.9 10 Four randomised controlled trials (RCTs) have been published,11–14 with the majority of these reporting that weaning from nCPAP using nHF was as effective as weaning from nCPAP alone. As well as being preferred by parents15 16 and nurses,17 potential benefits of nHF include easier application,18 less nasal trauma17 19–21 and lower rates of pneumothorax.22 Our primary outcome was time on respiratory support.
Methods
The CHiPS study was a single-centre RCT at Middlemore Hospital, New Zealand, from 2015 to 2019 (ACTRN12615000077561). Preterm infants <30 weeks’ gestational age (GA) who were on Hudson (Teleflex Medical, New Zealand) bubble nCPAP 6 cm water pressure for at least 48 hours and deemed ready to wean were eligible, provided informed consent was obtained. To be deemed ready to wean infants had to meet stability criteria for the 24 hours prior to randomisation. This period could be part of the 48 hours at 6 cm nCPAP as noted above. The stability criteria were as follows:
No requirement for oxygen supplementation.
Respiratory rate ≤60 breaths/min.
No significant desaturation (SpO2 <80%) or bradycardia (heart rate <100 beats/min) requiring bedside intervention.
Infants who had previously been off respiratory support for >7 days or had significant congenital heart disease, surgical conditions, chromosomal abnormalities, genetic syndromes or other major congenital malformations were excluded.
Prior to randomisation infants received routine clinical management, primarily bubble nCPAP using Hudson binasal prongs with humidification (Fisher and Paykel 950 humidifier, New Zealand). Prior to the study nHF using Optiflow Junior nasal prongs with humidification (Fisher and Paykel, New Zealand) was only used for infants ≥36 weeks’ PMA. Airway suctioning occurred 4–6 hourly as required. All infants in the study received caffeine citrate.
The randomisation sequence was computer generated and stratified (≥27 weeks’ or <27 weeks’ GA) with random block sizes (2-10) and allocation using sequentially numbered sealed opaque envelopes, which clinicians opened immediately prior to study entry. Infants were randomised to wean off nCPAP support either by changing to nHF and progressively weaning the flow compared with weaning of nCPAP pressure, with strict adherence to the weaning protocol (figure 1). For all infants, the study commenced at 12 midday on the day of randomisation.
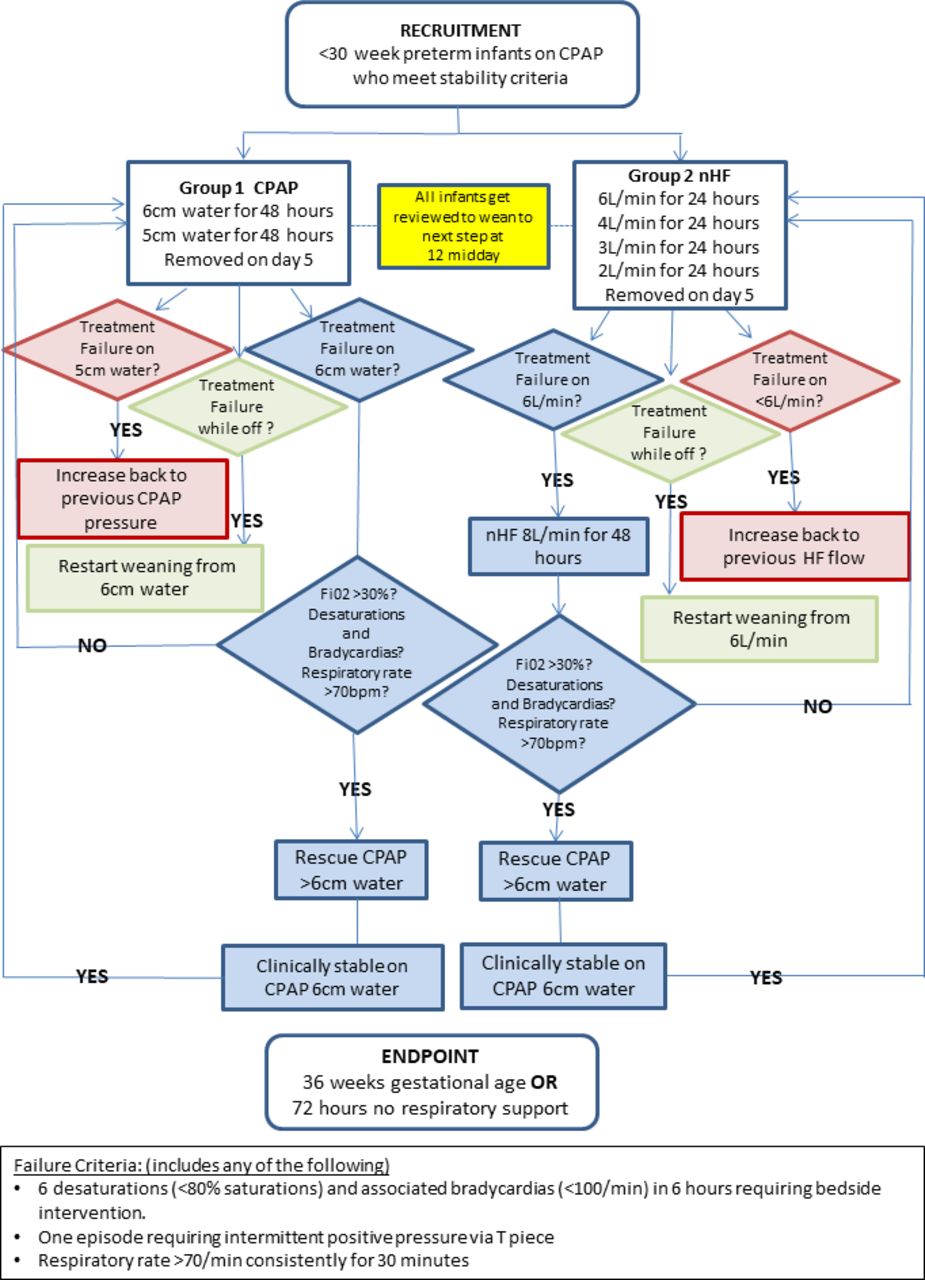
Weaning protocol. nCPAP, nasal continuous positive airway pressure; nHF, high flow nasal cannula.
Ninety-six hours was the minimal time before trialling off. At each step stability criteria had to be met. Prior to randomisation all infants had been on nCPAP. Infants did not wean to the next step if failure criteria were met, following review of the nursing observation chart and cardiorespiratory monitor (Philips IntelliVue MX800; Philips Medizin Systeme, Germany) by the attending medical team. Failure criteria are shown in figure 1. Infants could receive increased pressure or flow if they met failure criteria and infants on nHF could be ‘rescued’ to nHF 8 L/min prior to being placed back on nCPAP. If nCPAP support of >6 cm water or nHF support of >8 L/min were required, then infants received rescue nCPAP until stability criteria were met and they recommenced their protocol as originally assigned. Infants who met failure criteria while off respiratory support recommenced weaning from step one of their originally assigned weaning arm. All infants were eligible for weaning again at 12:00 hours (see figure 1). Infants completed weaning by successfully remaining off respiratory support at 72 hours or reaching 36 weeks’ PMA (when our usual practice was to commence low flow oxygen).
The primary outcome was the duration of respiratory support (in hours) from randomisation until weaning was completed. Secondary outcomes were subgroup analysis of the duration of respiratory support for infants <27 weeks’ GA, CLD defined as any respiratory support or oxygen at 36 weeks’ PMA,23 nasal trauma (modified Fischer nasal trauma grading),5 age of first sucking feed, age when full sucking feeds was achieved (eight consecutive sucks with no top-ups), type of feeding at discharge, weight z scores24 and other neonatal morbidities (all defined as per local network guidelines).23 A validated parental stress and perception of infants’ treatment survey (Parental Stress Scale:Neonatal Intensive Care Unit, PSS:NICU)25 was given to parents at week 1 following randomisation and again at 36 weeks’ PMA. Infants discharged prior to 36 weeks’ PMA or those infants randomised after 34 weeks’ PMA only received one survey to complete.
The study was approved by the Northern A Health and Disability Ethics Committee (15/NTA/42) and local research committees. Informed written consent was gained from the parents when infants were approaching the predetermined stability criteria.
Statistical analysis
Sample size was determined by using observational data and bootstrapping (further described in the online supplemental file). A total of 100 infants (50 per arm) would provide a 92% power to conclude non-inferiority of the weaning time (one-sided significance test). A non-inferiority margin of 15% was chosen. To achieve the required sample size, it was planned to recruit 120 infants (60 per group).
Supplemental material
Statistical analysis was performed using R V.3.6.1.26 A non-inferiority one-sided alternative (significance level 2.5%) was used to test the primary hypothesis and a superiority two-sided alternative for secondary hypotheses.27
Independent predictors were investigated (gestational age at birth, patent ductus arteriosus, late-onset sepsis, maternal diabetes and a sibling factor which identified pairs of siblings). No interactions were included in the primary outcome model. Hours on respiratory support and gestation at birth were predictors included in time to suck analyses, and gestation at birth and a sibling factor for CLD analyses.
The primary outcome was analysed using a per-protocol (pp) analysis with time-to-event (survival) analysis including right censoring for those infants who remained on respiratory support at 36 weeks’ PMA (see online supplemental file for more detail). A restricted mean survival time was used for the primary outcome.28 To obtain this, a standard survival curve was estimated. A cut-point was chosen,29 by estimating the hazard at each event time, and searching for a point with the smallest sums of squared error for a model. This conservative approach allowed for different hazards between the two groups and the same hazard after the chosen time point.29 Subgroup analysis of <27 weeks’ GA infants was carried out in the same way. Treatment failure for example, failure of weaning, and other proportions were analysed using χ2 tests. There was no adjustment for missing outcome values. The PSS:NICU25 consists of four domains and a total score and was analysed using linear mixed modelling with Tukey correction. The data were collected from parents over two time points.
Results
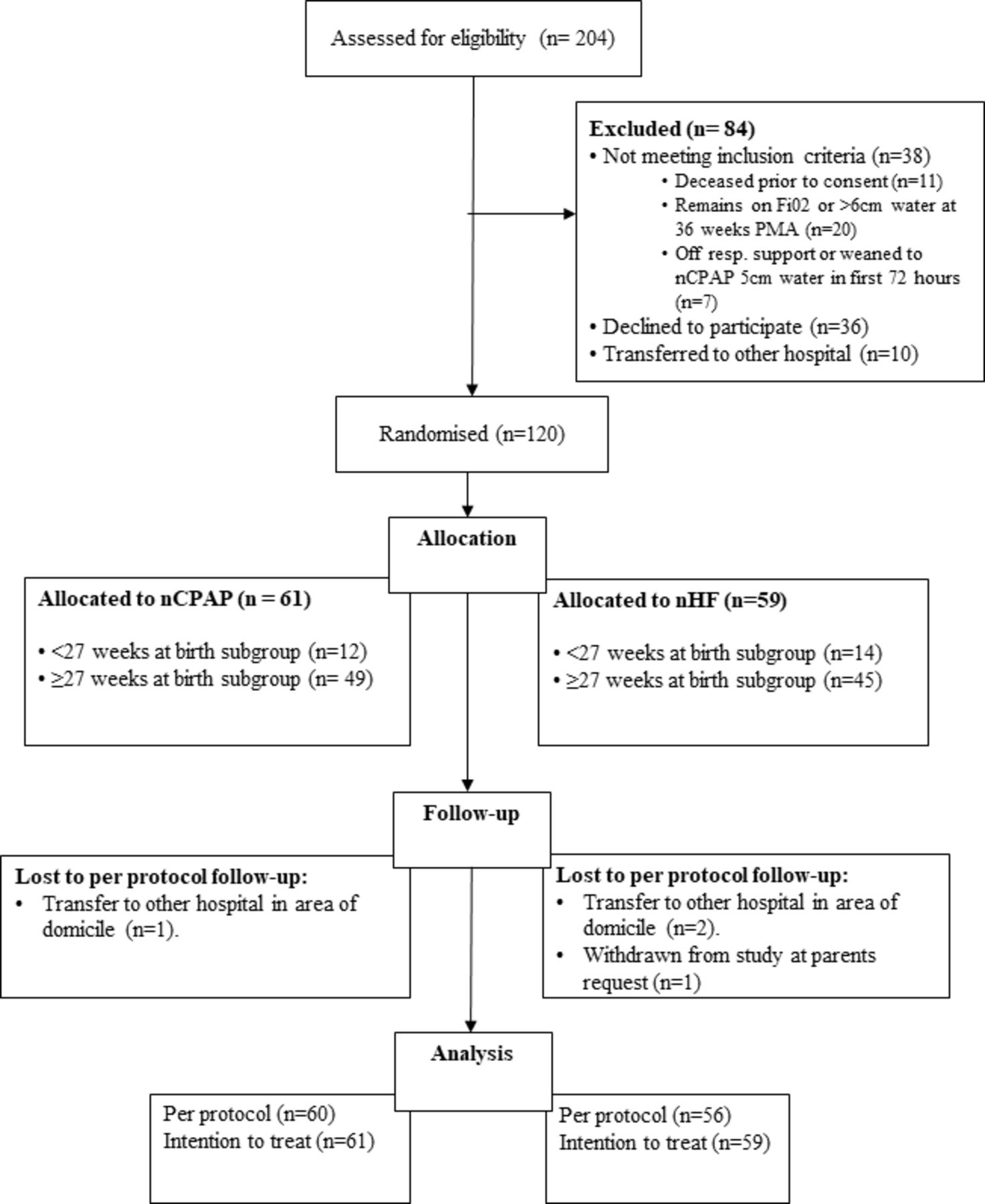
Two hundred and four infants were assessed for eligibility and 120 randomised; 61 to the nCPAP group and 59 to the nHF group. Four infants were excluded from the pp analyses, three transferred to other hospitals and one infant was withdrawn for parental request (figure 2). Of the 36 infants whose parents declined the study, there were no significant differences in important demographics compared with those randomised. Baseline demographics are shown in table 1.
Baseline maternal and infant characteristics
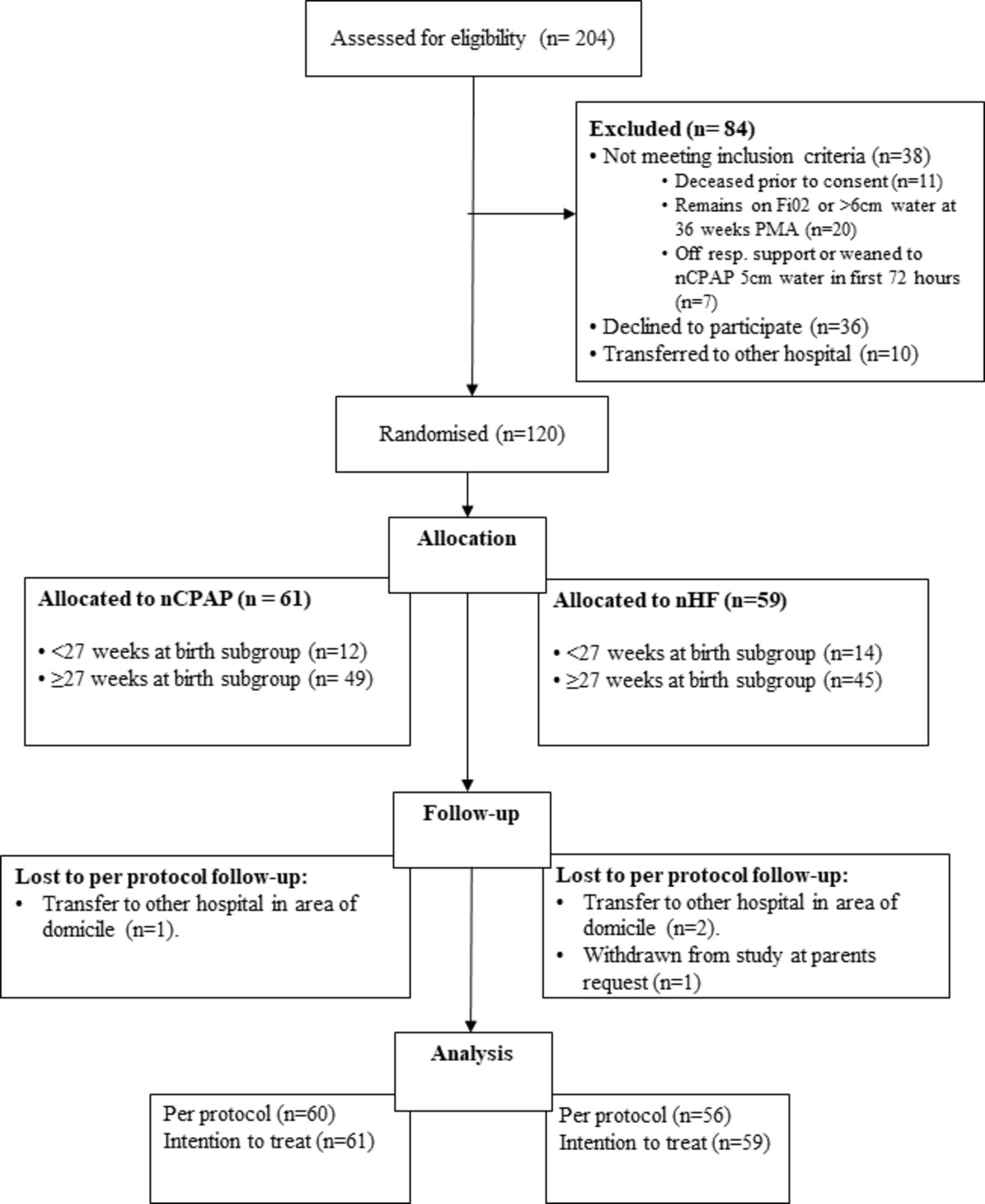
Consort diagram. Fio2, fractional inspired oxygen; nCPAP, nasal continuous positive airway pressure; nHF, high flow nasal cannula; PMA, postmenstrual age.
Primary outcome
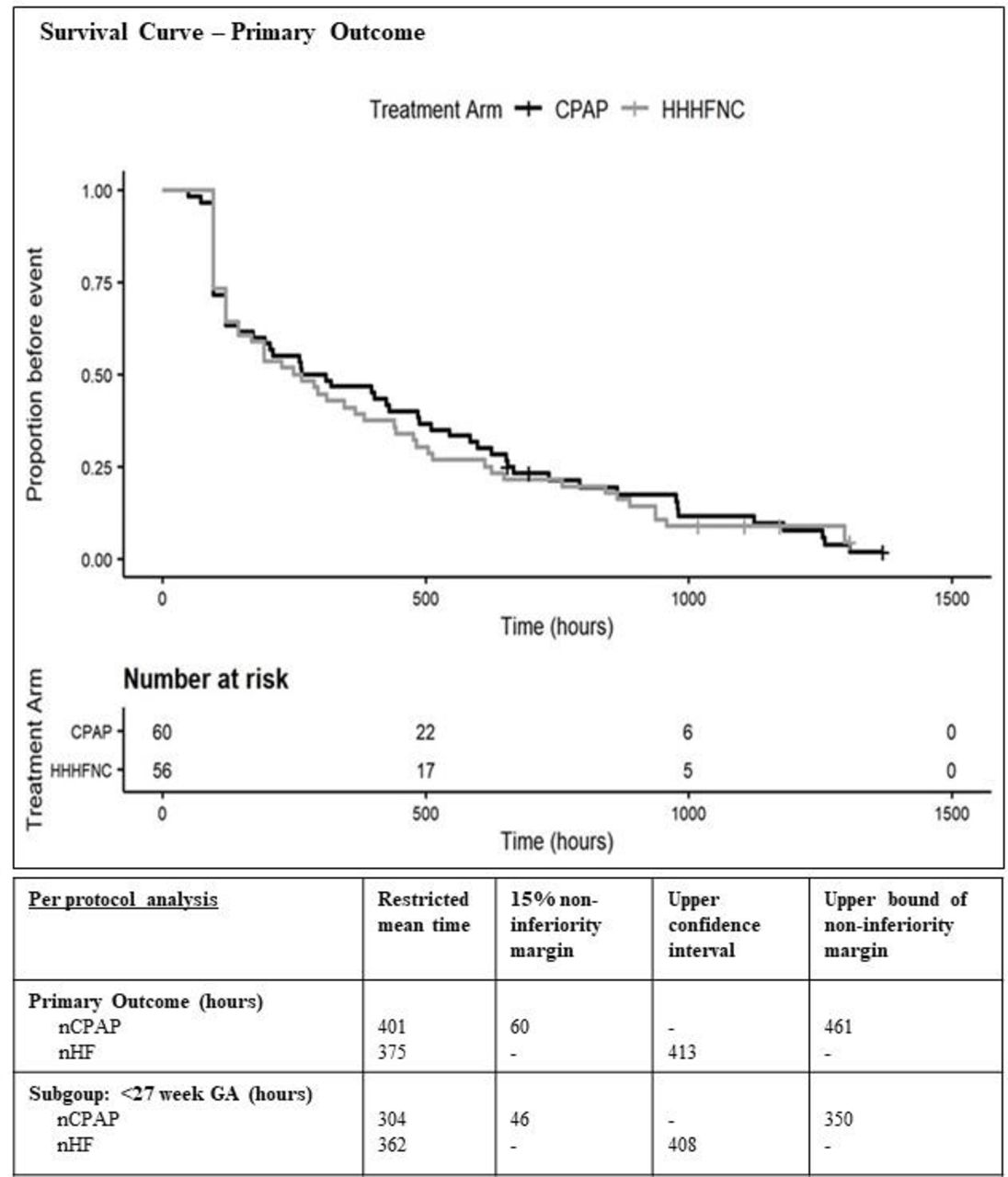
PP analysis of the primary outcome (duration of respiratory support following randomisation) is shown in figure 3, and the cut-point for the restricted mean was 888 hours. The restricted mean hours from randomisation to 72 hours off respiratory support or 36 weeks’ PMA was 401 hours in the nCPAP group giving an upper bound of 461 hours (mean plus 0.15 non-inferiority margin). The restricted mean in the nHF group was 375 hours with an upper CI of 413 hours, showing that nHF weaning was non-inferior to nCPAP weaning using the 15% non-inferiority margin (figure 3). An intention-to-treat analysis gave similar results (see online supplemental file).

{kind=link}
{kind=link}
{kind=link}
Time-to-event curves for nCPAP and heated humidified high flow groups with primary outcome data using restricted mean survival time analysis. GA, gestational age; HHHFNC, heated humidified high flow nasal cannula; nCPAP, nasal continuous positive airway pressure; nHF, high flow nasal cannula.
Thirty-two infants completed the primary outcome at 96 hours (15 nHF, 17 nCPAP). It can be seen in the survival curve (figure 3) that both arms did not diverge at this early stage.
Weaning
The first trial off respiratory support following randomisation was at a similar PMA in the two groups (median 31 weeks). On point estimates prior to successful trial off support suggested infants in the nHF group had a higher rate of escalating flow/pressure (52.5% vs 34.4%; OR 1.53 (95% CI 0.78 to 2.95)), however this was not statistically significant. Similarly, point estimates suggested reduced treatment failures prior to achieving 72 hours in the nHF group compared with nCPAP (24% vs 47.5%; OR 0.49 (95% CI 0.24 to 1.03)). The leading cause of treatment failure in both groups was desaturation/bradycardia. See table 2 for more detail.
Weaning and secondary outcomes
Secondary outcomes
In the <27 weeks’ GA subgroup, we were unable to conclude nHF non-inferior to nCPAP when weaning from nCPAP within a 15% non-inferiority margin (see online supplemental file for detail). Other secondary outcomes are listed in table 2. Infants in the nHF arm had significantly less CLD than those in the nCPAP arm (18% vs 36%; OR 0.42 (95% CI 0.18 to 0.99 corrected for gestation and sibling factor but not multiple comparison)). Other secondary outcomes listed in table 2 were not significantly different. There was a 95% return for the first PSS:NICU25 and a 77% (nCPAP) and 66% (nHF) return for the second PSS:NICU survey. Stress scores were reduced in the nHF group, in regards to the ‘relationship’ section of the survey (p=0.045; see online supplemental file and supplemental eTable for further discussion).
Supplemental material
Discussion
Weaning from CPAP is important—there are potential adverse outcomes for weaning too slowly (exposure to oxygen, CLD) but also for weaning too rapidly, for example, atelectasis, loss of functional residual capacity and inflammation.30 There remains a lack of consensus over how best to wean from CPAP.
Prior to this study, our usual nCPAP weaning strategy was to remove nCPAP once infants were stable in room air at a pressure of 5 cm water.31–33 We did not use lower pressures or cycling. A systematic review of nCPAP weaning indicated that this method of abrupt cessation significantly reduced the PMA of successful weaning.34–36 For a non-inferiority weaning study with the primary outcome being time of respiratory support, we chose a weaning method that resulted in the shortest time on support.
Owing to the potential benefits of nHF (ease of application, earlier introductions of suck feeds), our study design was a non-inferiority one—we reasoned if nHF weaning was non-inferior to our usual nCPAP weaning strategy, the other potential health benefits could make it a viable weaning tool.
We noted infants were more likely to wean successfully on the first occasion following the stepwise decrease in nHF rather than abrupt nCPAP cessation. This has been noted in other studies35 and may reflect the more graded steps carried out with nHF weaning. Although a similar gradation could be achieved with nCPAP, such an approach has not been shown to reduce the PMA at which nCPAP is discontinued.36 On the other hand, before being ready to trial off, infants on nHF required more interventions (increases in flow) than those on nCPAP; therefore, there was no overall difference in PMA at successful wean when comparing the two groups. Optimal nHF and nCPAP weaning might involve different mechanisms, but we found the overall time on support was similar. It is of interest that the PMA of nCPAP successful wean for infants <30 weeks’ GA has remained constant in our centre over the past 15 years, with this PMA reflected in a systematic review.37 Similar percentages (approximately 25%) in each group were successfully weaned off immediately after the initial 96 hours. In a post hoc analysis (see online supplemental file 1), we found that assuming the nCPAP group might have come off earlier for example, by 24 hours instead of 96 hours, did not alter the overall results.
There have been four published RCTs reporting on nHF as a strategy for weaning from nCPAP.11–14 There is considerable heterogeneity between these studies. Abdel-Hady et al 13 and Badiee et al 12 focused on duration of oxygen requirement and included infants born >28 weeks’ GA (mean 31 weeks’ GA). Infants were eligible for randomisation when they reached nCPAP 5 cm water in <0.30 fractional inspired oxygen, at which time they were randomised to a fixed nHF flow of 2 L/min or remained on nCPAP 5 cm water and weaning of oxygen was commenced. One study found the use of nHF lengthened time of exposure to oxygen and respiratory support13 and the other found a significant reduction in oxygen exposure using nHF and earlier time to discharge.12
Tang et al 11 reported no significant difference in days on respiratory support when nHF was used to wean from nCPAP . Soonsawad et al 14 reported that time to wean off nCPAP with the use of nHF was not different than weaning directly from nCPAP. Both the latter studies included infants born <28 weeks’ GA. In our cohort of infants <27 weeks’ GA, the non-inferiority threshold for our primary outcome was not met. This may be a reflection of the small numbers but requires further research as the study was not powered for this outcome and the analysis was exploratory.
Parents in the CHiPS study reported less stress in regards to the ‘relationship’ section of the survey, which included separation, contact and interaction with their infant while on nHF compared with nCPAP. This is similar to another study, where parents assessed nHF treatment as significantly better than nCPAP in three survey domains: child satisfied, parental contact and interaction and possibility to take part in care.16 Our PSS:NICU was an exploratory analysis, and the study was not powered for these outcomes.
Nasal trauma was uncommon in both groups. We did note a significant decrease in CLD in the nHF group. We did not find differences in either antenatal demographics or indicators of disease severity between groups to explain these results. However, the results are exploratory as the study was not powered for this outcome and adjustments were not made for multiple comparisons.
Strengths of the CHiPS study include a clear weaning algorithm, predetermined failure criteria, inclusion of infants with a GA of <27 weeks and the ability for nHF groups to be ‘rescued’ to nCPAP. The limitations include the fact that there were a small number of infants <27 weeks’ GA. The study was undertaken in one NICU and the weaning occurred at a set time of day. This could lengthen time on respiratory support for some infants, although the same limitation applied to both groups. Fifteen per cent of study infants were not able to be weaned from support during the study period.
The CHiPS study validates the use of nHF as a viable alternative method for weaning preterm infants from nCPAP when using predefined stability and failure criteria.
Data availability statement
All data relevant to the study are included in the article or uploaded as supplementary information. Study data is not available
Ethics statements
Patient consent for publication
Ethics approval
This study involves human participants and was approved by Northern A Health and Disability Ethics Committee (15/NTA/42). Participants gave informed consent to participate in the study before taking part.
Acknowledgments
The authors wish to acknowledge the contributions of the following people: Kelly Roczniak (BHSc), Neonatal Unit, Middlemore Hospital, Auckland; Alain C Vandal (PhD), Department of Statistics, The University of Auckland, Auckland and KoAwatea Research and Evaluation Office, Counties Manukau Health, Auckland; Mark Wheldon (PhD), Centre for Clinical Research, Counties Manukau Health, Auckland; Paula Massey (BHSc), Middlemore Hospital, Kidz First Research, Auckland; Christin Coomarasamy (MPhil, MSc), KoAwatea Research and Evaluation Office, Counties Manukau Health, Auckland; Maisie Mi-Chih Wong (FRACP), Neonatal Unit, Middlemore Hospital, Auckland; David Hou (FRACP), Neonatal Unit, Middlemore Hospital, Auckland and Department of Paediatrics: Child and Youth Health, The University of Auckland, New Zealand, and the staff and families at Middlemore Hospital Neonatal Intensive Care Unit, South Auckland, New Zealand.
References
Supplementary materials
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Footnotes
Contributors JC was responsible for the conduct of the study, had access to the data and made the decision to publish.
JC and MM: conceptualisation and design, methodology, investigation, funding acquisition, data curation, formal analysis and resources; MM: supervision/oversight. PC: conceptualisation/design, funding acquisition, methodology and formal analysis.
Funding This work was supported by KoAwatea Tupu Project Fund, Middlemore Hospital, South Auckland, New Zealand.
Competing interests None declared.
Provenance and peer review Not commissioned; externally peer reviewed.
Supplemental material This content has been supplied by the author(s). It has not been vetted by BMJ Publishing Group Limited (BMJ) and may not have been peer-reviewed. Any opinions or recommendations discussed are solely those of the author(s) and are not endorsed by BMJ. BMJ disclaims all liability and responsibility arising from any reliance placed on the content. Where the content includes any translated material, BMJ does not warrant the accuracy and reliability of the translations (including but not limited to local regulations, clinical guidelines, terminology, drug names and drug dosages), and is not responsible for any error and/or omissions arising from translation and adaptation or otherwise.
Linked Articles
- Highlights from this issue