Article Text

Abstract
Objective To compare neonatal outcomes in singletons versus multiples, first-born versus second-born multiples and monochorionic versus dichorionic/trichorionic multiples <33 weeks’ gestational age (GA) who received delayed cord clamping (DCC).
Design Retrospective, observational study of 529 preterm infants receiving ≥30 s DCC. Generalised estimating equations and mixed effects models were used to compare outcomes in singletons versus multiples and monochorionic versus dichorionic/trichorionic multiples. Wilcoxon signed-rank and McNemar tests were used to compare first-born versus second-born multiples.
Setting Level III neonatal intensive care unit, California, USA.
Patients 433 singletons and 96 multiples <33 weeks’ GA, born January 2008–December 2017, who received DCC.
Results 86% of multiples and 83% of singletons received DCC. Multiples had higher GA (31.0 weeks vs 30.6 weeks), more caesarean sections (91% vs 54%), fewer males (48% vs 62%) and higher 12–24 hour haematocrits (54.3 vs 50.5) than singletons. Haematocrit difference remained significant after adjusting for birth weight, delivery type and sex. Compared with first-born multiples, second-born multiples were smaller (1550 g vs 1438 g) and had lower survival without major morbidity (91% vs 77%). Survival without major morbidity was not significant after adjusting for birth weight. Compared with dichorionic/trichorionic multiples, monochorionic multiples had slightly lower admission temperatures (37.0°C vs 36.8°C), although this difference was not clinically significant. There were no other differences in delivery room, respiratory, haematological or neonatal outcomes between singletons and multiples or between multiples’ subgroups.
Conclusions Neonatal outcomes in preterm infants receiving DCC were comparable between singletons and multiples, first and second order multiples and monochorionic and dichorionic/trichorionic multiples.
- delayed cord clamping
- multiples
- preterm
- second-born multiple
- monochorionic multiple
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
What is already known on this topic?
Delayed cord clamping (DCC) is beneficial in preterm infants.
DCC is feasible and safe in dichorionic multiples.
What this study adds?
Multiples who receive DCC have similar outcomes to singletons who receive DCC.
Second-born multiples do not have worse outcomes than first-born multiples in those who receive DCC.
DCC is feasible in both monochorionic and dichorionic/trichorionic multiples.
Introduction
Delayed cord clamping (DCC) has been widely studied in preterm infants, decreasing the risk of intraventricular haemorrhage (IVH), necrotising enterocolitis (NEC) and transfusion.1 The most recent review showed a reduction in mortality.2 International/national organisations including the WHO, American College of Obstericians and Gynecologists and American Academy of Pediatrics’ Neonatal Resuscitation Program have recommended ≥30–60 s DCC for preterm infants.
Multiple pregnancies are unique situations where obstetricians and paediatricians may be hesitant to perform DCC due to concerns about placental vascular connections between fetuses in monochorionic placentation, second fetus well-being, difficulty extracting second fetuses during caesarean section (C-section) due to delay from the first infant’s delivery and increased risk for postpartum haemorrhage (PPH). Studies comparing neonatal outcomes between first-born and second-born multiples have shown that second twins are at higher risk for morbidity with lower Apgars, birth asphyxia, delivery room (DR) resuscitation and intubation, respiratory distress syndrome (RDS) and neonatal intensive care unit (NICU) complications.3–5
Inclusion of multiples has varied in DCC studies. Randomised control trials (RCTs) including multiples have not provided separate outcomes data for multiples.6 7 Observational studies confirmed that DCC was feasible in dichorionic twins <32 weeks’ gestational age (GA)8–10 and was associated with improved neonatal outcomes in multiples.8 These studies did not compare outcomes between first-born and second-born multiples or between monochorionic and dichorionic/trichorionic multiples. As DCC is becoming standard of care in preterm infants, there is paucity of evidence of its impact on very preterm multiples, especially first-born and second-born multiples and monochorionic multiples.
In 2007, we implemented DCC as standard of care for all preterm infants as part of a standardised DR bundle to reduce risk of IVH. This study’s objective was to evaluate neonatal outcomes in preterm infants <33 weeks’ GA who received DCC, comparing singletons and multiples, first-born and second-born multiples and monochorionic and dichorionic/trichorionic multiples.
Methods
Design
This is a retrospective, observational single-centre study. Data collection was approved by our institutional review board as a quality improvement (QI) project.
Setting and subjects
This study was conducted at a public safety-net hospital in California with a regional level III NICU. Our study included preterm infants <33 weeks’ GA who received ≥30 s DCC and were born January 2008–December 2017. Infants receiving <30 s DCC and multiples with intrauterine fetal demise (IUFD) of one twin were excluded.
Standardised DR management of preterm infants
In 2007, we implemented ≥30 s DCC for all very preterm infants as standardised DR management. DCC duration increased to ≥60 s in March 2011 and ≥120 s in July 2016. Our DCC procedure was based on the Mercer trial11 and was previously published.12 During DCC, an infant was placed on a portable warming mattress, and gentle stimulation and airway suctioning with a bulb syringe were performed as needed. After the first multiple was delivered, many obstetricians delivered second/third multiples while the first received DCC. This allowed providers to evaluate the well-being of all multiples during DCC. Occasionally, obstetricians delivered the first multiple and waited to deliver the next multiple until the first multiple’s cord was clamped. DCC was contraindicated if there was active maternal bleeding from abruption/placental disruption at time of delivery, cord tear/avulsion, en caul delivery, hydrops fetalis, recipient twin of severe twin-to-twin transfusion syndrome (TTTS) or severe anaemia from isoimmunisation. DCC was discontinued if an infant appeared lifeless or apnoeic despite stimulation and bulb suctioning for 30–45 s. Continuous positive airway pressure was initiated in all preterm infants after the cord was clamped as a DR standard.
Data collection
Maternal and neonatal demographics, and neonatal outcomes were obtained from our prospectively collected NICU database. Haematocrits, obtained when clinically indicated, and maternal estimated blood loss (EBL), documented in electronic medical records, were collected retrospectively. Haematocrits measured after packed red blood cell (RBC) transfusion were excluded.
Demographic variables included GA, birth weight (BW), antenatal steroids, C-section and sex; DR measures included 1 min Apgar <3 and 5 min Apgar <7, admission temperature, intubation, chest compressions and maternal EBL; respiratory outcomes included surfactant administration, any intubation during NICU stay and pneumothorax; haematological outcomes included haematocrits at 0–2 and 12–24 hours of life, polycythaemia (haematocrit >65%), peak bilirubin, exchange transfusion and RBC transfusions; and neonatal outcomes included severe IVH (grade 3 or 4), NEC (Bell stage ≥2), late-onset sepsis (LOS) (positive blood or cerebro spinal fluid culture >72 hours), chronic lung disease (CLD) (requiring oxygen/respiratory support at 36 weeks postmenstrual age), severe retinopathy of prematurity (ROP) (≥stage 3, plus disease or received anti-Vascular Endothelial Growth Factor), survival without major morbidity (survival without severe IVH, NEC, LOS, CLD and severe ROP) and death.
Analysis
Singleton versus multiples and monochorionic versus dichorionic multiples
Singletons versus multiples and monochorionic versus dichorionic/trichorionic multiples demographics, DR measures and outcomes were analysed using mixed effect (ME) and generalised estimating equation (GEE) models clustered around pregnancy to account for multiples. Continuous variables were analysed using ME with exchangeable covariance structures and restricted maximum likelihoods. Categorical variables were analysed using GEE with exchangeable correlation structures, logistic links and robust variance estimates. Maternal EBL was analysed using linear regression adjusting for C-section. Additional ME and GEE analyses were performed, with adjustments for baseline/demographic differences between groups.
All model residuals were assessed for normality, linearity and homoscedasticity. Correlation coefficients were used to assess for multicollinearity. Outlier residuals >2 SD were assessed by running each model with/without outliers.
First-born versus second-born multiples
Paired analyses were performed in first-born and second-born multiples who both received DCC to compare demographics, DR measures and outcomes between multiples from the same mother. The third-born triplet was excluded. Wilcoxon signed-rank test was used for continuous variables, and McNemar test was used for categorical variables. GEE analysis was performed adjusting for baseline BW difference to compare outcomes. Subgroup analysis was performed between monochorionic and dichorionic/trichorionic multiples. Stata V.14.0 was used for statistical analysis. A p value <0.05 was considered significant.
Results
DCC in multiples
During the study period, there were 640 preterm infants born at <33 weeks’ GA: 520 singletons and 120 multiples. Infants who did not receive DCC (n=103 [16%]: 87 singletons and 16 multiples), and multiples with IUFD of one twin (n=8) were excluded. The study included 529 infants (433 [82%] singletons, 96 [86%] multiples) who received ≥30 s DCC (figure 1). Fifty-four sets of multiples (n=112) were born: 50 sets of twins and 4 sets of triplets. There were 21 pairs of dichorionic-diamniotic twins, 27 pairs of monochorionic-diamniotic twins, 2 pairs of monochorionic-monoamniotic twins and 4 pairs of trichorionic-triamniotic triplets. Table 1 shows DCC achievement across all multiple types. Twenty-two pairs of monochorionic twins that received DCC were included. Eleven monochorionic twin pairs had >20% BW discordance; of those 11, 7 pairs had >5% haematocrit difference, and of those 7, 5 pairs had higher haematocrits in larger twins, suggestive of TTTS. None of these infants had polycythaemia, and only one had anaemia. Second-born twins were smaller in four of five pairs with TTTS.
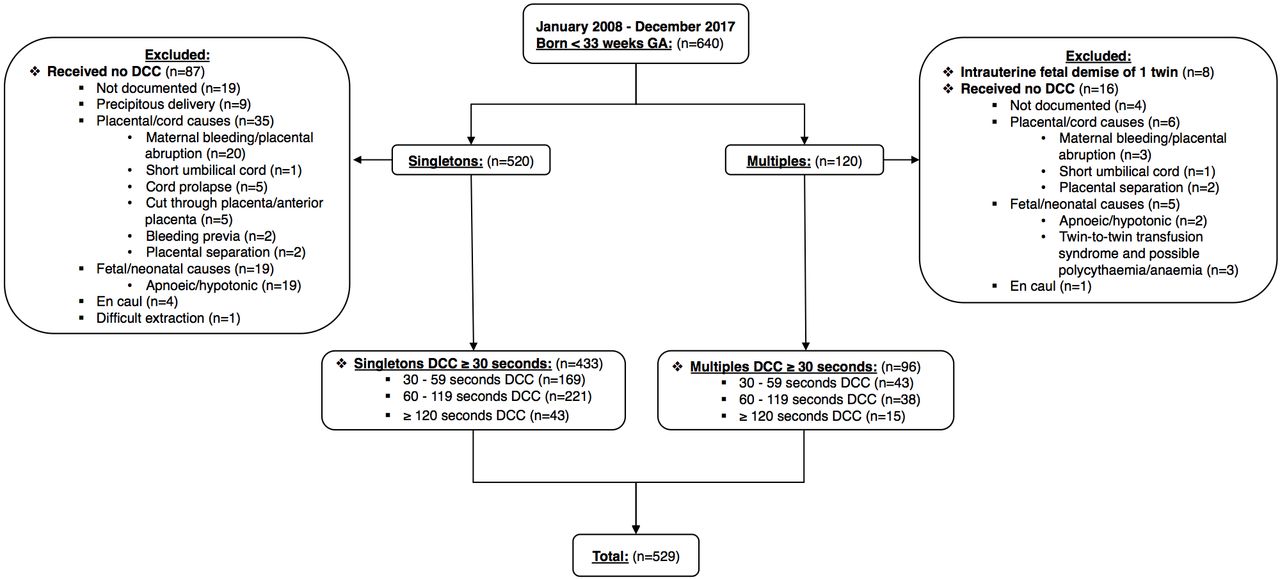
{kind=link}
Study subject selection for infants <33 weeks’ gestational age (GA). DCC, delayed cord clamping.
Delayed cord clamping (DCC) achievement in multiples
Singletons versus multiples
Neonatal and maternal demographics, DR measures, respiratory and haematological outcomes and neonatal mortality and morbidity of singletons and multiples are shown in table 2. Multiples had a higher GA (31.0 weeks vs 30.6 weeks, p=0.001), more C-sections (91% vs 54%, p<0.0001), fewer males (48% vs 62%, p=0.02) and higher 12–24 hour haematocrits (54.3 vs 50.5, p=0.01). The haematocrit difference remained significant after adjusting for BW, delivery type and sex (p=0.02). Mothers in the multiples group had higher EBL than those from the singletons group (800 mL vs 650 mL, p<0.0001) and higher risk of PPH (EBL >1000 mL) (23% vs 16%, p=0.04). These differences were not significant after adjusting for delivery type (EBL: p=0.1, PPH: p=0.3).
Singletons versus multiples: demographics, DR measures and outcomes
First-born versus second-born multiples
Neonatal and maternal demographics, DR measures, respiratory and haematological outcomes and neonatal mortality and morbidity of first-born and second-born multiples are shown in table 3. Second-born multiples had a lower BW compared with first-born multiples (1438 g vs 1550 g, p<0.02). Second-born multiples had lower survival without major morbidity (77% vs 91%, p=0.03). This difference was not significant after adjusting for BW (p=0.1).
First-born versus second-born multiples: demographics, DR measures and outcomes
Subgroup analysis between first-born and second-born monochorionic multiples showed that second-born multiples were smaller (1380 g vs 1510 g, p=0.008). Second-born twins had less surfactant administration (18% vs 36%, p=0.02) and higher 12–24 hour haematocrits (56.0 vs 52.7, p=0.02) after adjusting for BW.
Monochorionic versus dichorionic/trichorionic multiples
Neonatal and maternal demographics, DR measures, respiratory and haematological outcomes and neonatal mortality and morbidity of monochorionic and dichorionic/trichorionic multiples are shown in table 4. Monochorionic multiples had lower admission temperatures than dichorionic/trichorionic multiples (36.8°C vs 37.0°C, p=0.046), however this difference is not clinically significant.
Monochorionic versus dichorionic/trichorionic multiples: demographics, DR measures and outcomes
Discussion
Our single-centre study is one of the first to compare neonatal outcomes of preterm singletons and multiples, first-born and second-born multiples and monochorionic and dichorionic/trichorionic multiples, all receiving DCC. Neonatal outcomes were comparable for infants born at <33 weeks’ GA, both for singletons and multiples and for first-born and second-born multiples.
Singletons versus multiples
Of many DCC RCTs, only a few included multiples.6 7 13 The Australian Placental Transfusion Study (APTS) is the largest DCC RCT, having 196 preterm multiples <30 weeks’ GA in their DCC group. In 2017, a meta-analysis including APTS showed a 32% reduction in mortality in preterm infants who received DCC.2 A QI study showed successful implementation of DCC in 77% of preterm singletons and multiples. Their DCC cohort, which included 25% multiples (n=41), had fewer DR intubations, less metabolic acidosis and higher haematocrits.9 A pre/postintervention study showed that preterm twins receiving DCC required fewer transfusions and surfactant treatment for RDS compared with infants receiving early cord clamping.8
Our study showed that DCC was feasible in 86% multiples, and outcomes were comparable with singletons who received DCC. DCC was beneficial to singletons and multiples; in fact, multiples had higher haematocrits than singletons. We did not compare outcomes between multiples who received DCC versus no DCC because 23% of our infants did not receive DCC due to needing immediate resuscitation, and 40% due to maternal bleeding/placental disruption. Hence, multiples who did and did not receive DCC are not comparable.
Maternal haemorrhage
One study found no difference in maternal EBL in vaginal or C-section deliveries in preterm multiples who received 30–60 s DCC compared with multiples with no DCC (<30 s).10 In our study, maternal EBL was higher during delivery of multiples than singletons. However, this difference was not significant after adjusting for delivery type. During our 10-year study period, DCC duration was gradually increased from 30 s to 2 min. Our obstetricians developed a practice of delivering both or all multiples and leaving them side-by-side outside of the uterus to evaluate the well-being of second-born and third-born multiples when present. This practice allowed the overall time between the first multiple’s delivery and the last multiple’s cord clamping to be shorter than the additive duration of DCC for each infant.
First-born versus second-born multiples
Studies have shown that second-born multiples have worse outcomes in almost every category compared with first-born including mortality, Apgars, RDS, intubation and resuscitation.3–5 One study showed that second-born multiples had more neonatal complications, especially in infants with BW <1500 g and non-vertex presentation in the second twin.3 Major contributors of morbidity in second twins have been birth asphyxia and RDS.4 5 Biological sex has contributed to first and second twin outcome discrepancy, with male second twins generally having worse outcomes than female second twins.4
We did not observe a significant difference in DR measures, haematological and respiratory outcomes or neonatal mortality and morbidity when both first-born and second-born multiples received DCC. Second-born multiples in our cohort had lower survival without major morbidity; however, second-born multiples were smaller than first-born (BW 1438 g vs 1550 g). The difference in survival without major morbidity between first-born and second-born multiples disappeared after adjusting for BW. Our study suggests that in the cohort where both first-born and second-born preterm infants received DCC, the second-born may not be at an increased risk for worse outcomes. During our study period, first-born and second-born multiples received DCC in 80% multiple births. The 20% who did not receive DCC may have additional risk factors, and second-born multiples in that population may have worse outcomes than first. Regardless, in those multiples who receive DCC, it is reassuring that second-born multiples do not have worse outcomes.
Monochorionic versus dichorionic/trichorionic multiples
Monochorionic multiples present a unique challenge to implementing DCC due to TTTS complications and concerns about putting the second twin’s well-being at risk while performing DCC on the first. Many studies excluded monochorionic multiples or a subset of those who fit TTTS diagnostic criteria.4 7 9 Studies including monochorionic multiples had very small sample sizes.8 10 Another study with more multiples did not specify results according to chorionicity.6 Our study had 22 pairs of monochorionic multiples who both received DCC. We compared outcomes between monochorionic first-born and second-born multiples and showed that second-born multiples had less surfactant administration and higher haematocrits, while all other outcomes were comparable. There was no difference between first-born and second-born multiples in the dichorionic/trichorionic subgroup.
BW discordance from TTTS contributes to adverse outcomes in second twins.4 5 Rates of neonatal morbidity are highest in twins with BW discordance >20%.4 This is especially significant when second twins have a higher BW, contributing to fetal distress, oxygen insufficiency, RDS and lower Apgars in second twins.4 However, second twins <1500 g require more intubation and resuscitation, and are more likely to die of complications.3 Many prior DCC studies excluded monochorionic twins with >20% BW discordance. Eleven of our monochorionic twins had >20% BW discordance. Of the five pairs who had haematocrits suggestive of TTTS, only one pair was prenatally identified as having TTTS, and others were noted as having discordant twins. Neonatal mortality and morbidity outcomes were not different between first-born and second-born multiples in the monochorionic subgroup, although there is suggestion of second twins having worse outcomes (CLD and survival without major morbidity).
Limitations
Our study has limitations as a single-centre observational study. Selection bias related to implementing DCC could influence internal and external validity of results. Neonatal outcomes were not analysed for approximately 20% of infants born in our centre who did not receive DCC. Since the study was conducted over a decade, our goal for minimum DCC duration increased from 30 s in 2008 to 120 s in 2016. Because our centre’s obstetric and neonatal teams became more comfortable implementing DCC over time, generalisability of results may be limited to centres with similar experience implementing DCC. Our sample size of multiples was relatively small to be confident about subgroup analysis results for different multiple types.
Conclusion
Our study shows that it is feasible and safe to implement ≥30 s DCC in preterm multiples born at <33 weeks’ GA. Neonatal outcomes in multiples are no different from singletons, and second-born multiples have similar outcomes to first-born multiples. Monochorionic multiples did not display worse outcomes than dichorionic/trichorionic multiples. Given our sample size, there may be insufficient power to detect differences between subgroups. Our results need to be validated by larger studies.
Acknowledgments
Gratitude is expressed to our patients and families and for the extreme dedication of Santa Clara Valley Medical Center (SCVMC) neonatal intensive care unit (NICU) and labor and delivery nursing staff, respiratory therapists, neonatal nurse practitioners, neonatologists, neonatal hospitalists, NICU database team, obstetricians, perinatologists, Stanford University paediatric house staff and SCVMC obstetric house staff and Santa Clara County First Five and Valley Medical Center Foundation.
Footnotes
Contributors PJ, DS and BG conceived the idea and developed the methodology. EB assisted in data collection, statistical analysis and wrote the first draft of the manuscript. MN performed the statistical analysis. All authors developed and approved the final manuscript. This publication is the work of the authors, and PJ will serve as guarantor for the contents of this paper.
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Competing interests None declared.
Ethics approval The data collection for this retrospective study was approved by our Institutional Review Board as a Quality Improvement project evaluating the outcomes of very preterm infants.
Provenance and peer review Not commissioned; externally peer reviewed.
Data sharing statement The data sets used and analysed for this study will be made available on request.
Patient consent for publication Not required.
Linked Articles
- Fantoms