Article Text

Statistics from Altmetric.com
Executive summary
This Framework has been developed by a multidisciplinary working group in the light of evidence of improving outcomes for babies born before 27 completed weeks of gestation, and evolving national and international changes in the approach to their care.
Management of labour, birth and the immediate neonatal period should reflect the wishes and values of the mother and her partner, informed and supported by consultation and in partnership with obstetric and neonatal professionals.
Whenever possible, extreme preterm birth should be managed in a maternity facility co-located with a designated neonatal intensive care unit.
Neonatal stabilisation may be considered for babies born from 22+0 weeks of gestation following assessment of risk and multiprofessional discussion with parents. It is not appropriate to attempt to resuscitate babies born before 22+0 weeks of gestation.
Decision-making for babies born before 27 weeks of gestation should not be based on gestational age alone, but on assessment of the baby’s prognosis taking into account multiple factors. Decisions should be made with input from obstetric and neonatal teams in the relevant referral centre if transfer is being contemplated.
Risk assessment should be performed with the aim of stratifying the risk of a poor outcome into three groups: extremely high risk, high risk and moderate risk.
For fetuses/babies at extremely high risk, palliative (comfort focused) care would be the usual management.
For fetuses/babies at high risk of poor outcome, the decision to provide either active (survival focused) management or palliative care should be based primarily on the wishes of the parents.
For fetuses/babies at moderate risk, active management should be planned.
If life-sustaining treatment for the baby is anticipated, pregnancy and delivery should be managed with the aim of optimising the baby’s condition at birth and subsequently.
Conversations with parents should be clearly documented and care taken to ensure that the agreed management plan is communicated between professionals and staff shifts.
Decisions and management should be regularly reviewed before and after birth in conjunction with the parents; plans may be reconsidered if the risk for the fetus/baby changes or if parental wishes change.
Introduction
Care of the baby, mother and family around the time of an extremely preterm birth is one of the most challenging aspects of perinatal medicine, both for clinicians and families. In 2006, the Nuffield Council on Bioethics convened a working group to explore the ethical, social, economic and legal issues around clinical decisions made in fetal and neonatal medicine1; in response to their report, the British Association of Perinatal Medicine (BAPM), in conjunction with other professional groups, developed a Framework for Clinical Practice for the management of babies born extremely preterm at less than 26 weeks of gestation. These documents were based largely on data from the original EPICure study in 1995 of births before 26 weeks of gestation, with some additional preliminary data from EPICure 2 regarding babies born in 2006 before 27 weeks of gestation.2 3 Subsequently, the Royal College of Obstetricians and Gynaecologists (RCOG) developed a scientific position paper about the management of delivery at the threshold of viability.4
The ethical principles that formed the basis for these earlier guidelines have not changed, but advances in perinatal care have led to steadily improving outcomes for babies admitted to UK neonatal intensive care units (NICUs), particularly at the lowest gestational ages. In the current era, the outcomes for babies actively managed at 22 weeks of gestation appear similar to those of babies at 23 weeks of gestation at the time of the 2008 BAPM Framework for Clinical Practice.5–8 Reports from other countries confirm increasing survival and improving neurodevelopmental outcome for babies born before 27 weeks of gestation.9–12 Although internationally there remain differences in practice, there is increasing willingness to consider stabilisation at birth and subsequent intensive care for the most extremely preterm babies,13–15 accompanied by greater acknowledgement of the importance of involving parents in perinatal decision-making.16 Reported outcomes are, of course, impacted by willingness to consider active interventions before and after birth.17
This updated Framework for Practice has been developed by consensus, taking into account the most recent available outcome data both from the UK and internationally, and follows wide consultation. BAPM is grateful for input from the RCOG, the British Maternal and Fetal Medicine Society, the Royal College of Paediatrics and Child Health (RCPCH), MBRRACE-UK, the Neonatal Nurses Association and parent representative organisations including Bliss and Sands. The scope has been extended to include births up to 26+6 weeks of gestation, better to align with national recommendations and published data, and we refer to new RCPCH and other national guidance on palliative care of babies as well as guidance on bereavement care for parents who experience loss of a baby.18 19
Prevention of preterm birth is now a national priority and all maternity services should ensure that measures are in place to realise this ambition. National guidance is available to enable prevention strategies; this guidance focuses on the importance of good communication between professionals and parents, strategies to ensure high-quality active and/or palliative care as appropriate and interventions to optimise outcomes for babies born too soon.4 20–22
Perinatal care at extremely preterm gestations will always need to be individualised and should be led by senior staff in midwifery, obstetrics and neonatology. Parents should be included in discussions about perinatal care, and their hopes and expectations explored with honesty and compassion in a realistic way. Decisions should be made together with parents, based on the best available evidence about the prognosis for the individual baby, and mindful of the need to act in the baby’s best interests. It is essential that such decisions reflect all relevant prognostic information and not simply gestational age.
REMIT
The purpose of this Framework for Practice is to assist decision-making prior to and/or at the time of birth relating to perinatal care and preterm delivery at 26 weeks and 6 days of gestation or less in the UK. It does not relate to decision-making around termination of pregnancy.
For some extremely preterm babies, postnatal events may indicate that continuation of neonatal intensive care is not in the baby’s best interests. While parents should be made aware of this possible outcome, this Framework does not address decisions around withdrawal or withholding of life-prolonging treatment after a baby has been admitted to a NICU.
The Framework for Practice is aimed primarily at professionals but is freely available via the BAPM website. We have included guidance designed to assist health professionals in communicating with parents about the issues and information contained within this document. It is emphasised that each case will be unique and that communication should always be tailored accordingly. We hope that the Framework will be incorporated into local and network guidelines, to ensure consistency of practice within units and networks and acknowledgement of the importance of individualised care for families.
Definitions
In the UK, a stillbirth is legally defined as the birth of a baby with no signs of life at, or after, 24 completed weeks of gestation.
For consistency, we have used the term ‘fetus’ to describe the baby before birth, and ‘baby’ after birth. Within the document, ‘parents’ refers to the mother and her partner.
We have used the terms ‘active care (survival focused)’ to refer to obstetric and neonatal management that has the aim of sustaining life for the baby, and‘palliative care (comfort focused)’ to refer to obstetric and neonatal management when the aim is not to attempt to sustain the life of the fetus/baby, but to focus on the baby’s comfort.
We acknowledge that these terms are imperfect: palliative care requires an active approach to the management of labour, delivery and the care of the baby, and active care may appropriately include no active interventions (eg, unassisted vaginal birth).
‘NICU’ refers to a designated neonatal intensive care unit, sometimes termed a level 3 unit.
Risk-based approach to decision-making
A key ethical consideration for decisions about instituting life-sustaining treatment for an extremely preterm baby is the baby’s prognosis—the risk of an acceptable (or unacceptable) outcome if active (survival focused) management is undertaken. If there is a plan to provide life-sustaining treatment for the baby, then it follows that the pregnancy and birth should be managed with the aim of optimising the baby’s condition at birth and subsequently.
We advise a stepwise approach to decision-making, involving three key stages:
Assessment of the risk for the baby if delivery occurs, incorporating both gestational age and factors affecting fetal and/or maternal health.
Counselling parents, and their involvement in decision-making.
Agreeing and communicating a management plan.
Assessment of the risk for the baby
Gestation-based risk assessment, including mortality and survival with severe impairment
The earlier the ultrasound dating scan has been carried out, the more accurately gestational age will be known. In accordance with NICE guidelines, all pregnant women in the UK should have been offered an early ultrasound scan between 10+0 and 13+6 weeks of gestation, with crown–rump length (CRL) measurement used to determine gestation. This assessment is accurate to within 5 days in 95% of cases.23 From 14+0 weeks (CRL >84 mm), gestation should be estimated from fetal head circumference; the estimated uncertainty of this gestation prediction is 6–7 days at 14 weeks, rising to 12–14 days by 26 weeks of gestation.24
Survival of extremely preterm infants has increased steadily since 2006 with greater willingness to offer neonatal intensive care. Recent UK data, for babies born in 2016, indicate survival to 1 year of 38% of those babies 23+0 to 23+6 weeks of gestation who received active treatment after birth8 (online supplementary appendix 1). Similar survival rates for admitted babies at 22 weeks of gestation are reported, but the number of surviving babies at 22 weeks of gestation is small, with appreciable in-labour mortality, and thus the CIs are wider than at later gestational ages. These figures accord with international data which show a trend towards increasing survival at 22 weeks of gestation, with reported survival rates of approximately one-third in babies who receive active care at birth. Since only a small proportion of babies born at 22 weeks of gestation receive active treatment, there is the possibility of selection bias and survivors may represent a subgroup of 22-week-gestation babies with more favourable risk factors (see below).
Supplemental material
At all gestational ages, survival rates show ongoing improvement,6 are higher when the number of live born babies rather than all births is used as a denominator and are highest when babies who receive palliative care at birth are excluded. As survival to live birth will be influenced by management of labour and birth, and the risk of mortality is 100% when a decision is made to offer palliative care, the most relevant denominator is those babies born alive and in whom active management has been attempted. Outcomes are continually changing and management should always be based on the most recent data available; online supplementary appendix 1 presents the most up-to-date data available in September 2019.
Assessment of the risk of severely disabling conditions among survivors is fraught with difficulty, not least differences in individual views about acceptable levels of disability. What for one individual or family may be an acceptable outcome may not be acceptable for another. For decisions about provision of potentially life-sustaining treatment, the ethically relevant consideration is the risk of disabilities that could affect whether it is in the baby’s best interests to survive and thus risk assessment should focus on the most severe disabilities.25
In the absence of regularly updated national data on the prevalence of severe disability after extremely preterm birth, we recommend that the well-established “severe impairment” category, as defined by the 2008 BAPM Working Group, be used to inform parents when discussing risk following extremely preterm birth.26 It is acknowledged that many more extremely preterm babies will be affected by milder degrees of disability; this should also be included in information provided to parents, with clear explanation that disability is generally impossible to predict for individual babies at birth.
The severe impairment category includes any of:
Severe cognitive impairment with an IQ lower than 55 (<−3 SD); this will usually result in the need for special educational support and require supervision in daily activities.
Severe cerebral palsy—classified as Gross Motor Function Classification System grade 3 or greater (online supplementary appendix 1).
Blindness or profound hearing impairment.
The risk of severe impairment increases with increasingly preterm birth and is currently approximately one in seven at 24 weeks of gestation, and 25% at 23 weeks of gestation for those babies who receive active care and survive. The number of surviving babies with long-term outcome information at 22 weeks of gestation is relatively small, and therefore CIs apply, but the risk of severe impairment is estimated to be one in three. Generally, as the risk of mortality decreases, the risk of disability among survivors also decreases (online supplementary appendix 1, figure 1).
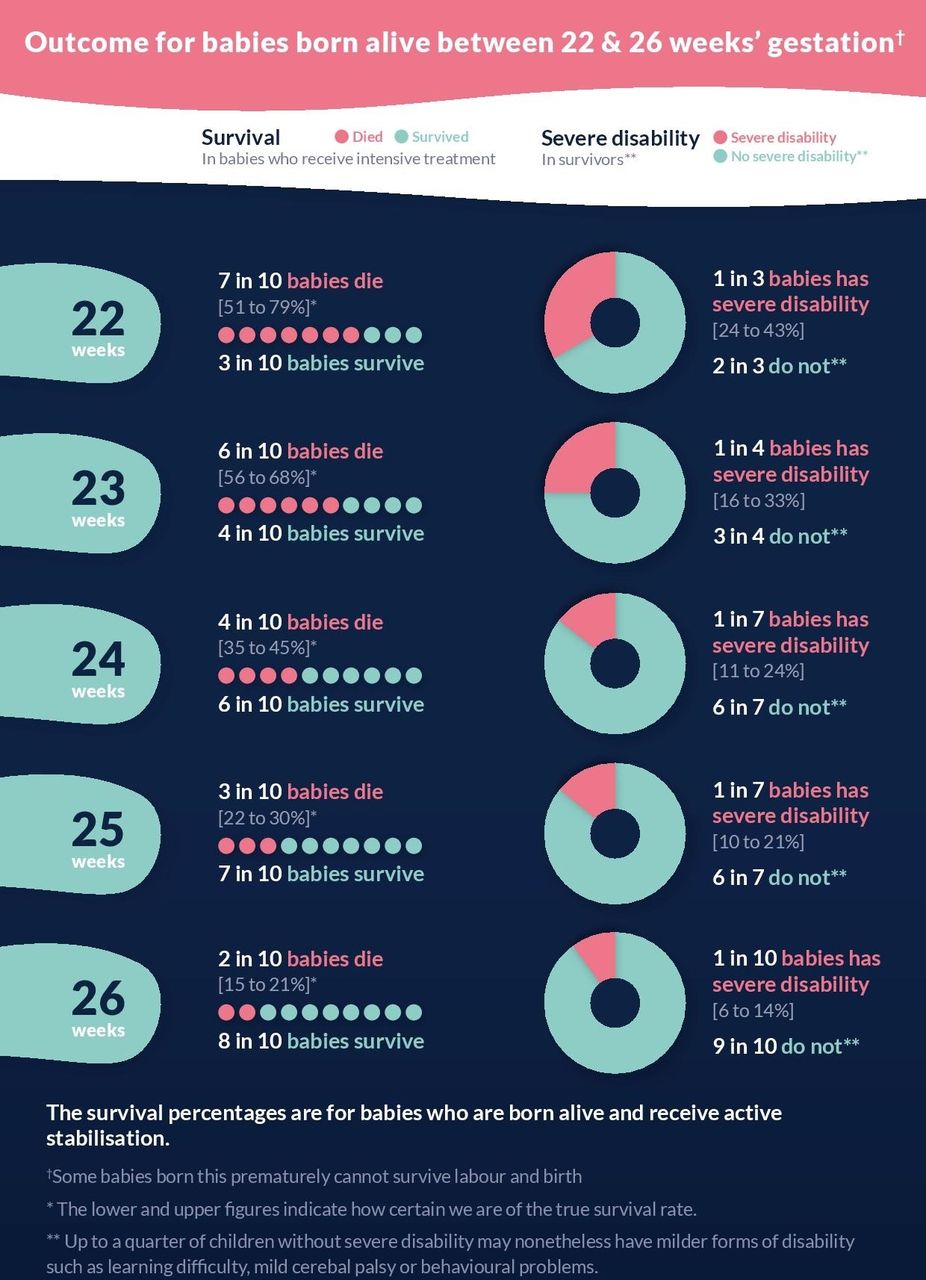
Infographic for parents on the outcomes of extreme preterm birth.
Modified risk assessment
Accurate information about the current pregnancy, including assessment of both fetal and maternal health should be used to refine gestation-based risk of absolute survival and survival without severe impairment.
A range of factors are associated with increased or decreased risk:
Fetal factors
Fetal factors which may increase risk include male sex, multiple pregnancy, congenital anomaly and poor fetal growth.
Clinical conditions
Clinical conditions which pose additional risk and have been associated with increased mortality and morbidity include prolonged pre-labour rupture of membranes before 24 weeks of gestation and clinical evidence of chorioamnionitis.27 28
Therapeutic strategies
Administration of antenatal steroid and magnesium sulfate are associated with improved survival and neonatal outcomes as well as reduced risk of childhood impairment, even before 24 weeks of gestation.29–32
Clinical setting
Survival is highest at these extreme preterm gestations in centres with experienced staff and higher patient numbers. A strategy of antenatal transfer below 27 weeks of gestation for birth in a maternity unit with a co-located NICU is recommended.4 33–37
Following full history taking and risk assessment, the risk of unacceptably poor outcome if life-sustaining care is provided for the baby will generally fall into one of the following categories: extremely high risk; high risk; moderate risk. A proposed visual tool for refinement of risk is illustrated in figure 2. See also online supplementary appendix 5 for case examples applying the risk categories.

Visual tool for refinement of risk. NICU, neonatal intensive care unit.
Box 1 represents the consensus of the Working Group in regard to risk categories for the purposes of this Framework.
Risk categories
Extremely high risk: The Working Group considered that babies with a >90% chance of either dying or surviving with severe impairment if active care is instigated would fit into this category. For example, this would include:
Babies at 22+0 to 22+6 weeks of gestation with unfavourable risk factors.
Some babies at 23+0 to 23+6 weeks of gestation with unfavourable risk factors, including severe fetal growth restriction.
(Rarely) babies ≥24+0 weeks of gestation with significant unfavourable risk factors, including severe fetal growth restriction.
High risk: The Working Group considered that babies with a 50–90% chance of either dying or surviving with severe impairment if active care is instituted would fit into this category. For example, this would include
Babies at 22+0 to 23+6 weeks of gestation with favourable risk factors.
Some babies ≥24+0 weeks of gestation with unfavourable risk factors and/or comorbidities.
Moderate risk: The Working Group considered that babies with a <50% chance of either dying or surviving with severe impairment if active care is instituted would fit into this category. For example, this would include
Most babies ≥24+0 weeks of gestation.
Some babies at 23+0 to 23+6 weeks of gestation with favourable risk factors.
There is no objective way of defining a risk as ‘extremely high’ versus ‘high’ and families differ in the outcome that they regard as unacceptably poor. Thus, risk assessment may need to be modified in the light of the parents’ knowledge, views and values. It is important that parents are offered choices and supported to make decisions appropriate for their individual preferences.
For women presenting to a non-tertiary maternity and neonatal centre, assessment of risk should include early discussion with the relevant referral centre. For pregnancies from 22+0 weeks of gestation, decisions should not be based on gestational age alone. Within a multiple pregnancy, the risk may differ between fetuses and so each should be considered as an individual. This means that appropriate management may not be the same for each baby, even with the same gestational age. If birth occurs prior to 22+0 weeks of gestation, active obstetric and neonatal management is not appropriate. Situations of uncertainty (eg, uncertain gestation) or disagreement are discussed in online supplementary appendix 2.
The agreed risk for the baby has ethical and practical implications for the options that should be available.
Extremely high risk
For babies with an extremely high risk of death or of survival with unacceptably severe impairment despite treatment, palliative (comfort-focused) care would be in the best interests of the baby and life-sustaining treatment should not be offered. There is no absolute indication for paediatric attendance at the birth although for individual families this may be helpful.
High risk
For babies with a >50% risk of death or of surviving with unacceptably severe impairment despite treatment, it is uncertain whether active (survival focused) management is in the best interests of the baby and their family. Parents should be counselled carefully and parental wishes should inform a joint decision to provide either active or palliative treatment. Ideally, a senior neonatal clinician who has previously met the parents will be available to attend the birth and supervise implementation of the agreed plan.
Moderate risk
For babies with a <50% risk of death or of survival with unacceptably severe impairment, active management would be in the best interests of the baby. A senior neonatal clinician should attend the birth.
Counselling parents and decision-making
Whenever possible, parents should be involved in planning an extremely preterm birth. The planning consultation should include senior clinical staff from the obstetric, midwifery and neonatal teams who will be caring for the mother and her baby before, during and after the birth.
The assessed category of risk to the baby (including the inherent uncertainty around this) should be conveyed sympathetically and with clarity, and the hopes and expectations of parents explored with honesty and compassion in a realistic way. Clear, balanced information should be shared (figure 1) and management options discussed. Time should be allowed for clarification and questions, and parents offered the opportunity to revisit discussions with the perinatal team at any point, acknowledging the challenging nature of the information that they are being asked to receive and the decisions that are being made. See online supplementary appendix 3 for guidance on communication and consultation with families. Online supplementary appendix 4 provides some sample written material to complement consultations.
In utero transfer to a maternity facility co-located with a NICU should be considered at the earliest opportunity when active management is planned. All such transfers should be discussed with the receiving team, and parents should be made aware that the prognosis (and therefore management) may be revised following in utero transfer to a centre with greater experience of managing extremely preterm birth (eg, following detailed ultrasound scanning). Communication and agreed plans should be documented in full (including in the maternity handheld record) and, when relevant, clearly communicated with the receiving centre. The agreed plan of management should be revised regularly if pregnancy continues. Parents should also be helped to appreciate that the baby may be born in unexpectedly poor, or unexpectedly good condition, and the implications of this for what care might be appropriate. Processes should be in place to ensure timely transfer.
When active care is planned and time allows, parents should be given an opportunity to visit the neonatal unit and to meet staff and should receive information and support regarding expressing breast milk.
Where appropriate, the practicalities of commencing, withholding and/or withdrawing intensive care and the positive role of palliative care strategies should be described to the parents. This will help prepare them for possible outcomes after the birth. Parents may find the advice and support of their family, friends, spiritual advisers and/or local and national support organisations to be of great value at this time and should be signposted appropriately.
Agreeing a management plan
Following consultation with parents, initial management of the birth will follow one of two pathways: ‘active’ (survival focused) or ‘palliative’ (comfort focused) (figure 3). Consistency in obstetric and neonatal management is essential, either to ensure that the baby is born in the best possible condition or to avoid unnecessary intervention. The agreed plan should be clearly documented and communicated to all members of the obstetric and neonatal teams who may be involved in care of the family.

{kind=link}
{kind=link}
{kind=link}
Decision-making around management of delivery, following risk assessment and after consultation with parents.
The challenges inherent in making a binary decision from a continuum of risk should not be underestimated and categorisation of risk should always be undertaken by the most senior clinicians available. Electronic risk calculators may be of value, but care should be taken to ensure they are populated with the most recent data and include the most relevant denominator.
Parents should be counselled that the plan for management will be reviewed and may need to change based on the clinical condition of the baby before, at or after birth, or subsequently in a NICU.
Obstetric management
Active (survival focused) obstetric management
When it has been agreed that potentially life-sustaining care for the baby is appropriate, active obstetric management is important to ensure the baby is born in the best possible condition. An individualised package of obstetric intervention should be offered in all cases where a commitment to active neonatal care is in place.4 35 The potential for each component intervention to optimise the condition of the individual baby at birth should be considered and not excluded on the basis of gestational age alone. Obstetric management should be regularly reviewed, particularly if events suggest changing prognosis for the baby.
The package of obstetric care to be offered to parents may (but not necessarily) include any or all of the following:
Antenatal steroids.
Tocolysis.
Antenatal transfer to a tertiary obstetric centre co-located with a NICU.
Magnesium sulfate for neuroprotection.
Deferred cord clamping, ideally for 60 s or more.
Intrapartum fetal heart rate monitoring.
Caesarean section (if potential benefits are considered to outweigh risks)
Antenatal steroids, tocolytic use, magnesium sulfate and deferred cord clamping38 have been shown to be of benefit in improving outcome in preterm infants. However, parents should be made aware that there is a paucity of data in relation to the magnitude of benefit and risks of these interventions, particularly below 24 weeks of gestation.
In utero transfer to a tertiary centre optimises outcomes for the baby, is better than ex utero transfer and is now a prioritised NHS England recommendation as well being recommended in the Scottish Maternity and Neonatal Services Review.21 36 37 While the majority of women presenting in threatened preterm labour before 27 weeks of gestation do not deliver in the subsequent 24 hours, there is currently no proven test which accurately predicts preterm delivery. Transfer may present challenges for the family as well as obstetric and ambulance services, but the Working Group strongly recommends that this is considered at the earliest opportunity. A decision for antenatal transfer should include documented discussion with the relevant tertiary centre and careful risk assessment by a senior obstetrician, to ensure that the mother is fit for transfer and to reduce the risk of birth in transit. Both written and verbal information should be given to parents. In some cases, poor maternal health and/or advanced stage of labour may mean that in utero transfer is not the safest option.
Below 26 weeks of gestation, a senior obstetrician should be involved in decisions around intrapartum fetal heart rate monitoring as there is a lack of evidence to inform practice.20 The family should be made aware of the rationale for either recommending or withholding fetal heart rate monitoring; for example, it may be appropriate not to monitor the fetal heart if delivery by caesarean section is not part of the agreed package of care, either because it is considered that the risks of caesarean section outweigh any potential benefits or because parents have declined caesarean section should there be a fetal heart rate abnormality. Autonomic immaturity at gestations below 26 weeks makes interpretation of continuous electronic fetal heart rate monitoring (CEFM) difficult and there is no evidence that CEFM improves outcomes compared with intermittent auscultation. From 26+0 weeks of gestation, when active management is planned, women in established preterm labour should be recommended CEFM.4 20
In the majority of extremely preterm births, the mother presents in spontaneous labour and an uncomplicated vaginal delivery may be anticipated. The risk of head entrapment following breech presentation is approximately 10%,4 but the evidence for delivery by caesarean section for extremely preterm babies is limited and of poor quality39 40 and prognosis is more likely to be dictated by factors other than mode of delivery. NICE guidance is that delivery by caesarean section may be considered in cases of breech presentation after 26 weeks of gestation.20 Extremely preterm caesarean sections can be difficult, and fetal trauma including head entrapment can still occur.4 Maternal risks and consequences including pain, haemorrhage, infection, thrombosis and injury to bowel and bladder are higher after caesarean section compared with vaginal birth, particularly at extremely preterm gestations, and should be discussed with the mother. There is an impact on future pregnancies in terms of increased risk of uterine rupture and morbidly adherent placenta, and the likelihood of classical caesarean section, with its increased risk of serious maternal complications, is greatest at the most preterm gestations.40 41 For all these reasons, it is essential that obstetric care is individualised after full discussion between the family and a senior obstetrician along with the neonatal team. There should be clear documentation of this conversation and the mother’s wishes.42 Where delivery by caesarean section has been agreed as the optimal mode of birth, this should only occur once labour is established, unless maternal or fetal condition dictates otherwise. Established preterm labour can be difficult to determine and even at advanced cervical dilation birth may not occur for several days. There may be additional benefit to the baby of delaying delivery.
In the absence of labour and where delivery should be expedited for maternal reasons (eg, pre-eclampsia or chorioamnionitis) or, more rarely, for fetal reasons (eg, severe fetal growth restriction) delivery by caesarean section may be the only option to ensure timely delivery for mother and/or baby. Induction of labour is unlikely to be appropriate in such circumstances where there is maternal or fetal compromise and a commitment to potentially life-sustaining care for the baby has been agreed with the parents.
Palliative (comfort focused) obstetric management
When a decision is made for palliative (comfort focused) management of the baby at birth, only interventions for maternal benefit are appropriate. Intrapartum fetal heart rate monitoring is not advised, although assessing or listening for the presence of a fetal heart to check viability may be helpful in clarifying expectations around the baby’s condition at birth and be preferable for parents. Parents should be made aware that their baby may show signs of life after birth, including visible heartbeat, gasping and/or movement of limbs.
Neonatal management
Active (survival focused) neonatal management
Stabilisation and support for transition should be carried out by, or under the direct supervision of, the most senior member of the neonatal/paediatric team available at the time of birth, and in accordance with Resuscitation Council UK guidance, noting specific recommendations for preterm infants.43 Ideally, this team will be experienced in stabilisation of extremely preterm babies and led by a consultant neonatologist. The team should be aware of parental wishes, but when the baby is born in unexpectedly poor, or unexpectedly good condition, it is reasonable for the attending neonatologist to proceed with care in the baby’s best interests (see online supplementary appendix 2).
Deferred cord clamping for at least 60 s should be routine practice (unless contraindicated), and particular attention should be paid to the maintenance of normothermia, with the use of a plastic bag and/or other methods of delivering thermal care, and skin protection. Stabilisation and supported transition with lung inflation, using an appropriately sized facemask, should be initiated. Care should be taken not to over-distend the lungs.
Clinical assessment in the delivery room is not a good predictor of survival in extremely preterm babies44; if there is no response to mask ventilation, and any doubt around the adequacy of ventilation, the baby should be intubated and surfactant administered. The most important intervention is establishment of adequate lung recruitment, and the most important measure of success is heart rate. Use of advanced measures for resuscitation including cardiac massage and endotracheal or intravenous epinephrine are rarely required following extreme preterm birth. In the absence of sufficient evidence to justify a different approach in extremely preterm babies, if advanced resuscitation is considered appropriate, the Working Group recommends applying newborn resuscitation algorithms as used in more mature babies.
Where babies are born in much poorer condition than expected, it may be appropriate to reconsider the planned provision of active management and to move to palliative care (see online supplementary appendix 2). Absent heart rate or severe bradycardia persisting despite effective cardiopulmonary resuscitation for more than a few minutes is associated with high rates of mortality and neurodevelopmental impairment in extremely preterm babies.45 46 The most senior experienced attending professional should decide if or when attempts to stabilise and/or resuscitate the baby should stop.47
Stabilisation should normally be undertaken in the same room as the parents, who should be offered the opportunity to see, touch and photograph their baby. Following successful stabilisation of the baby, the mother should be supported to express breast milk as early as possible, with ongoing facilitation of parental contact and family involvement as partners in care.
Palliative (comfort focused) neonatal management
Where there is an extremely high risk of a poor outcome for the baby, it would be considered in the best interests of the baby, and standard practice, not to offer active neonatal management.
The aim of palliative neonatal management is to support the parents and their baby and to avoid interventions that may cause discomfort, pain or separation of the baby from the parents. This care should be delivered in the most appropriate location for the family (which is not necessarily a neonatal unit) and should not necessitate in utero transfer. There should be an emphasis on family-centred care, with opportunities for parents to create positive memories of their baby. An Individualised Care Plan should be made in partnership with parents following guidance within the Perinatal Palliative Care Pathway from Together for Short Lives.18 Further recommendations may be found in a RCPCH monograph on making decisions to limit treatment in life-limiting and life-threatening conditions.19
Depending on parents’ wishes and service provision, a senior neonatologist or paediatrician may be present at delivery to provide a brief assessment of the baby’s condition at birth and to support midwifery staff and the family. Respiratory support (including provision of positive pressure ventilation) should not be provided. Parents should be offered the opportunity to hold and to spend as much time as they wish with their baby in a quiet and private location; they should have been counselled that the baby may show brief reflex movements or signs of life after birth. In the unlikely scenario of the baby being born in much better condition than expected, palliative management may need to be reconsidered (see online supplementary appendix 2 for further discussion).
On average, babies born before 24 weeks of gestation who receive comfort care in the delivery room live for approximately 60 min (range from a few minutes to several hours).48 Supplemental oxygen is not necessary but could be provided if parents desire.
After the baby has died, a parent-led bereavement care plan should be put in place for the family, including communicating with parents and creating memories. Parents should understand what to expect in terms of a review into the care provided during pregnancy and birth using the Perinatal Mortality Review Tool, and the benefits of investigations such as autopsy and placental histopathology, to provide as much explanation as possible for the preterm birth and the death of their baby.18 In England and Scotland, this should follow the guidance outlined in the National Bereavement Care Pathway49; in Wales and Northern Ireland, there are locally developed bereavement pathways. Parents should be facilitated to make informed choices and signposted to support available after they go home. Follow-up pathways for all women who have undergone an extremely preterm birth should be in place and include planning care for future pregnancies. Placental histology, undertaken by a perinatal pathologist, should be routine.
After discharge home, optimal communication with all professionals involved (and in particular the general practitioner, health visitor and community midwife) is essential. The mother will continue to require postnatal care and should also receive information and advice about milk suppression or donation. Parents should be offered bereavement counselling and the opportunity to meet with perinatal staff for a follow-up consultation in an outpatient setting. Where possible, this meeting should be conducted by the same staff that counselled the family in the peripartum period. Parents should also be offered the opportunity to participate in a multiprofessional perinatal mortality review process that follows the framework set out in published statutory and operational guidance.49 At an appropriate time, the prognosis for future pregnancies should also be discussed.
Implementation of this Framework for Practice
A lead person should be identified in each maternity facility with responsibility for implementation, education, and dissemination of this new Framework for Practice and the accompanying parent information.
Links to relevant national documents are provided within this document; these should be highlighted and made easily available within each maternity facility.
Management of extreme preterm birth and the conversations around this can be exceptionally challenging for staff, so it is recommended that implementation of this Framework into individual units is accompanied by education and training in specific consultation skills.
Networks need to ensure sufficient resource to cope with the predicted number of extreme preterm deliveries, both actual and threatened, and pathways should be in place to ensure appropriate prioritisation and assessment of women likely to deliver extremely preterm. A newly delivered mother should be accommodated in a maternity facility adjacent to her baby.
References
Supplementary materials
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Footnotes
Twitter @HMactier, @SarahBates18, @carolinemdavey, @NeonatalEthics
Collaborators British Association of Perinatal Medicine Working Group: Erica Everett, Tara Selman. British Association of Perinatal Medicine in conjunction with the Royal College of Obstetricians and Gynaecologists, the Royal College of Paediatrics and Child Health, the British Maternal and Fetal Medicine Society, MBRRACE-UK, Bliss and Sands.
Contributors All of the authors attended at least one Working Group meeting and contributed to the writing and editing of the Framework for Practice. HM: chaired the Working Group and wrote the first and all subsequent drafts of the article. Approved the final version. SEB: contributed significantly to the drafting of the article and appendices and subsequent edits, and approved the final manuscript. TJ: contributed to the drafting of the article and subsequent edits, and approved the final manuscript. CL-D: contributed to the drafting of the article and appendices and approved the final manuscript. NM: contributed significantly to the drafting of the article and appendices and subsequent edits, compiled the figures and approved the final manuscript. KM: contributed to the drafting of the article and appendices and subsequent edits, and approved the final manuscript. LKS: contributed to the drafting of the article and appendices and subsequent edits, compiled the tables and approved the final manuscript. MT: contributed to the drafting of the article and subsequent edits, and approved the final manuscript. DW: contributed significantly to the drafting of the article and appendices and subsequent edits, compiled the figures and approved the final manuscript.
Funding BAPM supported preparation of this document by funding travelling expenses for Working Group members.
Competing interests None declared.
Patient consent for publication Not required.
Provenance and peer review Not commissioned; internally peer reviewed.