Article Text

Abstract
Non-invasive ventilation and especially the application of continuous positive airway pressure (CPAP) has become standard for the treatment of premature infants with respiratory problems. However, CPAP failure may occur due to respiratory distress syndrome, that is, surfactant deficiency. Less invasive surfactant administration (LISA) aims to provide an adequate dose of surfactant while the infant is breathing spontaneously, thus avoiding positive pressure ventilation support. Using a thin catheter for surfactant application allows infants to maintain function of the glottis and continue spontaneous breathing, whereas the INtubate-SURfactant-Extubate (INSURE) procedure is connected with sedation/analgesia, regular intubation and a (brief) period of positive pressure ventilation. Individual studies and meta-analyses summarised in this review point in the direction that LISA is more effective than standard treatment or INSURE both in terms of short-term (avoidance of mechanical ventilation) and long-term (intracerebral haemorrhage and bronchopulmonary dysplasia) outcomes. Open questions include exact treatment thresholds for different gestational ages, the usefulness of devices/catheters that have recently been purpose-built for the LISA technique and especially the question of analgesia/sedation during the procedure. The current technology still demands laryngoscopy with all its unpleasant effects for infants. Therefore, studies with pharyngeal surfactant deposition immediately after delivery, the use of laryngeal airways for surfactant administration and attempts to nebulise surfactant are under way. Finally, LISA is not simply an isolated technical procedure for surfactant delivery but rather part of a comprehensive non-invasive approach supporting the concept of a gentle transition to the extrauterine world enabling preterm infants to benefit from the advantages of spontaneous breathing.
- clinical procedures
- neonatology
- less invasive surfactant
- CPAP
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
History of LISA
Lack of surfactant was described as the cause of respiratory distress syndrome (RDS) in preterm infants 60 years ago. In the last 30 years surfactant replacement with exogenous surfactant preparations derived from animal sources became the most effective evidence-based therapy for RDS. The mode of administration has evolved especially in the last decade from endotracheal surfactant bolus administration during mechanical ventilation over Intubate-SURfactant-Extubate (INSURE) followed by continuous positive airway pressure (CPAP) towards less invasive techniques (less invasive surfactant administration (LISA)) that aim to effectively provide an adequate dose of surfactant while the infant is breathing spontaneously.1
As early as the 1980s, the introduction of CPAP, with the possibility to apply positive end-expiratory pressure (PEEP) via the nasal route with prongs, was avidly taken up in Scandinavia as an integral part of their minimal handling approach.2 However, CPAP failure, that is, increasing respiratory distress and oxygen demand due to evolving RDS, was common in very immature infants on non-invasive ventilation, prompting the search for methods to combine surfactant instillation with continued spontaneous breathing during CPAP support. Swede Lars Victorin was the first to treat infants with short-time intubation and surfactant instillation in Kuwait, where no neonatal ventilators were available in the 1980s. Following endotracheal intubation, surfactant was instilled intratracheally followed by bag ventilation and extubation after a variable interval. Danish neonatologist Henrik Verder was the first to use a small-diameter gastric tube to instil surfactant during spontaneous breathing in 1992, the obvious advantage of this method being that unlike an endotracheal tube no neonatologist would be tempted to leave a thin catheter longer than needed in the trachea (for review on the history of LISA, see ref 3).
However, at that time it was felt that distending positive pressure via bag ventilation was of prime importance for the spread of surfactant, so that the INSURE procedure was promoted, especially in Scandinavia, also by Verder and colleagues.3 However, INSURE needs analgesia/sedation and there is at least a (short/variable) period of positive pressure ventilation. The ‘small diameter tube method’ was forgotten until it was rediscovered, about 10 years after its initial description, by Angela Kribs in Cologne.4 Since 2003 the method has also been used in Lübeck. The founding of the German Neonatal Network (GNN) provided a solid platform for the pivotal randomised trials (Avoid Mechanical Ventilation and Non-Intubated Surfactant Application trials5 6) and additional observational studies on LISA,7 8 resulting in a cohort of currently more than 5000 well-characterised infants that were treated with LISA.
For some years, the method was exclusively used in Germany, until countries such as Austria, Australia, Turkey, Spain, Iran and China also began to publish studies on this topic.3 9 LISA is now an acknowledged alternative to the standard mode of surfactant delivery in a variety of national guidelines for surfactant treatment.10 In Germany, the majority of surfactant treatments are now performed by LISA (see figure 1).

Mode of surfactant administration in the German Neonatal Network. Inclusion limited to infants ≤30 weeks of gestation. LISA, n=4419; tube surfactant, n=5295; no surfactant, n=3514. LISA, less invasive surfactant administration.
How to perform LISA
In Germany, mainly thin and soft catheters (eg, gastric tubes, suction catheters, umbilical arterial catheters) are used for LISA and are mostly introduced into the larynx with the help of a Magill forceps. Routine oral intubation is more common in other parts of the world, so that the use of a stiff vascular catheter was described by Peter Dargaville et al 11 as the so-called Hobart method (minimally invasive surfactant therapy (MIST)) in 2011. Straight (LISAcath)12 or stiff catheters with an angulated tip (Surfcath) have been designed especially for the purpose of LISA via the oral route. Special introducers13 (Neocath) and devices to guide the catheter when video laryngoscopy is being used have recently been developed.
Effects of LISA
LISA is different from other modes of surfactant delivery as it allows the infant to keep on breathing and to use the physiological function of the larynx without (nearly complete) obstruction by a larger diameter endotracheal tube. Such small tubes (eg, 5 French, external diameter 1.66 mm) allow adduction of the vocal cords (see below for link to video). Following LISA, surfactant spreads quickly, making use of its unique biophysical properties without the need for positive pressure ventilation.
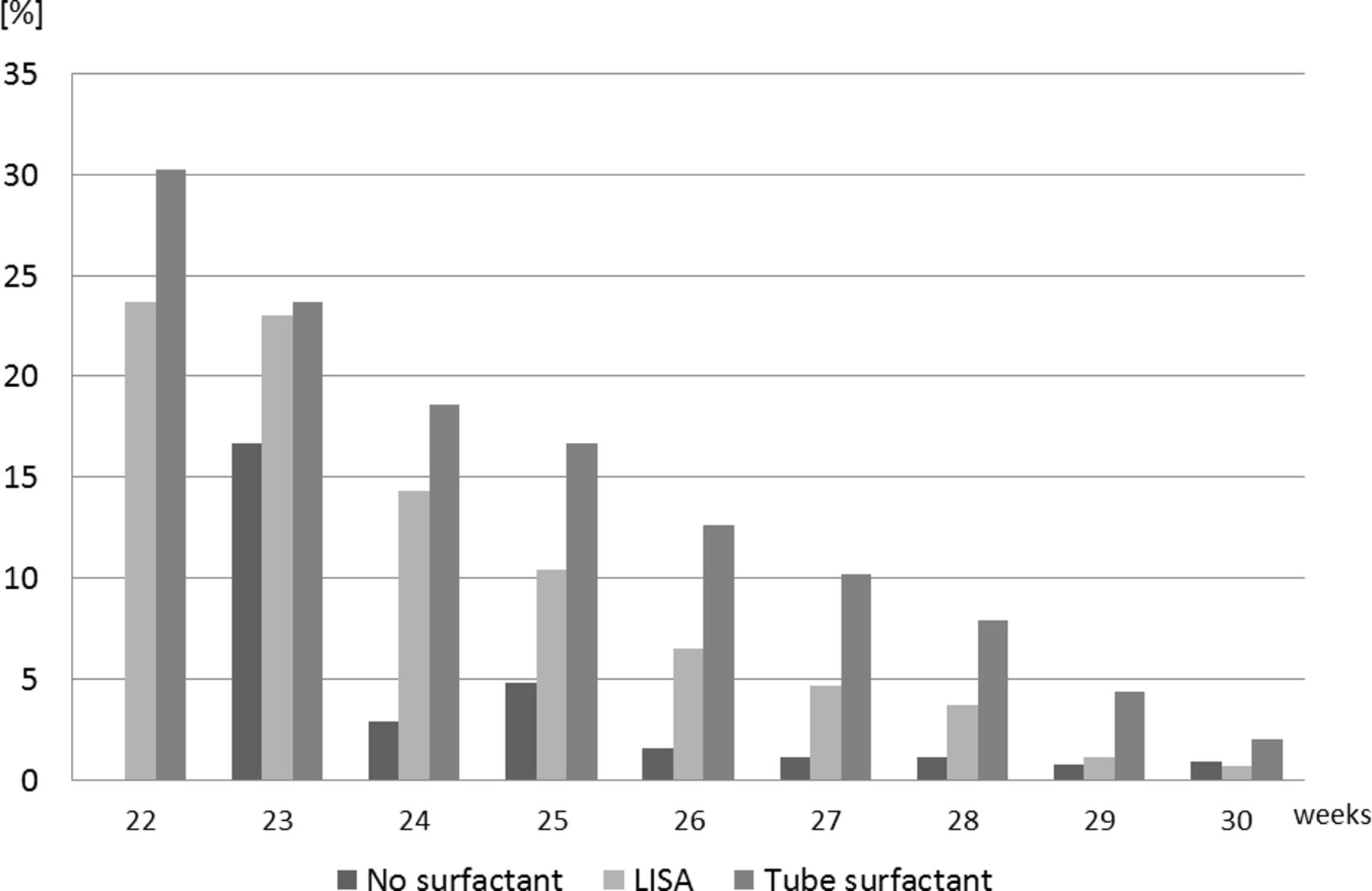
LISA has been shown to reduce the need for mechanical ventilation in randomised controlled trials (RCTs).5 6 An observational study using a matched-pairs design in more than 1000 infants demonstrated that this effect is robust in clinical practice also outside the specific setting of trials.7 Use of LISA in infants with a gestational age (GA) of 26–28 weeks avoids mechanical ventilation in the first 72 hours, which also means that the majority of infants will not need endotracheal intubation and ventilation throughout their hospital stay. In smaller infants with a GA of 25 weeks or less, the rate of mechanical ventilation is also reduced in the first 72 hours, but quite a few of these infants still need intubation later on mainly for severe apnoea.6 Figure 2 demonstrates that the effectiveness of LISA in preventing mechanical ventilation in the first 72 hours strongly depends on GA. The rate of bronchopulmonary dysplasia (BPD) in infants that have received surfactant by the LISA technique is low compared with international standards (figure 3).

Mechanical ventilation within the first 72 hours of life in LISA-treated infants, n=4419. LISA, less invasive surfactant administration.
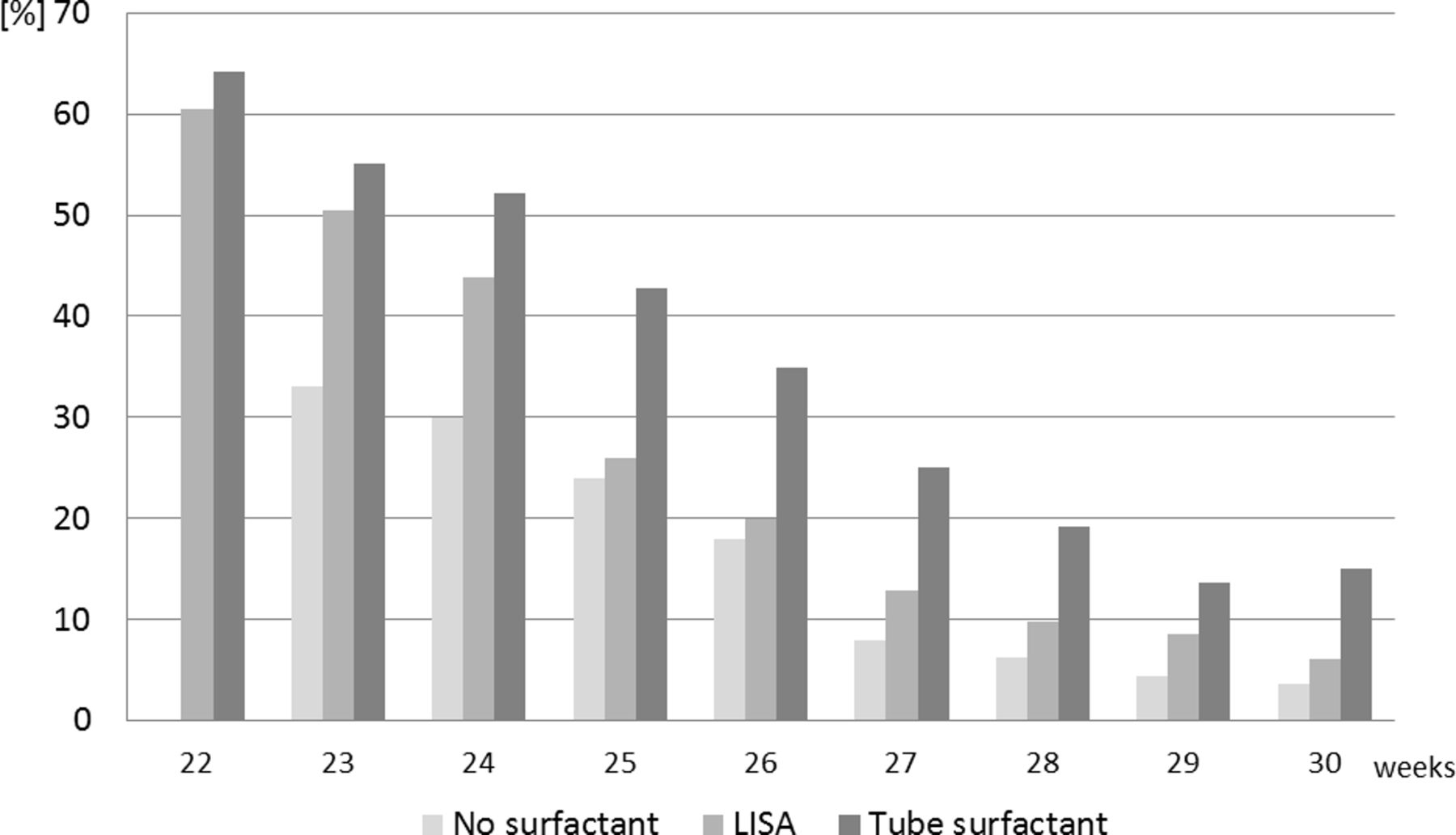
Bronchopulmonary dysplasia at 36 weeks stratified for gestational age and mode of surfactant treatment. LISA, less invasive surfactant administration.
The data derived from the GNN reflect clinical practice in >50 German neonatal intensive care units (NICUs), and the effects observed are very similar to the findings from randomised trials. This is reassuring as it seems that similar effects of LISA can be obtained in the well-controlled settings of clinical trials and under ‘real life’ clinical situation. However, such data can clearly not replace data from RCTs as there may be selection bias; for example, the group of infants that receive surfactant by endotracheal tube may also include some infants that were intubated, for example, due to asphyxia directly in the delivery room. However, due to the large number of included infants treated with the LISA technique, such confounders show relatively little distorting effects. A matched-pair analysis including, for example, Apgar and disease severity came to very similar results in terms of avoidance of mechanical ventilation and complication rate.7
The network data (figure 4) on intraventricular haemorrhage (IVH) also confirm the findings from the NINSAPP study6 with a reduced incidence of complications. This indicates that postnatal adaptation under spontaneous breathing, even if for only a few days, may have lifelong benefits.6 7
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Intraventricular haemorrhage (grade III–IV) stratified for gestational age and mode of surfactant treatment. LISA, less invasive surfactant administration.
Meta-analyses9 14 15 point out that LISA is superior to CPAP alone or the INSURE technique both in terms of avoidance of BPD and IVH.9 However, the quality of some of the studies included in these meta-analyses was questionable, so that further confirmative randomised controlled studies are needed.9
LISA and GA
LISA can be successfully applied in infants as immature as 22 weeks, but obviously special experience is needed in this age group. In the most immature infants, many centres use LISA already in the delivery room as soon as oxygen demand or respiratory distress becomes evident. However, such a ‘quasi prophylactic’ approach has not yet been evaluated in RCTs. In the more mature preemies, often a threshold fractional inspired oxygen (FiO2) of 0.30 is used as an indication for LISA. With FiO2 >0.60 severe RDS has to be assumed and the risk for LISA failure seems higher.
In infants above 32 weeks there is no evidence for a benefit of LISA. In our experience these relatively mature infants often need sedation/analgesia to tolerate the procedure, which interferes with the spontaneous breathing that is needed to make the method work. In addition, the risk of chronic lung disease is low in this group of infants.16
LISA does not exclude analgesia and/or sedation
In infants <26 weeks most centres in Germany will do the first LISA attempt without analgesia.5 Non-pharmacological methods of analgesia such as positioning, holding (‘facilitated tucking’) and/or sucrose solutions are used in most centres. A variety of drugs have been studied for the purpose of analgesia/sedation during INSURE or LISA; fentanyl, ketamine and propofol were the most frequently used medications. First studies indicate that these drugs may help to reduce pain scores, but may interfere with spontaneous breathing.17 With fentanyl, chest rigidity and interference with spontaneous breathing have also been reported. Stress and pain in the neonatal period may have long-term negative effects and should clearly be avoided whenever possible, but drugs used for stress/pain relief also have acute and long-term side effects. Thus, practice patterns of using these drugs vary widely.18
Timing, dosage and type of surfactant
There is a trend to use LISA early, that is, at 20–30 min of life after successful adaptation after birth. Clearly, randomised trials are needed to evaluate the effects of such ‘quasi prophylactic’ versus later ‘rescue’ LISA treatment.
Animal-derived surfactants obtained by lung lavage or from tissue homogenates of bovine or porcine origin have been used in different studies. These studies were too small for valid comparisons between different surfactant preparations in terms of LISA effectiveness. The AMV trial5 used a dose of 100 mg/kg, while the NINSAPP trial6 a whole vial of 120 mg porcine surfactant per infant. In daily routine, a whole vial policy often resulting in doses of ≥150 mg/kg (eg, in an 800 g baby) has been widely adopted hoping that this higher surfactant dose may give ‘some reserve surfactant pool’ and reduce the need for retreatment. In addition, when LISA is done in the delivery suite, the exact birth weight is often estimated, which makes the whole vial approach also practical from this perspective.
LISA is not an isolated technical procedure
LISA is not only a single technical procedure but rather a component of a complex care bundle supporting the individual capacity of a newborn premature baby to adapt to extrauterine life. Prenatal lung maturation with antenatal steroids and the right timing to deliver a baby in good condition enabling spontaneous breathing and efficient CPAP therapy are crucial for LISA success. It seems wise to allow time for postnatal adaptation, avoid hypothermia, avoid unnecessary manipulations (eg, suctioning without indication), delay cord clamping and use a minimal handling approach (‘soft landing’) whenever possible. Most German centres with LISA experience use intravenous caffeine straight after birth in the delivery room to promote spontaneous breathing, although there is no clear evidence from RCTs supporting this approach.
Centre effects are observed in the GNN. This suggests that the LISA procedure itself and the handling of the infants in the first hours of life are decisive for maintaining spontaneous breathing. Most centres used CPAP at 6–9 cm H2O after birth with a variety of different devices. The use of high flow nasal cannula later on in the NICU is increasing in popularity, but usage in the delivery suite is uncommon in Germany as CPAP seems to allow higher distending pressures.
In the most immature infants LISA may only delay intubation and mechanical ventilation for some days. Most of the babies <26 weeks are intubated by the end of the first week of life often due to either apnoea or respiratory fatigue.6 However, looking at the low IVH rate in LISA infants, it seems to be of advantage to allow adaptation to extrauterine life under spontaneous breathing (see figure 3).
LISA is a safe procedure
LISA is a manipulation that requires specific skills and should therefore only be performed by neonatologists experienced in airway management. Videos to visualise and learn the procedure are available (eg, The Lancet TV: https://www.youtube.com/watch?v=IYf92NN1kV0) from different sources.5 Manikins simulating the airway anatomy in very premature babies in a realistic way have recently become available for training.
Failure to insert the catheter through the vocal cords at first attempt, significant surfactant reflux, acute desaturations, bradycardia and/or need for manual ventilation during LISA were observed in <10%5 to >30%16 of LISA/MIST manipulations. The highest incidence of such complications was reported in studies that treated relatively mature premature infants at a postnatal age of several hours in a setting that interrupted CPAP during the LISA procedure.11 16 19 To treat early with continued CPAP with a gentle approach, laryngoscopy seems to be of key importance to avoid discomfort as much as possible. Studies with continuous monitoring of saturation and regional (eg, also cerebral) saturation by near-infrared spectroscopy are under way.20
First results indicate that a careful direct laryngoscopy technique is important to avoid the complications described above. Relatively few infants demonstrate discomfort while surfactant is being instilled via the thin diameter tube. If that happens, the injection (usually over <2 min) can be slowed down. If apnoea occurs, manual breaths can be delivered via the CPAP device that should stay in place during the LISA procedure. Nowadays, atropine with the (theoretical) idea to reduce secretions and avoid bradycardia is rarely used.
In the NINSAPP trial,6 the matched-pair study7 and the meta-analyses,9 LISA was shown to reduce the incidence of IVH compared with controls. However, none of these studies had IVH as a primary endpoint and the meta-analyses are not very robust in terms of the diversity of the included studies. However, the findings are still reassuring as initially there were fears that the LISA manipulation shortly after delivery at a vulnerable developmental period may increase IVH incidence.
In a recent study an increase in the rate of focal intestinal perforation was observed in a subset of infants born at 23–24 weeks’ GA receiving LISA.8 This finding may be related to the distension of the fragile intestinal wall in consequence of the PEEP applied during non-invasive ventilation, but clearly more data are needed.
Small, retrospective follow-up studies on LISA infants suggested favourable neurocognitive outcome compared with historical controls.21 Unpublished data from the 5-year follow-up of LISA infants in the GNN cohort suggest better lung function (forced expiratory volume in 1 s) and better neuro-outcome/intellectual properties (Wechsler Preschool and Primary Scale of Intelligence score) in infants that received surfactant via LISA compared with infants that received surfactant via the standard route. All of these studies were non-randomised, so that selection bias is likely to account for part of the positive results that were observed in favour of LISA. In addition, Bayley scores differed widely between the different participating centres. In consequence, for the ongoing follow-up of the NINSAPP study, one team of investigators blinded to the study allocation of the infant’s treatment group now travels to the different study sites, so that investigators and equipment are identical for all infants. In addition, a group of normal newborns are investigated as a term control group, and for the school-age follow-up interviews the items picked are identical to the large German Study on Infant Health (https://www.kiggs-studie.de), which will allow comparability with a normal paediatric/youth cohort.
Beyond LISA
As the current LISA procedure is still connected with the discomfort of laryngoscopy, the search for gentler methods for surfactant delivery goes on. Surfactant deliveries via, for example, nebulisation, pharyngeal instillation, bronchoscope or laryngeal mask are alternative techniques that are currently being actively pursued in research, but have not yet been adopted to any significant degree into clinical practice.
Future research will include LISA with new synthetic surfactant preparations. The unique properties of surfactant as a ‘vehicle’ may be used to facilitate the spread of drugs to the peripheral airspaces in the lung. In this context for example, surfactant/budesonide mixtures are under investigation by various groups, connected with the hope to have good local effectiveness without relevant systemic side effects.
Conclusions
Surfactant administration via LISA is becoming more widely used in NICUs around the world.22–25 LISA has recently become an acknowledged alternative to the standard mode of surfactant delivery.
In meta-analyses LISA lowers the need for mechanical ventilation and improves outcome by reducing neonatal complications such as IVH and BPD. A large international trial (OPTIMIST study) is ongoing.26 Still, the search for even less invasive ways to deliver surfactant needs to go on.
Finally, LISA is not simply an isolated technical procedure for surfactant delivery but rather part of a comprehensive non-invasive approach supporting the concept of a gentle transition to the extrauterine world enabling preterm infants to benefit from the advantages of spontaneous breathing.
Acknowledgments
We are grateful for the support of the families and of the colleagues contributing to this network.
References
Footnotes
Contributors EH, CH and WG designed and/or debated the series of articles/studies, made editorial comments and assure the validity of the content. EH drafted this article initially, with comments and involvement from all authors.
Funding Clinical data on LISA in Germany were obtained from the German Neonatal Network (GNN; www.vlbw.de), which is sponsored by the German Ministry of Education and Research (BMBF grant no: 01ER0805 and 01ER1501).
Competing interests EH, CH and WG have received study support, honoraria for presentations and travel support from Chiesi Farmaceutici, a surfactant producer. EH and CH served as advisors for Draeger Medical, a company producing incubators, monitors and ventilators.
Ethics approval Approval by the local institutional review board for research in human subjects of the University of Lübeck (file number 08-022) and by the local ethic committees of all participating centres has been given.
Provenance and peer review Commissioned; externally peer reviewed.
Author note This manuscript is in part based on the results of an international meeting on less invasive surfactant application (LISA) that took place in Lübeck, Germany, on 31 May 2018. This workshop was sponsored by the German Research Foundation (DFG) (grant: DFG-He 2072-3).
Patient consent for publication Parental/guardian consent obtained.