Article Text

Abstract
Background Therapeutic hypothermia is standard of care for babies with moderate/severe hypoxic-ischaemic encephalopathy and is increasingly used for mild encephalopathy.
Objective Describe temporal trends in the clinical condition of babies diagnosed with hypoxic-ischaemic encephalopathy who received therapeutic hypothermia.
Design Retrospective cohort study using data held in the National Neonatal Research Database.
Setting National Health Service neonatal units in England, Wales and Scotland.
Patients Infants born from 1 January 2010 to 31 December 2017 with a recorded diagnosis of hypoxic-ischaemic encephalopathy who received therapeutic hypothermia for at least 3 days or died in this period.
Main outcomes Primary outcomes: recorded clinical characteristics including umbilical cord pH; Apgar score; newborn resuscitation; seizures and treatment on day 1. Secondary outcomes: recorded hypoxic-ischaemic encephalopathy grade.
Results 5201 babies with a diagnosis of hypoxic-ischaemic encephalopathy received therapeutic hypothermia or died; annual numbers increased over the study period. A decreasing proportion had clinical characteristics of severe hypoxia ischaemia or a diagnosis of moderate or severe hypoxic-ischaemic encephalopathy, trends were statistically significant and consistent across multiple clinical characteristics used as markers of severity.
Conclusions Treatment with therapeutic hypothermia for hypoxic-ischaemic encephalopathy has increased in England, Scotland and Wales. An increasing proportion of treated infants have a diagnosis of mild hypoxic-ischaemic encephalopathy or have less severe clinical markers of hypoxia. This highlights the importance of determining the role of hypothermia in mild hypoxic-ischaemic encephalopathy. Receipt of therapeutic hypothermia is unlikely to be a useful marker for assessing changes in the incidence of brain injury over time.
- neonatology
- neurology
Data availability statement
Data are available in a public, open access repository. Data can be extracted from the NNRD.Details of how to access the National Neonatal Research Database may be found at: https://www1.imperial.ac.uk/neonataldataanalysis/data/utilisingnnrd/
Statistics from Altmetric.com
What is already known on this topic?
Therapeutic hypothermia has been the standard of care in the UK for moderate to severe hypoxic-ischaemic encephalopathy since 2009.
Increasing numbers of babies with mild hypoxic-ischaemic encephalopathy are treated with hypothermia in the USA and Canada; this is not known in the UK.
Receipt of therapeutic hypothermia is used as an indicator for brain injury occurring at or shortly after birth for national reporting in the UK.
What this study adds?
Between 2010 and 2017, the annual number of babies receiving therapeutic hypothermia with a diagnosis of hypoxic-ischaemic encephalopathy increased in England, Scotland and Wales.
An increasing proportion of babies treated with therapeutic hypothermia had a diagnosis of mild hypoxic-ischaemic encephalopathy or had less severe clinical characteristics of hypoxia.
Routinely recorded clinical data can be used to monitor changing treatment patterns at population level.
Introduction
Newborn hypoxic-ischaemic encephalopathy (HIE) is caused by insufficient oxygenation and blood flow to the brain and is an important cause of long-term disability.1 The incidence of moderate to severe HIE in the UK is between 2.4 and 2.8 per 1000 live births.2 For these infants, treatment with therapeutic hypothermia improves neurological outcomes among survivors up to 6–7 years of age without serious adverse effects.3 Therapeutic hypothermia for infants with moderate to severe HIE as defined in the original trials3 4 has been the standard of care in the UK since 2009.5
There is uncertainty about optimal care for infants with mild HIE. Randomised clinical trials of therapeutic hypothermia largely excluded infants with mild HIE, as reviewed here,6 7 and death or major disability was seen in 61% of babies who received therapeutic hypothermia in the original trials.3 Therefore, there are little randomised data to inform the use of therapeutic hypothermia in these babies. Retrospective observational studies suggest that infants with mild HIE have good outcomes without therapeutic hypothermia8 9; however, more recent prospective data suggest that mild HIE may be more closely linked with neurodevelopmental impairment than previously thought.9–12
In several developed countries babies with mild HIE are increasingly treated with therapeutic hypothermia,13–15 and there is interest in such treatment in the UK, including an ongoing dose-finding trial.16 A recent national UK survey of practice for babies with mild encephalopathy reported that 75% of responding centres offered therapeutic hypothermia to infants with mild HIE.17 Receipt of therapeutic hypothermia forms part of an indicator for brain injury occurring at or shortly after birth 2 in England, therefore changes in the population receiving hypothermia have potential to influence national reporting, and the benchmarking and quality improvement initiatives that rely on such data.
The aim of this study was to examine the temporal trends in clinical characteristics and graded severity of babies diagnosed with HIE who received therapeutic hypothermia in the UK between 2010 and 2017. Clinical classification of HIE severity displays variability among observers; the interobserver reliability coefficient was 0.87 for Thompson score,18 therefore clinical, physiological and biochemical markers were used to characterise the severity of hypoxia ischaemia that infants had been exposed to, in parallel with recorded grade of HIE.
Methods
We undertook a retrospective and descriptive cohort study using deidentified, routinely recorded neonatal clinical data held in the National Neonatal Research Database (NNRD).
Data source
The NNRD19 holds deidentified data from all infants admitted to National Health Service (NHS) neonatal units in England, Scotland and Wales (approximately 90 000 infants annually). In the UK, therapeutic hypothermia is not provided outside of NHS neonatal units. Data are extracted from neonatal electronic health records completed by health professionals during routine clinical care. A defined data extract, the Neonatal Dataset,20 of approximately 450 data items is transmitted quarterly to the Neonatal Data Analysis Unit where patient episodes across different hospitals are linked and data are cleaned (queries about discrepancies and implausible data configurations are fed back to health professionals and rectified). Completeness and accuracy of data held in the NNRD have been assessed in comparison with Case Record Forms from a multicentre randomised controlled trial which demonstrated high data agreement.19 Data items include demographic and admission items (clinical reason for admission), labour and delivery details (resuscitation and initial condition), daily items (seizures, ventilation, nitric oxide and inotropes administration) and discharge items (diagnosis at discharge). The individual components of HIE severity classification systems are not recorded in the NNRD.
Study population
Infants born between 1 January 2010 and 31 December 2017 and admitted to a neonatal unit in England, Scotland and Wales were eligible for inclusion in the study if (1) they had a recorded gestational age of ≥36+0 weeks+days at birth, (2) were recorded as having received therapeutic hypothermia for 3 or more days or died during this period, and (3) had a diagnosis of HIE made by the clinical team and recorded as either primary clinical reason for admission or principal diagnosis at discharge (online supplemental table 1). Demographic, antenatal, labour and delivery, birth and organisational characteristics (neonatal unit and transfers) were extracted from included babies (online supplemental table 2).
Supplemental material
Clinical characteristics
The aim of this study was to describe temporal trends in the clinical condition of babies diagnosed with HIE who received therapeutic hypothermia. Primary clinical characteristics recorded in the NNRD of interest were umbilical cord pH; Apgar score; newborn resuscitation; and seizures and treatment on day 1. The secondary characteristic of interest was recorded grade of HIE.
Clinical characteristics of interest to describe severity of hypoxia ischaemia were selected a priori and grouped into three categories: delivery stabilisation/resuscitation characteristics, condition at birth and condition on the first day of neonatal care (table 1). The latter clinical characteristic was used because clinical signs (such as seizures) and treatment (such as ventilation, inotropes and nitric oxide) are recorded in the NNRD as daily rather than time-stamped data. Apgar scores and umbilical cord pH were grouped into a priori specified categories. The NNRD data items used to define each clinical characteristic are listed in online supplemental table 3.
Clinical characteristics of hypoxia/ischaemia extracted from the NNRD
Grade of HIE
HIE diagnosis was extracted using the following variable fields: primary clinical reason for admission or principal diagnosis at discharge (see online supplemental table 1 for the data items used). The recorded grade of HIE was extracted using the principal diagnosis at discharge: mild or grade 1, moderate or grade 2 and severe or grade 3 HIE. The NNRD does not hold data describing the individual components of the neonatal neurological examination or that are used to classify severity of HIE.
Statistical method
Simple descriptive statistics were used to describe the study population, clinical characteristics and grade of HIE of the infants included in the study. Continuous variables were analysed using linear regression of the annual means followed by Spearman’s rank correlation to account for non-normality of the data. Ordinal variables were tested using Spearman’s rank correlation of the annual means. Binary data were assessed with a χ2 test for trend over the years (Cochran-Armitage test). For all the statistical results, a p value <0.05 was considered as statistically significant. Missing data were counted and presented in the tables but were disregarded in the statistical analysis of trends over time. All the statistical analysis was undertaken on SAS V.9.4 software (Statistical Analysis System, SAS Institute, 2013).
Sensitivity analyses
We undertook a sensitivity analysis to examine whether any temporal changes in the clinical characteristics of infants who received therapeutic hypothermia for HIE could be explained by changes in the classification of babies who received therapeutic hypothermia but did not have a diagnosis of HIE, for example, due to misclassification or where the diagnosis of HIE was not confirmed or not considered a primary or principal diagnosis. For this analysis, data from infants with a recorded gestational age of ≥36+0 weeks+days at birth, recorded as having received therapeutic hypothermia for at least 3 days or having died during this period but without a diagnosis of HIE, were analysed.
Results
Study population
A total of 6031 babies born between 1 January 2010 and 31 December 2017 in England, Scotland and Wales received therapeutic hypothermia for 3 consecutive days or died during the period of cooling; 830 babies did not have a diagnosis of HIE leaving 5201 babies who met the study inclusion criteria (figure 1).

Study flow diagram describing the process of selection and analysis. HIE, hypoxic-ischaemic encephalopathy; NNRD, National Neonatal Research Database.
The descriptive and clinical characteristics of babies diagnosed with HIE who received therapeutic hypothermia from 2010 to 2017 are presented in tables 2 and 3. The number of babies who had a diagnosis of HIE and received therapeutic hypothermia for 3 days or died increased from 2010 to 2015 before decreasing slightly in 2016–2017.
Annual summaries of the descriptive characteristics of selected babies from 2010 to 2017. SD, standard deviation
Annual summaries of the clinical characteristics of selected babies from 2010 to 2017
Initial condition at birth
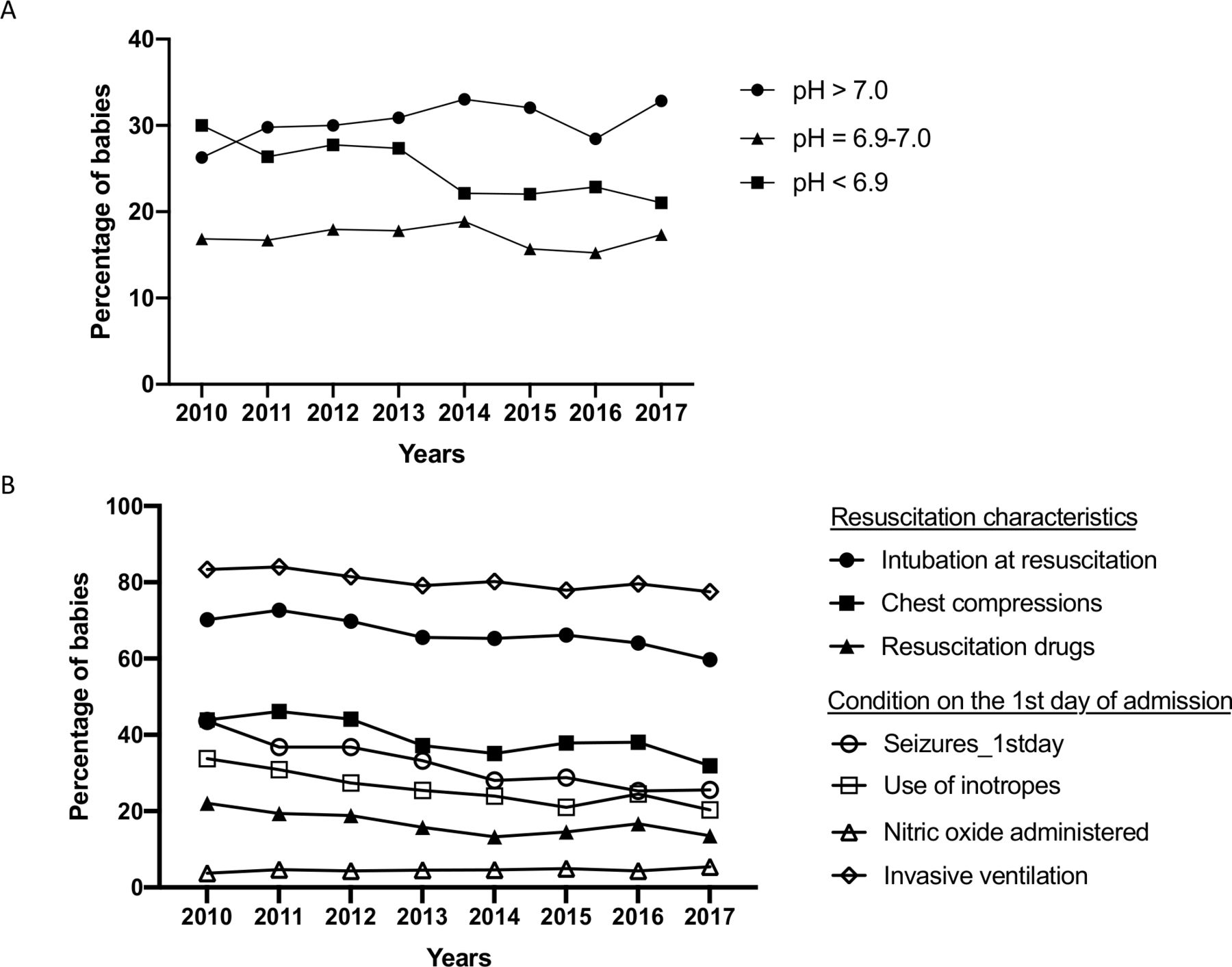
First analyses examined the temporal trends across multiple clinical characteristics related to severity of HIE in babies who received therapeutic hypothermia in the UK over the study period. Over the study period, we found evidence of an increasing trend in umbilical arterial cord pH over time (Spearman rank correlation test, p≤0.001). Results from the linear regression analysis indicated an average increase of 0.005 units in umbilical arterial cord pH per year of the study period (coefficient of 0.005, p≤0.001). The proportion and number of babies with an umbilical arterial cord pH greater than 7.0 who received therapeutic hypothermia for HIE increased, while the proportion and number of babies with an umbilical arterial cord pH of less than 6.9 decreased (table 3 and figure 2 and supplemental figure 1).

Line chart of the proportion of babies who had a diagnosis of hypoxic-ischaemic encephalopathy and received therapeutic hypothermia for 3 days or died during that period, by umbilical cord pH at birth (A), resuscitation characteristics and the condition on the first day of admission (B), from 2010 to 2017.
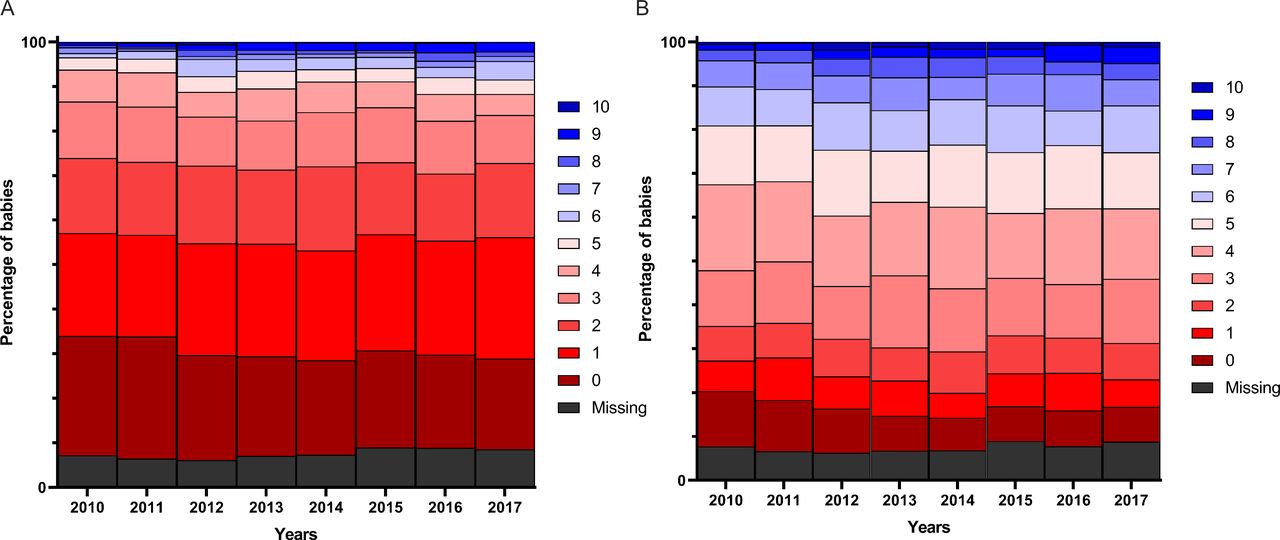
Over the study period, we found an increase in the recorded Apgar scores at 1 and 5 min (Spearman correlation test, p=0.007 and p=0.009, respectively) of babies with HIE who received therapeutic hypothermia (table 3 and figure 3 and supplemental figure 2).
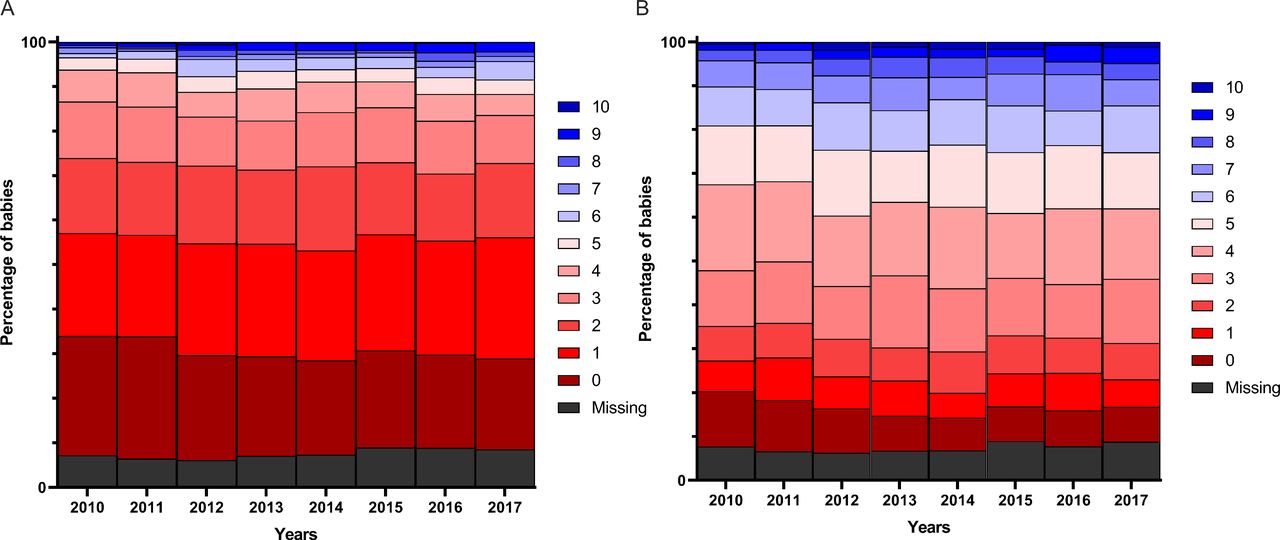
Bar charts of the proportion of babies who had a diagnosis of hypoxic-ischaemic encephalopathy and received therapeutic hypothermia for 3 days or died during that period, by Apgar score at 1 min (A) and 5 min (B), from 2010 to 2017.
Resuscitation and condition on the first day of admission
Over the study period, the proportion of babies with HIE who received therapeutic hypothermia or died and who were intubated, received drugs or chest compressions as part of newborn resuscitation decreased (χ2 test for trend, p≤0.001). There was also a decrease in the proportion of babies who had seizures recorded (p≤0.001) or who received inotropes (p≤0.001) or invasive ventilation (p≤0.001) on the first day. The proportion of babies who received inhaled nitric oxide on the first day was low and remained stable throughout the study period (χ2 test for trend, p=0.28) (table 3 and figure 3).
Quantification of HIE grades
Secondary analyses examined the temporal trends in the recorded HIE grade of babies who received therapeutic hypothermia in the UK. Over the study period, we found evidence of a decreasing trend in the recorded grade of HIE among babies in the study cohort (Spearman correlation analysis, p≤0.001). The proportions of babies who received therapeutic hypothermia or died and were recorded as having moderate (grade 2) or severe (grade 3) HIE decreased, while the proportion recorded as having mild (grade 1) HIE increased (figure 4 and online supplemental table 4).

{kind=link}
{kind=link}
{kind=link}
{kind=link}
Bar charts of the proportion of babies who had a diagnosis of hypoxic-ischaemic encephalopathy and received therapeutic hypothermia for 3 days or died during that period, by recorded severity of hypoxic-ischaemic encephalopathy, from 2010 to 2017. HIE, hypoxic-ischaemic encephalopathy.
Sensitivity analyses
Over the study period, 830 babies received therapeutic hypothermia but did not have a recorded diagnosis of HIE. The recorded diagnoses for these babies are presented in online supplemental table 5. Next, we wanted to assess whether changes in classification of babies over time explained temporal trends in the population of babies who received therapeutic hypothermia for HIE; for example, if mildly affected infants were increasingly classified as HIE rather than as other non-HIE diagnosis in later years. In order to do so, the described analyses were repeated on this cohort of babies (online supplemental table 6 and supplemental figure 3). Babies who received therapeutic hypothermia for 3 days or died during this period without a diagnosis of HIE had less severe markers of hypoxia ischaemia when compared with the study population with a diagnosis of HIE. The temporal trends seen in this non-HIE group are in the same direction and of the same order of magnitude as those seen in the primary analyses, indicating that changing diagnostic classification is unlikely to account for our findings.
Discussion
We show a temporal change in the clinical characteristics and recorded severity of HIE in babies who received therapeutic hypothermia in the UK between 2010 and 2017 despite there being no change to the clinical guidance for initiation and duration of neonatal therapeutic hypothermia over this period5: a greater proportion of these babies have less severe clinical characteristics of hypoxia ischaemia or are recorded as having mild (or grade 1) HIE. This pattern is consistent across several markers of hypoxia ischaemia comprising initial clinical assessment, resuscitation, biochemical markers, seizures and initial treatment, as well as in recorded grade of HIE. These data indicate that an increasing proportion of infants receiving therapeutic hypothermia in the UK have mild HIE and we find that a large number of infants are receiving therapeutic hypothermia without a principal or primary diagnosis of HIE. These infants are therefore receiving this therapy outside the scope of high-quality randomised evidence8 and guidelines.5
This ‘therapeutic creep’ towards treatment of mild HIE with therapeutic hypothermia that we document in the UK is in keeping with findings from North America,13 21 22 where in some healthcare systems over 75% of infants with mild HIE received therapeutic hypothermia23 and national data from the Canadian Neonatal Network where the rate of treatment also appears to be increasing.11 A similar pattern is seen internationally: a recent meta-analysis including studies from seven high-income countries found that 22% of infants who underwent therapeutic hypothermia only had mild HIE.24 Babies with mild HIE were excluded from the original hypothermia trials in part because adverse outcomes were thought to be rare in these babies.25 26 More recent data, however, suggest that adverse neurodevelopmental outcomes may be more common than previously documented10: an international prospective multicentre study follow-up of 43 infants with mild HIE found that 16% had disability at 18–22 months, and follow-up of 55 infants with mild HIE in Ireland and Sweden found significantly lower cognitive composite scores at 2 years when compared with healthy controls.27 Whether therapeutic hypothermia is effective in improving neurodevelopmental outcomes in babies with mild HIE is however unclear. Data from a non-randomised cohort study of 47 babies found improved magnetic resonance spectroscopy biomarkers in babies who received therapeutic hypothermia28; however, a systematic review and meta-analysis of 117 babies with mild HIE inadvertently recruited into trials targeting babies with moderate to severe HIE did not find evidence of benefit from therapeutic hypothermia; although low numbers meant that important benefit or harm could not be excluded.8 We also find a sizeable number of babies received therapeutic hypothermia without a principal or primary diagnosis of HIE. Administration of therapeutic hypothermia is not without adverse consequences,29 such as subcutaneous fat necrosis and impaired mother–infant bonding (particularly following postnatal transfer), and has health economic implications; therefore, there are ethical and practical considerations to administering such a treatment outside robust, evidence-based guidance. Data presented here indicate that infants with mild HIE are increasingly receiving therapeutic hypothermia in the UK, despite an absence of high-quality data supporting its use. This highlights the importance of undertaking large methodologically robust trials to determine the risks and benefits of therapeutic hypothermia in babies with mild HIE.30 31
Data from the NNRD are used for national and regional reporting of brain injuries occurring at or soon after birth in England as part of a national maternity ambition to make England the safest place in the world to give birth. Moderate to severe HIE is an important component of, and sizeable contributor to, such brain injuries nationally and is currently defined for this purpose in part by receipt of therapeutic hypothermia.2 The increasing application of therapeutic hypothermia to babies with mild HIE documented here means that many such babies are incorrectly classified as brain injuries occurring at or soon after birth. This has the potential to mask improvements in maternity care aimed at reducing the incidence of moderate to severe HIE.32 In light of these findings we suggest that the definition of moderate to severe HIE used when reporting of brain injuries occurring at or soon after birth in England be revisited.
Strengths of this study include the national, population-level coverage afforded by the data held in the NNRD, in contrast to many international studies that have reported trends within single networks. To reduce classification bias due to subjectivity of HIE staging systems we used clinical markers of hypoxia ischaemia in addition to recorded HIE grade with results that were consistent across both measures. We also performed sensitivity analyses of babies treated with therapeutic hypothermia but not diagnosed with HIE and found similar trends in clinical characteristics indicating that our findings are unlikely to be explained by changing patterns of diagnosis. Limitations include missing data, although the proportion of missing data was low, and that using routinely recorded clinical data meant that existing HIE grading systems could not be applied retrospectively from NNRD data due to the absence of key data fields for HIE grading. We therefore used recorded HIE grade; the quality of this and other diagnoses, including neonatal seizures, may vary between and within neonatal units. There is, however, no reason to suggest that the quality of such diagnostic reporting would change systematically over time within an established database such as the NNRD. All NHS neonatal units contributed to the NNRD from 2012 in England, and 2015 in Scotland and Wales, resulting in a higher proportion of missing data, particularly prior to 2012. This may explain the lower numbers of babies recorded as receiving therapeutic hypothermia in 2010 and 2011. MRI data could also have been used to evaluate severity of HIE in babies receiving therapeutic hypothermia. However, data from these investigations are not held by the NNRD, hence our reliance of clinical markers of severity and diagnostic grading. This study did not seek to examine neurodevelopmental outcomes of included babies.
We demonstrate that an increasing proportion of infants who received therapeutic hypothermia for HIE between 2010 and 2017 in England, Wales and Scotland had mild HIE or less severe clinical markers of hypoxia ischaemia. This indicates a ‘therapeutic creep’ in the UK in relation to increased therapeutic hypothermia for mild HIE outside its evidence base. This has implications for national reporting of brain injuries occurring at or soon after birth as receipt of therapeutic hypothermia is unlikely to be a useful marker for assessing changes in the incidence of brain injury over time. The capture of additional daily data items describing neurological condition within the NNRD would facilitate more accurate national monitoring of severity of HIE and treatment. There is a need for adequately powered clinical trials to evaluate the effectiveness and safety of hypothermia in this sizeable group of babies.
Data availability statement
Data are available in a public, open access repository. Data can be extracted from the NNRD.Details of how to access the National Neonatal Research Database may be found at: https://www1.imperial.ac.uk/neonataldataanalysis/data/utilisingnnrd/
Ethics statements
Ethics approval
Research ethics committee approval for the study was obtained from East Midlands-Leicester Central Research Ethics Committee (17/EM/0307) as an amendment to, and using data extracted for, the Optimising newborn nutrition during therapeutic hypothermia: an observational study using routinely collected data (NIHR16/79/03). Approval for inclusion of their data in this study was obtained from all English, Scottish and Welsh neonatal units. The National Research Ethics Service has approved the National Neonatal Research Database as a research database (16/LO/1093).
Acknowledgments
We are grateful to all the families who agreed to the inclusion of their baby’s data in the NNRD, the health professionals who recorded the data and the NDAU team, in particular Kayleigh Ougham.
References
Supplementary materials
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Footnotes
Twitter @lorysophie, @shaliniojha7, @DrDonSharkey, @NeenaModi1, @DrCBattersby, @DrCGale
Contributors The research question for this study was conceived by CG and developed by CG, JD, SO, CB and LSH. LSH, DJ and CB undertook the data extraction. LSH, DJ and NL undertook data analysis. NM leads the National Neonatal Research Database. LSH, DJ and CG drafted the first draft of the manuscript. All authors were involved in interpretation, review and revision of the draft manuscript and approval of the final version. LSH had full access to all the data in the study and take full responsibility for the integrity of the data and accuracy of the data analysis. CG is the guarantor and affirms that the manuscript is an honest, accurate and transparent account of the study being reported; that no important aspects of the study have been omitted; and that any discrepancies from the study as planned have been explained.
Competing interests JD reports grants from NIHR, during the conduct of the study, and grants from NIHR, outside the submitted work. JD was a member of the NIHR HTA General Board (from 2017 to 2018) and the NIHR HTA Maternity, Newborn and Child Health Panel (from 2013 to 2018). JD was also funded by Nutrinia in 2017 and 2018 for part of his salary to work as an expert advisor on a trial of enteral insulin. SO reports grants from the National Institute of Health Research, Medical Research Council, and the Derby Hospitals Charity. DS reports grants from the National Institute for Health Research, Medical Research Council, Engineering and Physical Sciences Research Council, outside the submitted work. He is also a committee member of the NIHR Research for Patient Benefit East Midlands Regional Assessment Panel and a non-executive director of SurePulse Medical. NM reports grants from the Medical Research Council, National Institute of Health Research, March of Dimes, British Heart Foundation, HCA International, Health Data Research UK, Shire Pharmaceuticals, Chiesi Pharmaceuticals, Prolacta Life Sciences and Westminster Children’s Research Fund, outside the submitted work. She is a member of the scientific advisory board of Nestle International. NM led the development of and directs the National Neonatal Research Database. CG reports grants from Medical Research Council, the National Institute for Health Research, the Mason Medical Research Foundation, Rosetrees Foundation and Canadian Institute for Health Research, outside the submitted work; and grants and personal fees to attend an educational conference from Chiesi Pharmaceuticals, outside the submitted work; he is a voluntary, unremunerated member of the Neonatal Data Analysis Unit Steering Board, which oversees the National Neonatal Research Database (NNRD), and is vice-chair of the NIHR Research for Patient Benefit London Regional Assessment Panel.
Provenance and peer review Not commissioned; externally peer reviewed.
Supplemental material This content has been supplied by the author(s). It has not been vetted by BMJ Publishing Group Limited (BMJ) and may not have been peer-reviewed. Any opinions or recommendations discussed are solely those of the author(s) and are not endorsed by BMJ. BMJ disclaims all liability and responsibility arising from any reliance placed on the content. Where the content includes any translated material, BMJ does not warrant the accuracy and reliability of the translations (including but not limited to local regulations, clinical guidelines, terminology, drug names and drug dosages), and is not responsible for any error and/or omissions arising from translation and adaptation or otherwise.
Linked Articles
- Fantoms