Article Text

Abstract
Objective Economic evaluation of computerised decision-support software intended to assist in the interpretation of a cardiotocography (CTG) during birth.
Design Individual patient level data from the INFANT study (an unmasked randomised controlled trial).
Setting Maternity units in the UK and Ireland.
Population Singleton or twin pregnancy women of 35 weeks’ gestation or more and receiving continuous electronic fetal monitoring during labour.
Intervention Computerised decision-support software.
Methods Cost-consequence analysis presenting costs and outcomes with a time horizon of 2 years from a government healthcare perspective. Unit cost data collected from a combination of primary and secondary sources.
Main outcome measures Primary clinical outcomes were (i) composite ‘poor neonatal outcome’ and (ii) developmental assessment at age 2 years in a subset of surviving children. Mean cost per mother and infant dyad from birth to hospital discharge, and from hospital discharge to 24 months follow-up. Maternal health-related quality of life was assessed at 12 and 24 months follow-up using the EuroQol three-level health-related quality of life instrument (EQ-5D-3L).
Results Data were analysed for 46 042 women and 46 614 infants. No statistically significant differences were detected between trial arms in any of the primary clinical outcomes or maternal quality of life. No statistically significant differences in costs were detected in maternal or infant costs from trial entry to hospital discharge or overall from hospital discharge to 2-year follow-up.
Conclusions Decision-support software during labour is not associated with additional maternal or infant benefits and over a 2-year period the software did not lead to additional costs or savings to the National Health Service.
Trial registration number ISRCTN98680152.
- health economics
- costing
- fetal medicine
- monitoring
- health services research
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
What is already known on this topic?
Continuous electronic fetal heart rate monitoring in labour is widely used across the National Health Service (NHS) hospitals.
The use of decision-support software in the interpretation of the cardiotocography in women undergoing fetal heart rate monitoring does not improve clinical outcomes for mothers or babies.
It is not clear whether the use of decision-support software leads to potential savings to the NHS.
What this study adds?
The use of decision-support software during labour did not lead to additional costs or savings to the NHS over the study period.
Clinical and economic evidence suggest the systematic use of computerised interpretation of cardiotocography in women during labour should not be supported.
Introduction
Continuous electronic fetal heart rate monitoring in labour is widely used across National Health Service (NHS) hospitals and computerised interpretation could potentially inform attending caregivers about abnormalities in fetal heart rate patterns.1 Data about abnormalities such as asphyxia could assist caregivers to act or to accelerate delivery to prevent poor outcomes for babies or mothers.2 3 INFANT (K2 Medical Systems, Plymouth, UK) is a decision-support software developed to interpret fetal heart rate information during labour.4 It analyses data from the cardiotocography (CTG) and conducts an evaluation of the overall pattern creating a colour-coded alert where needed (blue is the least severe, yellow is moderate severity and red is the most severe). The clinical effectiveness of INFANT was recently evaluated in a large randomised controlled trial which recruited 46 042 women in labour in the UK and Ireland.5 The study did not detect differences in the incidence of poor neonatal outcomes at birth or in terms of developmental assessment at age 2 years between the groups.5 In this manuscript, we assess the economic implication of these outcomes for the UK NHS and conduct a cost-consequence analysis alongside the INFANT study.
Methods
Study population
The study population was women in labour in maternity units in the UK and Ireland. Women who were having continuous electronic fetal monitoring in labour were eligible if they had a singleton or twin pregnancy, and were 35 weeks’ gestation or more. They were allocated to receive decision support using the INFANT software or no decision support. Between 6 January 2010 and 31 August 2013, 47 062 women were randomised to the INFANT trial from the participating centres. Of these, data were analysed for 46 042 women and 46 614 infants. Further clinical design and review details including the eligibility criteria, sample size calculations, exclusions, statistical analyses and administrative processes are reported elsewhere.5 6
Study perspective and time horizon
A cost-consequence analysis was conducted, and we present resource use, costs and selected outcomes in a disaggregated form.7 8 The time horizon mirrors the follow-up duration for the trial, which identified women during labour and was completed for mothers and babies at 24 months postbirth. An NHS perspective was taken, and only direct healthcare costs were considered.
Health outcomes
Two clinical primary outcomes of the trial and a maternal health-related quality of life (HRQoL) were included in the analysis. The first primary outcome was a composite of ‘poor neonatal outcome’ (binary present or not present) including deaths (intrapartum stillbirths plus neonatal deaths up to 28 days after birth, except deaths due to congenital anomalies) and significant morbidity (moderate or severe neonatal encephalopathy, defined as the use of whole-body cooling or admission to the neonatal unit within 48 hours of birth for 48 hours or longer associated with evidence of feeding difficulties or respiratory illness, and evidence of compromise at birth suggesting mild asphyxia or mild encephalopathy, or both). The second was a continuous outcome of ‘developmental progress’ captured using the Parent Report of Children’s Abilities-Revised (PARCA-R) composite score at age 2 years for a subset of approximately 7000 children who did not have the composite primary outcome at birth.9 Maternal HRQoL information was collected using the EuroQol three-level HRQoL instrument (EQ-5D-3L) at 12 and 24 months follow-up.10 The EQ-5D-3L identifies 243 different health states that can be converted into a continuous preference-based score (0 death, −1 full health) using a value set obtained from a representative sample of the British general population.11
Healthcare resource use
A comprehensive list of healthcare resource use information for mothers and their babies was collected for the study. Data collection commenced when women arrived in hospital in labour and ended when postnatal care for both mother and baby was completed. For most women, this was following hospital discharge. A subset of women who consented to be followed-up postbirth were sent a questionnaire regarding healthcare resource use and maternal quality of life at 12 and 24 months follow-up.
Labour-related resource use data included procedures undertaken for mothers and infants before discharge and were collected using the Guardian System (an electronic capture system for managing information from monitoring during labour).12 Additional information such as maternal transfers after birth, the admission of babies or mothers to a higher level of care and neonatal deaths were collected using bespoke data collection forms.
Healthcare utilisation at 12 and 24 months postbirth was identified using a postal questionnaire that collected information about acute and secondary care, community care and maternal HRQoL. It included outpatient appointments and inpatient stays (eg, for operations), follow-up care and number of visits to relevant healthcare professionals. The questionnaires were sent to a subsample of women with surviving infants who had given birth in the first year of the trial and had consented to follow-up. The 12-month follow-up questionnaire collected resource use data between postbirth discharge and 1 year, and the 24-month questionnaire asked about resources used in the previous 12 months. Table 1 shows the categories of NHS healthcare resource use collected during the study.
Categories of resource use and associated unit costs used in the cost analysis (expressed in 2017–2018 UK prices)
Unit costs
Information was extracted from secondary national sources including the Personal Social Services Research Unit and the NHS Reference costs.13 14 Unit costs associated with induction, episiotomy, perineal tear, manual removal of the placenta, blood transfusions and neonatal death were not available in the secondary data sources consulted. ‘Bottom-up’ costing methods were replicated from another perinatal economic evaluation for these resource use categories (see online supplementary information).15
Supplemental material
In our base case analysis, no specific price for the decision-support software was assigned. We explored the impact of assigning prices and maintenance fees to the cost of decision-support software in a sensitivity analysis (see online supplementary information).
All costs were expressed in 2017–18 pounds sterling, inflated using the most recent Hospital and Community Health Service Inflation Index.12 Costs incurred between 12 and 24 months follow-up were discounted at an annual rate of 3.5% as recommended by current guidance.16
Cost analysis
Resource use categories and associated costs are presented separately for mothers and babies for each trial arm. Analyses were by ‘intention to treat’ indicating that the costs incurred were attributed to the original trial arm. Costs from postbirth discharge to 12 months, and 12–24 months were combined to estimate the overall costs at 2 years postbirth. Categories of resource use costing <£1 and prescribed medications were excluded from the analysis. Given the number of participants used to estimate costs to hospital discharge and to 2 years’ follow-up were different, an overall total cost over the trial period was not calculated.
Statistical analysis
A comprehensive report of the statistical analysis of the primary outcomes in the clinical trial are presented elsewhere.5 6 The composite of poor neonatal outcomes and PARCA-R between treatment arms were compared using risk ratios and parametric 95% CIs. Parametric and non-parametric methods accurately estimate the true SEMs when large sample sizes for continuous variables are used even when the data are highly skewed.17 Thus, mean differences and 95% CIs between treatment arms for EQ-5D-3L scores, healthcare resource use and costs were estimated using parametric methods. Differences between treatment arms were adjusted using a random intercept binomial (for risk ratios) or linear (for mean differences) model adjusting for the stratification factors at randomisation centre, and clustering due to twins and multiple birth episodes. A 95% significance level was used in all the comparisons.
All categories of resource use to hospital discharge had <5% missing data except for manual removal of the placenta and infant resuscitation. In this case, a cost analysis was conducted using a complete case analysis and mean estimates were accompanied by SD for each category of resource use in each treatment arm. A larger proportion of missing data was identified in the 12 and 24 months follow-up cohort and a multiple imputation framework with a chained equation was prepared using the recent guidance for handling missing data in cost-effectiveness analysis (see online supplementary information).18 19
Results
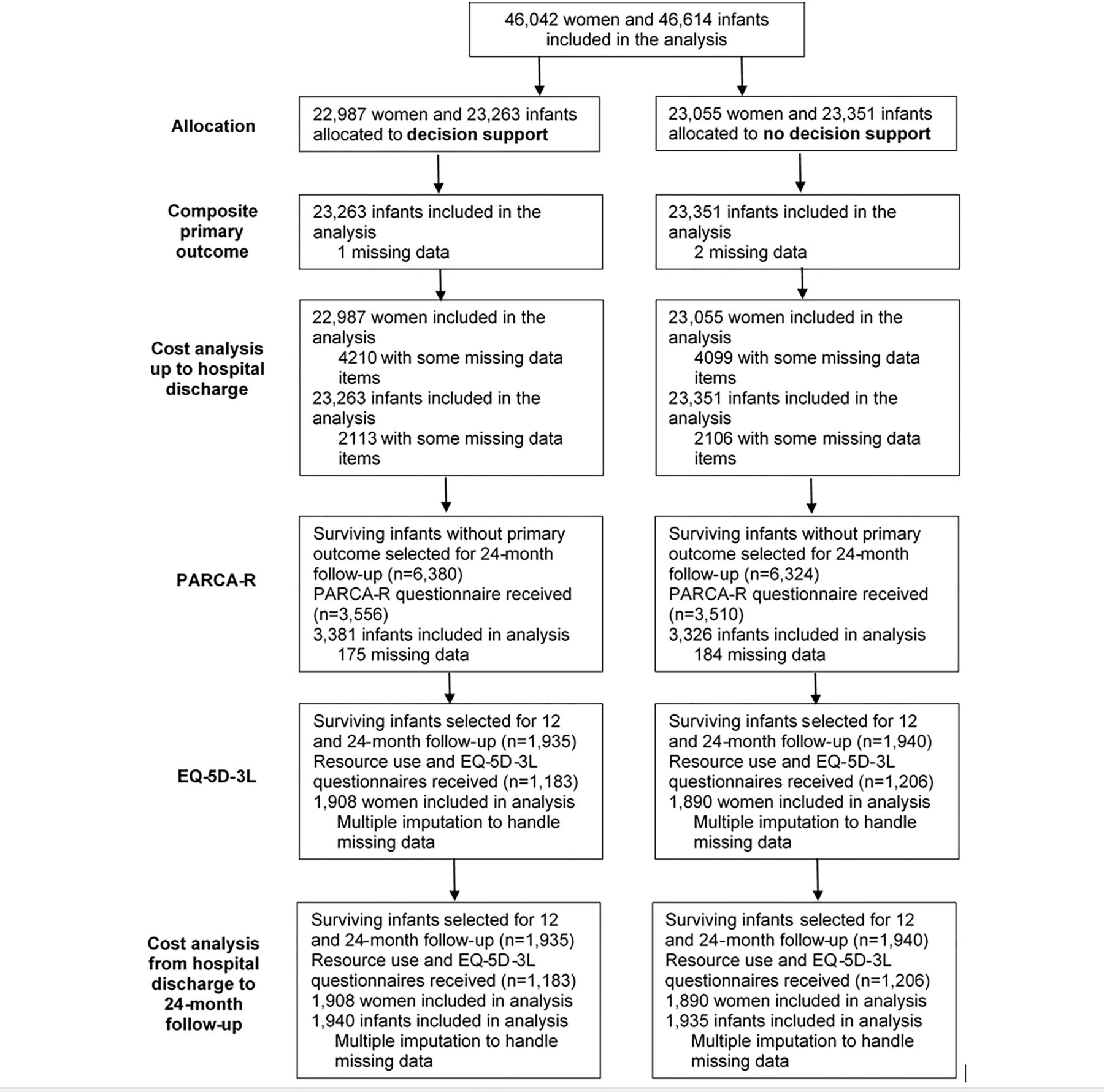
Figure 1 presents the flow chart of participants and the sources of information used for each component of the cost-consequence analysis. All women and infants participating in the trial were incorporated into the cost analysis to hospital discharge. A subset of 12 704 of surviving babies without the composite primary outcome were identified and a questionnaire to include PARCA-R developmental measures was sent at 24 months follow-up. Healthcare resource use and maternal HRQoL questionnaire at 12 and 24 months follow-up was sent to a subset of 3875 women with surviving babies. A total of 2389 (62%) completed questionnaires were received from this subset.
{kind=link}
Flow of participants and data availability included in each component of the cost-consequence analysis. EQ-5D-3L, EuroQol three-level health-related quality of life instrument; PARCA-R, Parent Report of Children’s Abilities-Revised.
The INFANT study reported similar baseline characteristics between the two groups.5 Online supplementary table S1 presents maternal characteristics for the entire trial cohort, for the subset responding to the PARCA-R questionnaire and the cohort completing the healthcare resource use and quality of life questionnaires. We observed differences in some baseline characteristics between the three subgroups with women responding to the developmental assessment and maternal quality of life and health resource use questionnaire more likely to be white, at term and without epidural analgesia.
Health outcomes
No evidence of a difference in the incidence of the primary outcome of poor neonatal outcome between the groups was observed, with 0.7% (172) babies having a poor outcome in the decision-support group compared with 0.7% (171) babies in the no decision-support group (adjusted risk ratio 1.01, 95% CI 0.82 to 1.25) (table 2). There was no evidence of a difference in any component of the composite primary outcome between the groups or in any of the trial’s secondary outcomes for the baby.5 At 24 months follow-up, there was no evidence of a difference between the two groups for the developmental primary outcome (table 2). The mean PARCA-R (SD) score in the decision-support group was estimated to be 98.0 (33.80) compared with 97.2 (33.41) in the no decision-support group (mean difference 0.63, 95% CI −0.98 to 2.25). Table 2 also presents information about maternal HRQoL using EQ-5D-3L scores at 12 and 24 months follow-up. Mothers reported scores that are similar to the English female population norm aged 25–34 years (currently 0.907) in both groups. No statistically significant mean differences in scores were observed at any follow-up point.
Summary of infant and maternal health outcomes included in the cost-consequence analysis
NHS healthcare resource use and costs
No significant differences were detected in any category of maternal and infant healthcare resource use from trial entry to postnatal hospital discharge (online supplementary tables S2 and S3). Online supplementary table S4 shows the results of the maternal and infant cost analysis from trial entry to hospital discharge. The total mean (SD) maternal costs from trial entry to hospital discharge was estimated to be £4083 (£1520) and £4062 (£1043) in the decision and no decision-support groups, respectively, a non-significant mean adjusted cost difference (95% CI) of £22 (−£5 to £49). The total mean (SD) for costs for infants from trial entry to hospital discharge was estimated to be £225 (£1891) and £243 (£2355) in the decision-support and no decision-support groups, respectively, a non-significant mean adjusted cost difference (95% CI) of −£18 (−£59 to £23).
Online supplementary tables S5 and S6 present the results of the maternal and infant healthcare resource use and associated costs over 24 months since hospital discharge. A significant adjusted mean cost difference (95% CI) was observed in the secondary care for mothers of −£194 (−£373 to −£15) favouring the decision-support group. Such difference was driven by slightly more admissions in the no decision-support group. However, when adding up all categories of costs (community plus secondary care), the total mean (SE) maternal follow-up costs was estimated to be £743 (£40) and £922 (£84) in the decision support and no decision support groups, respectively, a non-significant mean adjusted cost difference (95% CI) of −£178 (−£364 to £8).
A summary of the maternal and infant cost analysis included in the cost-consequence analysis is reported in table 3. For each of the maternal and infant total mean cost components from trial entry to 24 months follow-up, no statistically significant differences were observed between the groups, except for the secondary care for mothers as discussed above.
Summary of maternal and infant cost analysis included in the cost-consequence analysis over study period (expressed in 2017–18 UK prices)
The results of the sensitivity analysis identified that between a price of £11 and £12 per delivery the mean maternal cost difference from trial entry to discharge between treatment arms became statistically significant favouring no decision support (online supplementary table S7).
Discussion
This cost-consequence analysis is the first economic evaluation of decision-support for continuous electronic fetal monitoring for women in labour. We conducted an individual participant-level analysis using data collected as part of the INFANT randomised controlled trial. INFANT is the largest trial in the field of decision support for the interpretation of the CTG during birth. The large sample (46 042 women), the pragmatic methodological approach and the number of UK and Irish centres participating confirm the high internal validity and generalisability of the study.
The cost analysis included a very thorough description of the healthcare resource for mothers and their babies from trial entry to hospital discharge and up to 2 years follow-up. To reduce the burden of the microcosting however, we did not attempt to cost categories of resource use of <£1 and prescribed medications. For example, the clinical paper reported a significant difference in the number of fetal blood sampling in the decision-support arm compared with the control arm.6 However, except for consumables costing <£1, most of the costs attributable to fetal blood sampling is included in the mode of birth costs. Therefore, including these consumables in our cost analysis would have had a negligible impact on our results. A microcosting analysis of prescribed medication taken was also not undertaken because no significant differences between the two groups were observed in the proportion of medications and the number of courses prescribed for mothers or babies.
Due to the study’s large sample size, it was not administratively feasible to collect healthcare resource use and EQ-5D-3L information for the full sample to follow-up. Therefore, a subsample was recruited following the first women recruited to the trial (except babies with the primary outcome) to ensure data were available to analyse the primary and secondary outcomes closer to the end of recruitment for the whole study. In our subsample, we observed statistical significant differences in the demographic characteristics of the women who completed the questionnaires and non-responders. However, the magnitude of these differences was too small to have any clinical significance. We also asked mothers about healthcare utilisation over the previous 12 months, which may be subject to recall bias.20 This was based on evidence that recall period should not exceed 12 months21 and to minimise data collection efforts for the trial team due INFANT’s sample size.
Maternal HRQoL could not be collected at baseline preventing the calculation of maternal quality-adjusted life years (QALYs) over the trial period. There are still methodological challenges about the use of cost-utility analysis in maternal and perinatal health.22 23 The use of infant HRQoL methods for QALY estimation are still unresolved and there is still no consensus among health economists about the appropriate methodology to incorporate QALYs from different stakeholders into a meaningful measure for decision making.24 Given these, we opted to report the results of the economic evaluation using a cost-consequence analysis to present costs and consequences for mother and babies in disaggregated form. Similar approaches have recently been used in reporting economic evaluations for interventions in perinatal and maternal health.25 26
This cost-consequences analysis fills an evidence gap regarding the use of decision support in the form of computerised interpretation of the CTG for women receiving continuous electronic fetal monitoring during labour. We have shown that the use of a decision-support software during labour is not associated with additional maternal or infant benefits when compared with a control group. The use of this decision-support software did not lead to additional costs or savings to the NHS over a 2-year period.
References
Footnotes
ES and OR-A are joint first authors.
Contributors ES was a co-investigator of the INFANT trial and was responsible for the original health economic study design. ES and OR-A contributed to the health economics analysis plan, conducted the statistical analyses, wrote the manuscript and revised and approved the final version for submission. ES collected the unit cost data for the study with updates from OR-A and MY. MY conducted aspects of statistical analysis and revised and approved the final version for submission. PB was the Principal Investigators of the INFANT trial, secured funding for the study, contributed to the design of the health economics analysis plan and revised and approved the final manuscript for submission. LL conducted aspects of the statistical analysis and revised and approved the final version for submission.
Funding This project was funded by the NIHR HTA programme (project number 06.38.01). This report presents independent research commissioned by the National Institute for Health Research (NIHR). The views and opinions expressed therein are those of the authors and do not necessarily reflect those of the HTA Programme, NIHR, NHS or the Department of Health.
Disclaimer The views and opinions expressed by authors in this publication are those of the authors and do not reflect those of the UK NHS, NIHR, the UK Medical Research Council, Central Commissioning Facility, NIHR Evaluation, Trials and Studies Coordinating Centre, the Health Technology Assessment programme or the Department of Health.
Competing interests None declared.
Patient consent for publication Not required.
Ethics approval Research ethics committee approval for the study was granted by the National Research Ethics Service-Northern and Yorkshire Research Ethics Committee (09/H0903/31).
Provenance and peer review Not commissioned; externally peer reviewed.
Data availability statement Data are available on reasonable request from the authors.