Article Text

Abstract
Background Guidelines advise for more than 20 years to use occlusive plastic wraps for temperature management during delivery room care but data on efficacy of different types of wrap are still scarce.
Methods A random sample of seven different types of plastic wrap was tested using prewarmed aluminium blocks.
Results The most effective wrap increased the time to cool by 2°C by one-third for the core and by 100% for the surface whereas the least effective wrap led to even faster heat loss compared with no wrap at all. The least effective wrap concerning all capacities tested was made from polyurethane that contains potentially toxic and narcotic monomers. Heat and water retention did not correlate to wrap thickness.
Discussion Large differences in heat and water retention capacity warrant a careful choice of the type of wrap as some might be counterproductive. Wraps containing polyurethane should not be used.
- intensive care units
- neonatal
- toxicology
- emergency care
Data availability statement
Data are available upon reasonable request. Data are available to interested users for further corporate analysis.
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
What is already known on this topic?
Heat loss protection in the delivery room is important as it reduces mortality.
Therefore, plastic wraps are recommended by most guidelines to be used for immediate postnatal care of very low birthweight infants.
After more than 20 years data on the efficacy of different types of wrap are still scarce.
What this study adds?
Heat and water retention capacity varies widely with no correlation to the type of wrap or its thickness.
Wraps made from polyurethane cause an increased water and temperature loss compared with using no wrap and contain potentially toxic and narcotic monomers.
Introduction
Very low birthweight infants have an increased mortality when experiencing hypothermia.1 Because heat loss is caused mainly by evaporation the use of occlusive plastic wraps during their delivery room care has been recommended by different guidelines since 1999.1 2 In contrast, data concerning the efficacy of different types of wrap to retain heat and water are still not available. Solely, potentially toxic monomers of these wraps were described.3 4 Therefore, we tested a random sample of seven types of occlusive plastic wrap used by surrounding hospitals during delivery room care to study the differences in heat and water loss and related these data to the composition of the individual wraps.
Methods
Seven different types of plastic wrap were analysed: (a) freezer bag 4041055 (Melitta, Minden, Germany), (b) cling film (The Kestrel Group, Bristol, Great Britain), (c) cling film 4019769 (PrimeSource PE, Irving, Texas, USA), (d) drugstore food wrap, (e) 3M HealthCare 1003 (3M Medica, Neuss, Germany), (f) polyethylene (PE) occlusive wrap (Fisher & Paykel, Auckland, New Zealand), (g) Vi-Drape D37105510 (H&W, Glabbeek, Belgium). These were four individual bags and three single-layer films. Of all the seven, five consisted of PE only, one was a combined extrudate of PE and polyvinylidenchloride, and one consisted of polyurethane.
Heat loss
Two aluminium blocks of 983 and 548 g were equipped with one temperature probe on the surface and a second in the centre. After preheating to 36.9°C (±1.6°C) a block was completely covered with a single layer of one type of plastic wrap and moved to room temperature. Subsequently, the temperature of the block was measured every minute for 90 min (IntelliVue MP30, Philips, Germany). A data logger (Voltcraft DL-181THP, Conrad, Hirschau, Germany) continuously recorded air temperature, air pressure and humidity of the room. This process was repeated seven times with each type of wrap on each block.
Water loss
A 20×20 cm (±3 cm) washcloth was equally soaked with 20 mL of water and then wrapped in one of the plastic wraps using exactly 2.5 layers for wraps B, C, F and one closed bag for A, E, D, G. Immediately thereafter and after 23 hours at 37°C (±1°C), the weight of the package was determined. Measurements were repeated six times for each wrap.
Characterisation of wraps
Thickness of wraps was measured (a) from a 16 times folded wrap by micrometre screw and (b) by weighing a 400 cm² square and calculating thickness using the density of PE (0.925 g/cm³) and PU (1.2 g/cm³).
To characterise types of wraps, molar mass was determined by high-temperature gel permeation chromatography (Polymer Characterization, Valencia, Spain) at 150°C using 1,2,4-trichlorobenzene as solvent. Infrared absorption spectra were measured from a single layer of wrap (Bruker Vertex 80v, Bruker, Billerica, USA).
Statistics
Calculations were performed by Pearson correlation coefficient using MedCalc version 4.31.010 (MedCalc Software, Ostend, Belgium).
Results
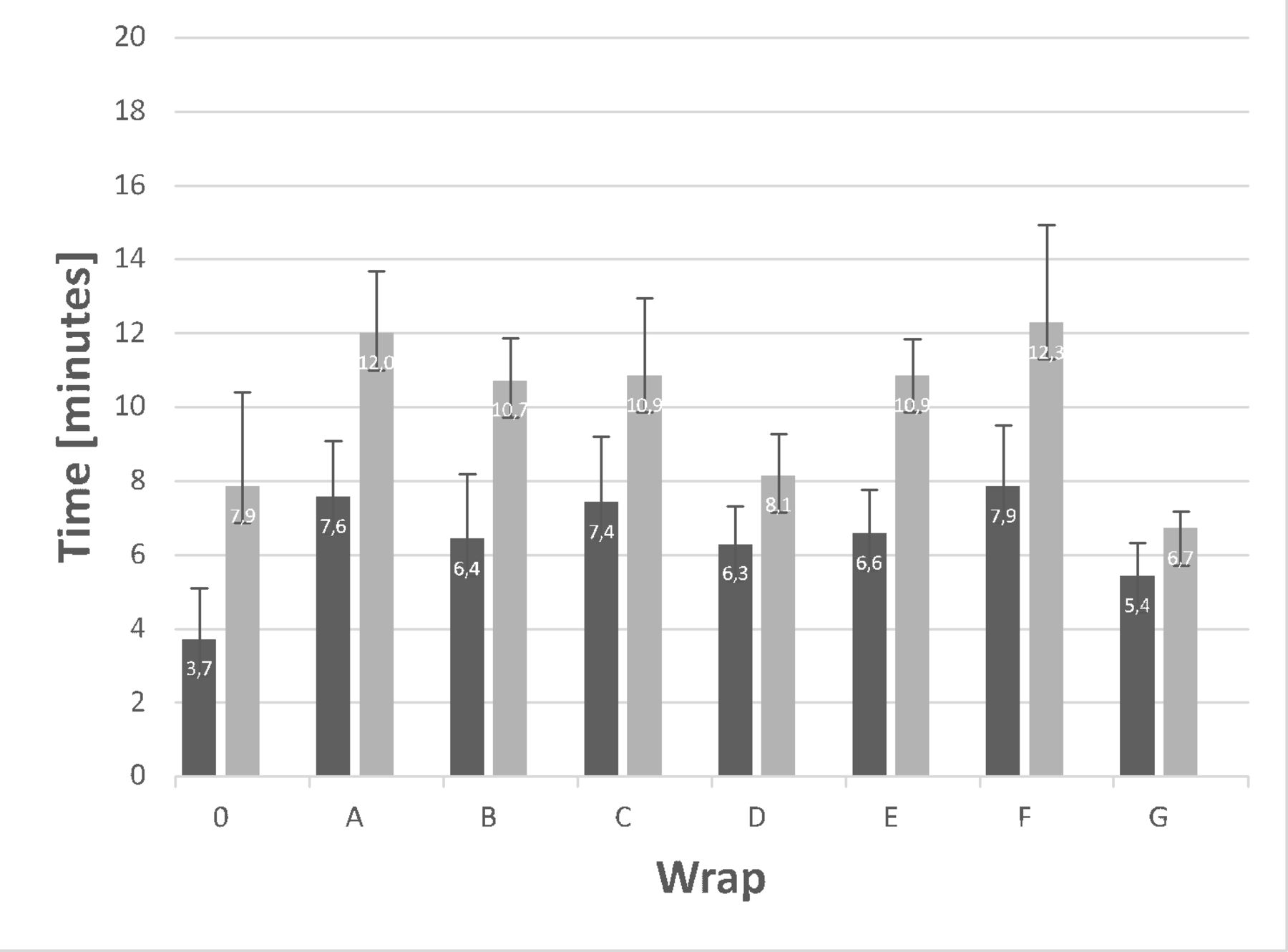
The core temperature of a 548 g aluminium block decreased by 2°C without a wrap within 8.1±2.4 min (figure 1). This time period increased to 11.1±2.5 min using the most effective wrap and decreased to 6.7±0.5 min using the least effective wrap. One of the other wraps showed no effect on the time compared with using no wrap and the remaining four wraps had an intermediate positive effect (figure 1). For the surface temperature, the most effective wrap almost doubled the time to lose 2°C, the other five wraps showed an intermediate positive effect. Time periods for a temperature loss of 5°C and when using a 983 g aluminium block were longer but comparable.

Heat loss from a 548 g aluminium block. Shown is the time in which the temperature on the surface (black) and core (grey) of a 548 g aluminium block decreased by 2°C when being wrapped with one of the wraps (A–G) or without a wrap (0).
Water loss within 23 hours without wrap was 20.3±0.2 g. This loss was reduced to 0.6±1.2 and 10.7±0.7 g with the most and least effective wrap, respectively (figure 2).

{kind=link}
{kind=link}
Water loss and thickness of wraps. Analysis of the seven different wraps showing the amount of water loss from a washcloth soaked with 20 mL of water being wrapped with one of the wraps (A–G) or without a wrap (0), the results of two different thickness measurements, the product description and their material by our analysis. Wrap B was discontinued while the study was in progress, the others are still in use in Germany. PE, polyethylene; PVdC, polyvinylidenechloride; PU, polyurethane.
Thickness of the seven wraps varied between 6.3 and 51.2 µm (figure 2). Both methods of measurement showed similar results except for the two thinnest wraps B and C, where for methodical reasons a difference of 23% and 19% was measured, respectively (Pearson r=0.998, p<0.0001). There was no correlation between wrap thickness and either temperature or water loss for any of the measurements (Pearson for water loss: r=0.70, p=0.08; for the 983 g aluminium block for 2°C core: r=−0.15, p=0.72; for 2°C surface: r=0.14, p=0.74).
High-temperature gel permeation chromatography and infrared spectrum proved five wraps to consist of PE only. Wrap E contains PE and polyvinylidenchloride, wrap G consists of polyurethane.
Discussion
While the use of occlusive plastic wraps during delivery room care has been recommended for more than 20 years by international guidelines, data regarding efficacy of different types of wrap are still scarce. In a prospective study, we found different types of wrap to be highly variable in their temperature and moisture retention capacity.
The high heat and water loss of wrap G is consistent with the fact that polyurethane is hydrophilic leading to higher water vapour permeability than PE or polyvinylidenchloride. Polyurethane will therefore absorb the water from the infant and emit it as vapour to the outside, thereby accelerating water and subsequently heat loss as seen in the results. This feature is the reason that polyurethane is often used for breathable textiles.
Soft plastics like occlusive wraps usually contain plasticisers that are absorbed by the body and their metabolites can be found in urine. Animal experiments found toxic effects of these materials.4 Therefore, polyvinylidenechloride (PVdC) containing materials like one wrap in our study should not be used in neonatal care. Another wrap consisted of polyurethane, a polycondensation product of 4,4'-bis(isocyanatophenyl)methane and 1,4-butanediol. The latter can be transformed in the body to gamma-hydroxybutyric acid which has a narcotic effect, the former is suspected to be carcinogenic.5 These toxic effects are another reason beyond its poor heat and water retention capacity to not use polyurethane wraps for newborn infants. Other hydrophilic plastics, such as cellophane, should also not be used for heat protection because they generally show poor water vapour retention.
Three of the PE wraps consisted of single-layer film and three were individual bags with both types having pros and cons. While bags keep an air cushion around the infant that should reduce water evaporation from the infant’s skin and thereby reduce heat transfer. On the other hand, single-layer wraps may be easier to apply and allow good access to individual body parts during delivery room care. Independent of these factors, the stiffness of the material may influence the feasibility to have a closed environment around the infant especially when it is moving.
The results of this study are limited as the wraps tested represent a random sample of those used in hospitals in Lower Saxony. Results may therefore not be transferable to other regions using other types of wraps. Also, tests were done objectively using aluminium blocks. Therefore, real stabilisation settings will be different due to radiant heating, air around the infant’s body or exposure of cool gas on its face through ventilatory support and movements of the infant. Nevertheless, the principal risks and benefits found should be transferable to other neonatal units.
Data availability statement
Data are available upon reasonable request. Data are available to interested users for further corporate analysis.
Ethics statements
Patient consent for publication
Acknowledgments
We would like to thank all the doctors and nurses of the NICU for their cooperation and help as well as Dr Richardson (Adelaide, Australia) for proofreading.
Footnotes
Contributors HK devised the study and the main conceptual ideas together with CR and PV. CR collected the data, performed calculations and drafted the manuscript with support from HK and PV. FE and PV did the wrap analysis. HK and PV reviewed the manuscript. All authors critically discussed the results and approved the final manuscript.
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Competing interests None declared.
Provenance and peer review Not commissioned; externally peer reviewed.