Article Text

Abstract
Objective To investigate the feasibility of determining the pattern and prevalence of alcohol consumption in pregnancy by measuring ethanol biomarkers in meconium.
Design Population-based observational study.
Setting Inner-city maternity unit in Scotland, UK.
Population Random sample of singleton infants delivered after 36 completed weeks’ gestation.
Methods Fatty acid ethyl esters (FAEEs) and ethyl glucuronide (EtG) in meconium were measured by liquid chromatography-mass spectroscopy. Samples were frozen at −20°C before analysis. Results were compared anonymously with demographic data including maternal age, parity, smoking, ethnicity and postcode and with infant gestation, birth weight and head circumference. Written informed consent was obtained from all subjects.
Results 235 samples of meconium were analysed (70% of eligible babies). Only four (1%) of mothers declined to participate. FAAEs were detected in all, including four samples below the limit of quantification (10 ng/g). 98 (42%) samples had FAEE concentrations >600 ng/g. EtG was detectable in 93 (40%) samples; in 35 (15%) EtG concentration was >30 ng/g. No mother reported heavy alcohol consumption in pregnancy. FAAE concentration correlated with EtG (Pearson’s coefficient; p<0.001). There was no association between either biomarker and maternal age, parity, smoking, ethnicity or postcode, or infant gestation, birth weight or head circumference.
Conclusion Measurement of ethanol biomarkers in meconium is a feasible tool for determining the pattern and prevalence of alcohol consumption in pregnancy. Data suggest that at least 15% of pregnant women in the west of Scotland are consuming significant quantities of alcohol during latter pregnancy.
- fatty acid ethyl esters
- ethylglucuronide
- meconium
- newborn
Statistics from Altmetric.com
What is already known on this topic?
Alcohol use in pregnancy is commonly under-reported and direct measurement of alcohol metabolites in mothers is difficult due to its rapid metabolism.
Biomarkers of alcohol can be measured in meconium to assess continuing alcohol use in pregnancy.
What this study adds?
Confirms under-reporting of alcohol use in pregnancy.
Measurement of ethanol biomarkers in meconium is a feasible tool for determining the pattern and prevalence of alcohol consumption in pregnancy.
Introduction
The effects of excess alcohol consumption are estimated to cost the National Health Service in England and Wales >£3.5 billion per year with a total annual cost to society of around £21 billion.1 In Scotland, although alcohol use has been falling over the past decade, the majority of women drink alcohol, with 60%–70% of women aged 16–44 classified as moderate drinkers (consuming up to 14 units per week) and 13%–24% of women drinking hazardously (>14 units per week).2 Data suggest that hazardous alcohol consumption is most common in women in highest income households compared with those in the lowest income households (22% vs 13%).2 3 Ethanol is teratogenic and the current UK government recommendations are for complete abstinence from alcohol consumption during pregnancy.4 Despite this advice, some women drink heavily before they realise they are pregnant, and others continue to drink through their pregnancy.5 Prenatal alcohol exposure (PAE) may lead to miscarriage, premature birth and increased perinatal morbidity and mortality.6 7Fetal alcohol spectrum disorder (FASD) describes a continuum of difficulties with learning, development, attention, social relationships and impulsive behaviour. At the severe end of the spectrum, fetal alcohol syndrome (FAS) is characterised by intrauterine growth restriction, reduced head circumference with poor postnatal growth, and typical craniofacial features.6 7 Based on a recent American study, up to 5% of school-age children in the USA and Western Europe may be affected by FAS/FASD.8 Since pregnant women commonly under-report alcohol use in pregnancy,9 10 and direct measurement of alcohol metabolites in the mother is difficult due to rapid metabolism of alcohol, the exact prevalence of FAS/FASD in the UK is unknown.
An alternative to self-reporting of alcohol consumption is the measurement of ethanol biomarkers in meconium.11–17 Ethyl glucuronide (EtG) is formed in the mother from conjugation of ethanol with glucuronic acid, which crosses the placenta and is deposited in meconium.12 Ethanol that has directly crossed the placenta is metabolised by the fetal liver to fatty acid ethyl esters (FAEEs).11 Since meconium begins to be formed from 12 to 20 weeks gestation when fetal swallowing of the amniotic fluid begins,11 postnatal measurement of ethanol biomarkers in meconium reflects PAE over several months prior to delivery. FAEE measurement in meconium may be 5–9 times more sensitive than self-reported alcohol consumption.18
Small amounts of FAEEs are produced endogenously from gut microflora, but concentrations>600 ng/g in meconium have been related to regular alcohol consumption during pregnancy of >2 drinks per day or binge drinking of >5 drinks per occasion.15 Concentrations of EtG >30 ng/g in meconium have relatively high sensitivity and specificity for regular alcohol consumption in pregnancy.12 Measurement of these biomarkers in meconium has the potential to provide more accurate data on alcohol consumption during pregnancy than maternal self-reporting. Such data are essential for targeting and subsequently evaluating interventions aimed at reducing alcohol consumption during pregnancy.
To date few data have been published regarding the demographic associations of excess alcohol consumption during pregnancy within geographical areas. In this study, we aimed to assess the feasibility of FAEE and EtG measurement in meconium as an estimate of alcohol consumption in pregnancy in an unselected population, and to explore relationships between these biomarkers and demographic factors including maternal age, parity, smoking, ethnicity and socioeconomic status, as well as infant birth weight and head circumference.
Methods
This observational study was carried out at the Princess Royal Maternity (PRM) in Glasgow, Scotland, over a 6-month period. The PRM serves the inner-city and northern and eastern suburbs of Glasgow, with an average of 6000 births annually. All mothers delivering singleton infants born after 36 completed weeks’ gestation, during every eighth 24-hour period over 5 months, were eligible for inclusion. Multiple births were excluded.
Meconium collection and analysis
Immediately after birth all eligible mothers were supplied with a disposable plastic bag and asked to retain their infant’s first meconium for analysis. Samples of meconium were collected into anonymised, sequentially numbered containers. Where possible the first meconium sample was collected, but the second sample was accepted if the first had been missed.
Since FAEEs are unstable at room temperature, samples were frozen at −20°C and transported on dry ice to the University of Firenze and Padova in Italy for analysis. A fully validated method was used for the determination of four FAEEs (ethyl myristate, ethyl palmitate, ethyl oleate and ethyl stearate) and EtG by liquid chromatography-tandem mass spectrometry.19 To summarise, 200 mg of meconium was sonicated for 15 min in the presence of 20 ng of EtG-d5 and 200 ng of each FAEE-d5. The supernatant was added to an aminopropyl solid-phase extraction cartridge, preconditioned with 2 mL of methanol, water and acetonitrile (ACN). FAEEs were eluted with 2 mL of hexane and EtG elution carried out with 2 mL of water. The two mixtures were dried under nitrogen stream and recovered with 50 µL of ACN (FAEE) and 50 µL of methanol (EtG). FAEEs were detected following separation using a C8 reversed-phase column. A C18 reversed-phase column was used in isocratic mode (1% ACN) for EtG detection. Acquisition was in multiple reaction monitoring for all of the analytes, in positive mode for FAEEs and negative mode for EtG. Lower limit of quantification (LLOQ) values were 10–15 ng/g for FAEEs and 10 ng/g for EtG.
Demographic information
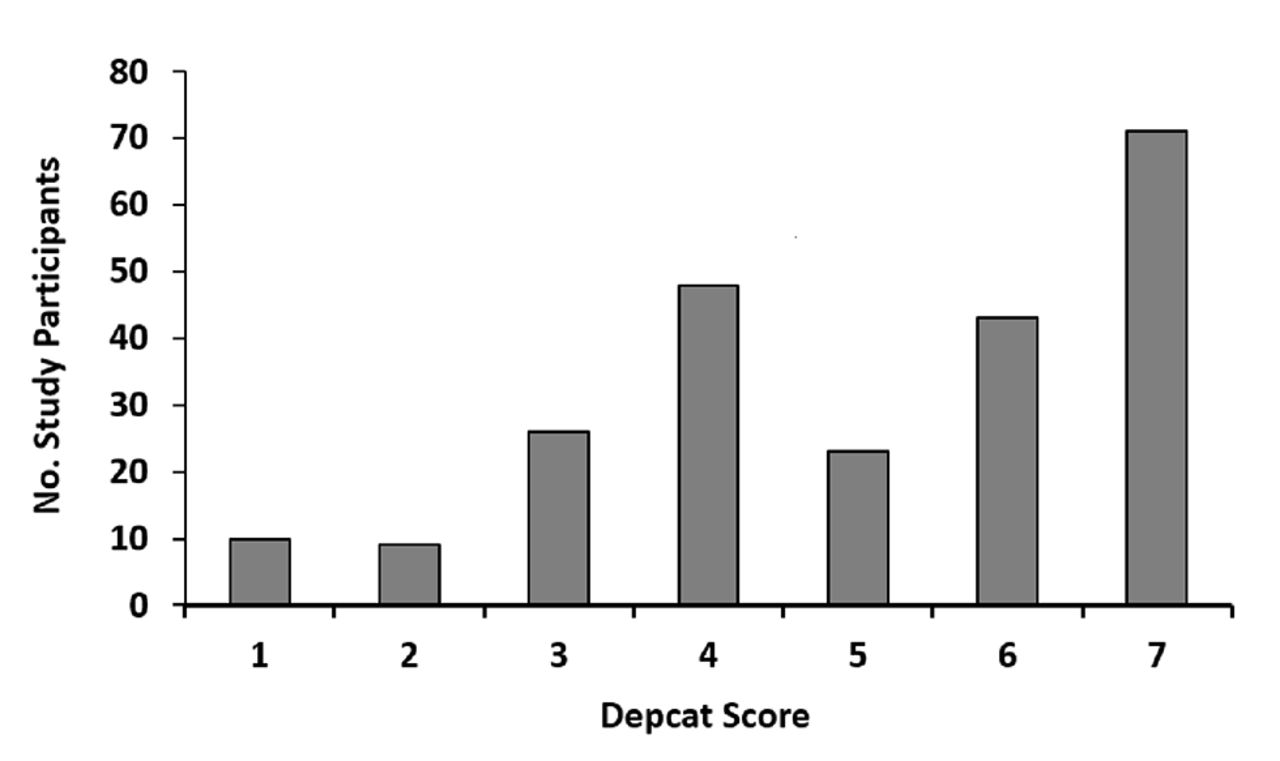
All mothers were approached by one of two researchers shortly after delivery and asked to complete a short informal questionnaire regarding their alcohol consumption during pregnancy. The questionnaire enquired with regards to quantity (number of units) and frequency of alcohol intake during their pregnancy. Patient records were consulted for demographic information regarding maternal age, parity, ethnicity, smoking status, postcode, gestation, birth weight and occipital frontal head circumference, which were recorded onto anonymised numbered datasheets matched in number to the corresponding meconium sample. Maternal postcode of residence was used to derive a DEPCAT. This is a score ranging from 1 to 7 assigned to every postcode area within Scotland that reflects socioeconomic status, with 1 being the most affluent and 7 the most deprived.20
Results
Study population
In total, 329 infants were born during the study period. Written consent was obtained from 325mothers. In three of the four non-consenting cases, informed consent was not sought due to maternal lack of fluency in English and unavailability of an interpreter. Only one mother actively declined to participate in the study (figure 1). Ninety meconium samples were not collected from babies whose mothers had consented either due to the meconium sample inadvertently being discarded or due to discharge of the mother and infant prior to passage of meconium. The eligible subjects from whom a meconium sample was not obtained did not differ in any way, with regard to maternal or infant characteristics from those mothers and babies who did participate in the study. In total, 235(70% of eligible infants) samples were available for analysis, all of which were collected within 48 hours of birth and were of sufficient quantity and quality to be processed.
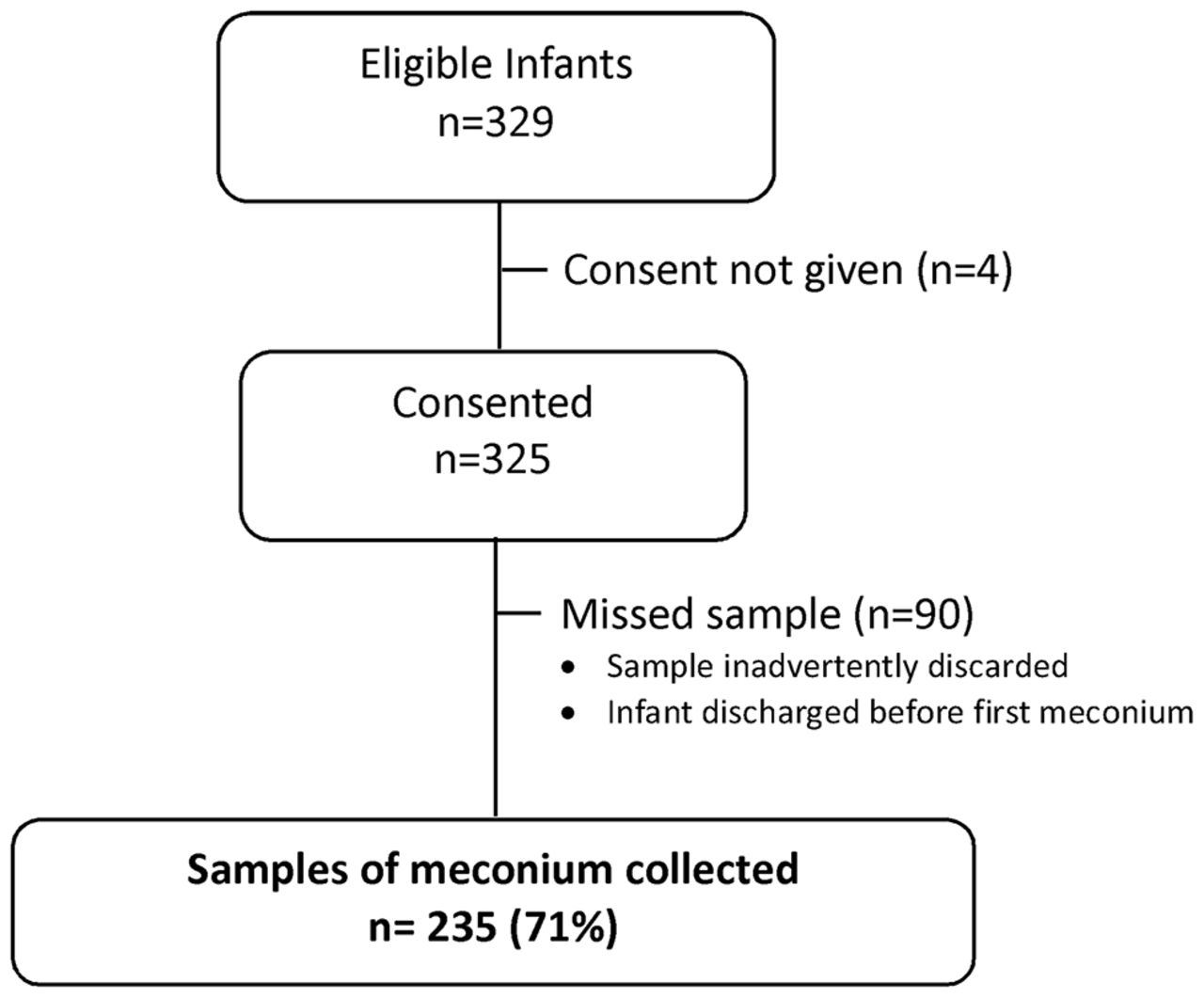
Consort of recruited study participants.
Table 1 shows the demographics of the population studied. Almost 50% of participants had a DEPCAT score of 6 or 7 and only 8% of the study population resided in the most affluent postcode areas (figure 2). Six mothers self-reported alcohol consumption during pregnancy, quantified as ‘light social drinking only’. No mother reported consuming large amounts of alcohol during pregnancy. The six mothers who declared some alcohol consumption were of varying age, parity and DEPCAT score.
Demographic data of population studied

Number of study participants for each DEPCAT score.
Ethanol biomarker levels
FAEEs were detected in 100% of the samples. Four (2%) samples had a total concentration of FAEEs below the LLOQ. Ninety-eight (42%) of samples had concentrations of FAEES >600 ng/g. EtG was detected in 93 (40%) of samples, of which 23 samples had EtG concentrations less than the LLOQ. Thirty-five samples (15% of all samples) had EtG concentrations>30 ng/g.
There was correlation between the concentrations of FAEEs and EtG (Pearson 0.327; p<0.001) (figure 3).

{kind=link}
{kind=link}
{kind=link}
Fatty acid ethyl ester (FAEE) versus ethyl glucuronide (EtG) concentrations.
Demographic associations with elevated biomarker levels
There was no significant association between either FAEE or EtG and any maternal or infant demographic factors (tables 2 and 3). There was a tendency towards a higher proportion of elevated FAEE in more affluent women, but the total number of women in these groups was low, and the differences were not significant (p=0.07, Mann-Whitney test). Infants born in February were more likely to have FAEE concentrations>600 ng/g (p<0.05, χ2), but were not more likely to have elevated EtG concentrations in meconium.
Demographic factors associated with fatty acid ethyl ester (FAEE) concentrations
Demographic factors associated with ethyl glucuronide (EtG) concentrations
Discussion
This pilot study demonstrates the feasibility of collecting anonymised meconium samples for population studies of alcohol consumption in pregnancy. Only one mother actively declined to participate in the study, although it is possible that some of the missing samples reflected tacit reluctance to participate. The study was generally favourably reviewed by midwifery staff who greatly facilitated sample collection.
As well as reflecting alcohol consumption, FAEEs may originate from endogenous ethanol production or from ethanol traces contained in common foods.17 This would explain the fact that traces of FAEEs were found in all meconium specimens analysed. A cut-off concentration of >600 ng/g in meconium is commonly used to indicate alcohol exposure and has been validated in populations with documented heavy alcohol consumption.16 A recent systematic review of alcohol biomarkers by McQuire et al has shown that using a cut-off of 600 ng FAEEs per gram of meconium has a high sensitivity (82%–100%) for detection of significant alcohol consumption in pregnancy but a variable specificity (13%–98%).21 Assuming that self-reporting in a known alcohol consuming population is accurate, this translates to a positive predictive value of 55%. The percentage of tests with FAEE concentrations >600 ng/g (42%) in our study is among the highest reported in the literature, but comparable with two larger studies from Spain16 and Uruguay.22 Although total FAEE concentration was higher among Spanish women who used illicit substances including opioids, cocaine and cannabis, in Garcia-Algar et al’s study the proportion of samples with FAEE concentrations >600 ng/g was 45% regardless of concomitant illicit drug use. The subjects in the latter study were described as ‘low socioeconomic status’16 consistent with our population who had a median DEPCAT score of 6.5 8 Hutson et al’s study included a group of women with an 84% unemployment rate and also found FAEE concentrations >600 ng/g in 44% of meconium samples.22 The incidence of raised FAEE concentration in our study was considerably higher than results from studies from Germany (cut-off 500 ng/g), Canada (cut-off 600 ng/g) and Italy (cut-off 600 ng/g) which reported raised FAEE concentrations in 7.1%, 3.5% and 7.9% of samples, respectively.11 13 23 FAEE concentrations may be falsely raised if meconium sample collection is delayed or not frozen immediately after collection, with a median time of 59 hours for the appearance of FAEEs in meconium if the sample is left at room temperature for ≥12 hours or is refrigerated rather than frozen.11 24 In our study, even if we were not able to collect the first meconium sample, all samples were collected within 48 hours of birth and were rapidly frozen at −20°C, so this is an unlikely explanation for our FAEE results. Consumption of olive oil has been described as contributing to FAEEs in meconium,16 but this is an unlikely contribution to elevated FAEE concentrations in meconium for the majority of babies born in the west of Scotland. In a previous study from our group, 47% of meconium samples from opioid dependent mothers had FAEE concentrations >10 000 ng/g.18 Only one sample in the current study had concentrations of FAEEs >10 000 ng/g, suggesting that extremely high alcohol consumption in pregnancy may be confined to particular groups of vulnerable women.
Since EtG is only produced from ethanol metabolism, it is likely to be a more accurate biomarker of alcohol consumption.13 23 The prevalence of raised EtG in our study was comparable to that reported by Bakdash et al, who reported meconium EtG concentrations >30 ng/g in 16.3% of cases in a maternal health evaluation study.13 The 3% of women who admitted to consuming alcohol during pregnancy in our study is similar to the 1% who declared alcohol consumption in Bakdash et al’s study. If a positive predictive value of 55% is assumed for FAEE concentration >600 ng/g, both alcohol biomarkers are reasonably consistent and suggest a prevalence of significant alcohol consumption in pregnancy in the west of Scotland of the order of 15%–25%.
This study found no significant associations between raised ethanol biomarkers in meconium and maternal age, parity, ethnicity or smoking status. Alcohol consumption in pregnancy is commonly assumed to be associated with poverty, but there are no published data to confirm this,The Scottish Health Survey 2014 reported a greater likelihood of alcohol consumption during pregnancy in women from higher social classes with higher incomes and who shared their home with a partner.2 In our study, babies of mothers living in more affluent areas were more likely to have FAEE concentrations>600 ng/g but this difference was not significant, perhaps reflective of small study numbers.
Mothers of infants with concentrations of FAEEs of >600 ng/g were more likely to have smoked in pregnancy, but the difference was not significant. Co-dependency on nicotine and alcohol is well documented and likely to be multifactorial,25 so this may well be a true finding, limited by small study numbers.
One of the strengths of this study is its generalisability. By seeking to recruit all babies born in every 24-hour period, every eighth day, we identified a random cohort. We specifically did not target women with a known history of drinking in pregnancy. Limitations of this study include relatively small numbers, particularly in some demographic groups. Since meconium is not a routinely collected substance, we were bound by the terms of our Ethics Committee to obtain informed consent from mothers to retain their infant’s meconium. Despite the anonymous nature of the study, it is possible that some mothers who had consumed alcohol throughout pregnancy consented to the study but chose not to provide a sample of their infant’s meconium and reported this as accidentally discarded. If this was indeed the case, the study would tend to underestimate the incidence of alcohol consumption in pregnancy. Seventy-five per cent of meconium is formed during the last eight weeks of pregnancy,13 17 therefore measurement of biomarkers mostly reflects alcohol consumption in the third trimester and may miss a proportion of women who cease drinking during the course of the pregnancy.
Conclusion
This study confirms that women in the west of Scotland under-report their alcohol consumption during pregnancy. Analysis of FAEE and EtG in meconium is a feasible and acceptable tool for estimating alcohol consumption patterns in pregnancy.
Acknowledgments
The authors thank Dr David Young for help with statistical analyses.
References
Footnotes
CA and KEMC contributed equally.
Contributors CCA: recruited patients and drafted initial manuscript. KMcC: recruited patients and extensively revised manuscript. GC: involved in study design and contributed to revisions of manuscript. DF: oversaw analyses of samples. FV and EB: analysed samples and contributed to revisions of the manuscript. HM: conceived study and extensively revised the manuscript. All authors approved the final version of the manuscript.
Funding The study was funded by a grant from Scottish government (CASE 126426/Meconium).
Competing interests None declared.
Patient consent Obtained.
Ethics approval The study was approved by West of Scotland Ethics Committee 4.
Provenance and peer review Not commissioned; externally peer reviewed.