Article Text

Abstract
Objective To evaluate the safety of an aerosolised surfactant, SF-RI 1, administered via nasal continuous positive airway pressure (nCPAP) and a prototype breath synchronisation device (AeroFact), to preterm infants with respiratory distress syndrome (RDS).
Design Multicentre, open-label, dose-escalation study with historical controls.
Setting Newborn intensive care units at Mater Mothers’ Hospital, Brisbane, and Royal Hospital for Women, Sydney, Australia.
Patients Infants 26 weeks through 30 weeks gestation who required nCPAP 6–8 cmH2O and fraction of inspired oxygen (FiO2) <0.30 at <2 hours of age.
Interventions In part 1, infants received a single dose of 216 mg/kg of aerosolised surfactant. In part 2, infants could receive up to four doses of aerosolised surfactant. Three historical control infants were matched for each enrolled infant.
Main outcome measures Treatment failure was defined as Respiratory Severity Score (FiO2×cmH2O nCPAP) >2.4, nCPAP >8 cmH2O, arterial carbon dioxide >65 mm Hg, pH <7.20 or three severe apnoeas within 6 hours during the first 72 hours of life. Other outcomes included tolerance of the AeroFact treatment and complications of prematurity.
Results 10 infants were enrolled in part 1 and 21 in part 2 and were compared with 93 historical controls. No safety issues were identified. In part 2, 6 of 21 (29%) AeroFact-treated infants compared with 30 of 63 (48%) control infants met failure criteria. Kaplan-Meier analysis of patients in part 2 showed a trend towards decreased rate of study failure in the AeroFact-treated infants compared with historical controls (p=0.10).
Conclusion The AeroFact system can safely deliver aerosolised surfactant to preterm infants with RDS who are on nCPAP.
Trial registration number ACTRN12617001458325.
- neonatology
- therapeutics
Data availability statement
Data are available upon reasonable request. Data not included in the article text may be available for subsequent meta-analysis. Please contact the corresponding author for details.
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
What is already known on this topic?
Respiratory distress syndrome is a serious disorder of pulmonary insufficiency in preterm infants that can be treated or prevented with surfactant administration.
There is growing interest in non-invasive techniques, including aerosolisation, to deliver surfactant without the potential trauma of intubation.
What this study adds?
We tested a novel prototype device/drug combination (AeroFact) that delivers small aerosol particles of surfactant, synchronised with the infant’s respiratory cycle, to preterm infants.
This technique appears to be safe and well tolerated.
Background
Treatment with exogenous surfactant, administered by endotracheal intubation or tracheal cannulation and bolus instillation, has been key in improving morbidity and mortality of infants with respiratory distress syndrome (RDS) for more than 30 years.1 Currently, many clinicians defer bolus surfactant administration until RDS has progressed to clinically moderate or severe levels, in the hope of avoiding the adverse impact of intubation and endotracheal ventilation. However, delayed surfactant therapy can lead to atelectasis, increased oxygen requirements, barotrauma, ventilation/perfusion mismatch and development of bronchopulmonary dysplasia (BPD).2 3 Even brief intubation or tracheal cannulation to administer bolus surfactant remains an invasive procedure requiring specialised skills and may be associated with airway tissue trauma, hypoxia and bradycardia.2–5 The option to deliver surfactant therapy by aerosol, without intubation or tracheal cannulation, would be advantageous.6
The delivery of aerosolised surfactant for RDS was first attempted, with minimal success, by Chu et al in 1967.7 In 1997, a pilot study in preterm infants of SF-RI 1 surfactant (now marketed as Alveofact), aerosolised with a jet nebuliser and delivered via pharyngeal continuous positive airway pressure (CPAP), showed improved oxygenation following treatment.8 Subsequent reports of aerosolised surfactant showed problems in delivering an effective dose to the lungs, presumably related to aerosolisation technique and/or the physical characteristics of different types of surfactant.9–14 It has been suggested that effective aerosol surfactant delivery might depend on a combination of different aerosolisation techniques to achieve smaller droplet size, use of undiluted surfactant and breath synchronisation so that surfactant is not generated and wasted during exhalation.6 15 Recent animal studies suggest that aerosolised surfactant can be delivered effectively.16–18
Objectives
We hypothesised that the AeroFact device/drug system would deliver aerosolised surfactant to preterm infants with RDS who were on nasal continuous positive airway pressure (nCPAP) and that it would be safe and well tolerated. The primary objective was to compare the outcomes of AeroFact treatment of infants with RDS who were 26 weeks through 30 weeks postmenstrual age with historical controls who were initially treated with nCPAP without prior installation of surfactant. The secondary objectives included determining if AeroFact treatment would reduce the number of infants whose RDS worsened until they met failure criteria and were treated with bolus surfactant, compared with historical controls.
Infants were enrolled after obtaining written informed parental consent.
Materials and methods
This was a multicentre, open-label, dose-escalation study comparing enrolled infants with matched historical controls. The protocol was divided into two parts. In part 1, patients received a single AeroFact treatment. In part 2 of the study, patients could receive a maximum of four AeroFact treatments within 96 hours. Part 2 was started only after review of part 1 data by an independent data safety monitoring board.
Study population
The study was conducted in the newborn intensive care units (NICUs) at Mater Mothers’ Hospital, Brisbane, and Royal Hospital for Women, Sydney, Australia in 2017–2018. Infants 26 weeks and 0 days through 30 weeks and 6 days postmenstrual age, with weight appropriate for gestational age, were eligible for enrolment if they had RDS, received nCPAP within 15 min of birth, required fraction of inspired oxygen (FiO2) <0.30 while on nCPAP 6–8 cmH2O, and could be placed on AeroFact at ≤2 hours of age. Infants were excluded if they had a 5 min Apgar score ≤5, received chest compressions or medications for resuscitation in the delivery room, had premature rupture of membranes >7 days, received mechanical ventilation within 30 min of birth or had received endotracheal liquid surfactant. Other exclusion criteria included significant congenital anomaly, diseases interfering with cardiopulmonary function, known or suspected chromosomal abnormality, treatment with inhaled nitric oxide, evidence of chorioamnionitis or uncertainty about commitment to providing ongoing care.
Each treated patient was matched to three historical control infants. The historical controls were born in the previous 2 years at the same hospital, had been resuscitated in the delivery room with CPAP only (ie, no surfactant instillation), were matched for gestational age, gender and antenatal steroid status, and met none of the exclusion criteria.
Device/drug description
The AeroFact device/drug combination is an investigational prototype consisting of three basic components: (1) single-patient single-use disposable nebuliser, drug delivery circuit and breath sensor; (2) reusable device controller; and (3) SF-RI 1 surfactant. SF-RI 1 surfactant is now produced by Lyomark Pharma (Germany) and marketed as Alveofact. It is derived from bovine lung lavage and is lyophilised then reconstituted. It was originally approved 30 years ago, and since it is available in more than 20 countries for use as a liquid bolus to treat infants with RDS, it has the potential for widespread availability if nebulised administration via CPAP proves effective.
The AeroFact device generates a fine droplet aerosol of undiluted surfactant suspension which is delivered to short nCPAP prongs and is synchronised with inspiration. The surfactant droplet size is <3 µm mass median aerodynamic diameter (MMAD), significantly smaller than the droplets produced by jet nebulisers.6 Smaller droplet size is associated with significantly more effective pulmonary delivery in small primates,19 as suggested by models predicting aerosol deposition.15 By synchronising aerosolisation with inspiration, the AeroFact device minimises the drug loss that occurs if aerosolisation continues during the infant’s expiratory phase. Synchronisation was accomplished with a sensor placed in the inspiratory limb of the CPAP circuit, sensing the flow increase associated with inspiration. Preliminary studies showed that this technique detected >85% of all breaths.
Study protocol
Infants were initially stabilised in the delivery room and NICU by adjusting nCPAP and FiO2 to maintain blood gases and oxygen saturation (SpO2) within clinical guidelines. Following stabilisation on nCPAP and informed consent, treatment with AeroFact aerosolised surfactant was started within 2 hours of birth. Infants were maintained on nCPAP or nasal intermittent positive pressure ventilation until they either no longer needed respiratory support or they met treatment failure criteria. For part 2, AeroFact retreatment occurred if the Respiratory Severity Score (RSS, cmH2O nCPAP×FiO2) while on nCPAP was ≥2.0 to maintain SpO2 of 90%–95%, and at least 2 hours had elapsed since the end of the first dose, or at least 4 hours had elapsed since the end of the second or third dose. Treatment failure was defined as one or more of the following: RSS ≥2.4, arterial carbon dioxide >65 mm Hg, pH <7.20, nCPAP >8 cmH2O or three severe apnoeas with bradycardia within 6 hours requiring escalation of support. These criteria for treatment failure were selected to match current standard of care for administration of bolus liquid surfactant in the study sites.
The AeroFact device/drug combination delivered a surfactant dose calculated at 50% delivery efficiency, that is, 216 mg/kg surfactant was aerosolised to achieve calculated inhaled dose of 108 mg/kg (the standard dose for Alveofact instillation). The dose was determined based on bolus dose recommendations and estimation of the delivered surfactant dose using this aerosol generator (unpublished preclinical data, J. Fink). The AeroFact device was a prototype vibrating mesh nebuliser which generated an aerosol of <3 µm MMAD. The aerosol generation was synchronised with the beginning of the patient’s inspiration and continued through 50%–80% of the patient’s inspiratory time. The aerosol generator was housed in an interface placed between the nCPAP gas flow and the nCPAP nasal prongs.
Data collection included maternal history, demographics, AeroFact treatment and tolerance, incidence of nasal congestion requiring suctioning, indices of respiratory support, need for intubation and bolus surfactant, duration of mechanical ventilation, use of select medications, and other outcomes of prematurity until the time of discharge from the NICU. Infants were assessed for BPD at 36 weeks postmenstrual age. Infants who were clinically stable and requiring supplemental oxygen via nasal cannula at flow ≤2 L/min or receiving only FiO2 0.21 via nasal cannula at ≤4 L/min at 36 weeks underwent a room air challenge to determine if they could maintain their SpO2 ≥90%, as described by the current National Institutes of Health recommendations for assessing BPD.20
Statistical methods
Patient demographics, status at study initiation and outcome were summarised for all patients. Patients in parts 1 and 2 were compared with their respective historical controls. Continuous variables were summarised using number (n), mean and SD, and were analysed with unpaired, two-tailed Student’s t-test with Welsh’s correction. Categorical or qualitative characteristics were summarised by number (n), median and range, and were analysed by Fisher’s exact test, with Mann-Whitney test used for Apgar score. In addition, a Kaplan-Meier graph showed the age at which patients in part 2 met failure criteria and was analysed with Mantel-Cox log-rank test.
Results
The study was conducted between November 2017 and July 2018. Part 1 consisted of 10 patients who received a single AeroFact treatment and 30 matched historical controls. Part 2 consisted of 21 patients who could receive multiple AeroFact treatments and 63 controls.
Table 1 summarises the demographic and baseline characteristics of patients in parts 1 and 2. There were no significant differences between AeroFact-treated patients and their historical controls in either part 1 or part 2. Almost all AeroFact and historical control infants received antenatal steroids. Although not shown in table 1, there was no difference in race (>60% European ancestry in all groups) or ethnicity (no Hispanic/Latinx patient in any group).
Demographics and status at study entry
Table 2 shows the number of AeroFact treatments received by enrolled patients in parts 1 and 2. By design, 100% of patients in part 1 received a single treatment with AeroFact. In part 2, patients could receive up to four doses of AeroFact, although none received more than three doses. No patients received AeroFact or instilled surfactant beyond 72 hours of life. Table 2 also shows the short-term tolerance of AeroFact treatment.
AeroFact treatment and short-term tolerance of treatment
Table 3 shows the outcome of treated infants as well as their historical controls. Of those who met the predefined failure criteria, the majority had an increase in RSS to greater than 2.4. One historical control infant in part 1 also met the apnoea/bradycardia criteria, and one historical control infant in part 2 had respiratory acidosis. In part 2, there was a non-significant trend towards fewer AeroFact patients than historical controls meeting failure criteria (6 of 21 (29%) vs 30 of 63 (48%); p=0.20 by Fisher’s exact test).
Outcome of AeroFact-treated infants and matched historical controls
Three historical controls in part 1 and one historical control in part 2 were intubated and received surfactant before meeting failure criteria. One AeroFact patient in part 2 met failure criteria and was intubated after missing an indicated third AeroFact dose. These five patients were included in all analyses except in the Kaplan-Meier analysis of time to meet failure criteria.
There were no significant differences in any of the common complications of prematurity between the AeroFact-treated patients and their historical controls. In all groups 100% of patients received caffeine and none received vitamin A. The median NICU length of stay for patients in parts 1 and 2 (68 and 69 days) was comparable with that of historical controls (71 and 61 days). One patient in part 1 and one patient in part 2 died of late culture-proven neonatal sepsis, whereas there were no deaths in the historical control groups.
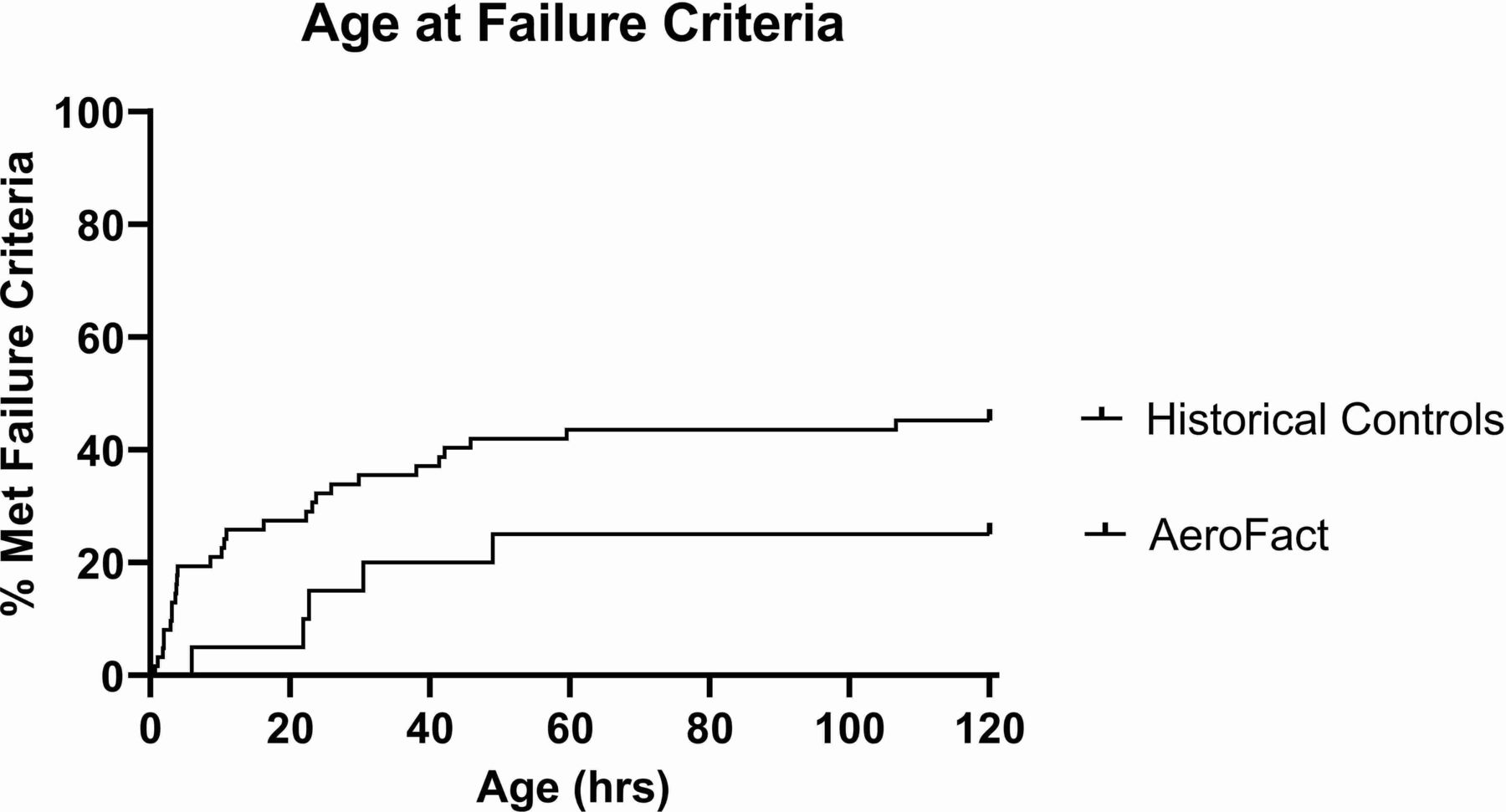
Figure 1 shows the Kaplan-Meier estimates of the time-to-failure analysis, comparing patients in part 2 with their historical controls. Although not statistically significant, the graph shows a trend (p=0.10) towards decreased rate of study failure criteria in the AeroFact patients than in historical controls.
{kind=link}
Kaplan-Meier plot of age at treatment failure for patients who received AeroFact treatment in part 2 compared with their historical controls. There was a trend of AeroFact patients being less likely to meet failure criteria (p=0.10 by Mantel-Cox log-rank test) than historical controls.
Discussion
AeroFact was well tolerated in infants 26 weeks through 30 weeks postmenstrual age with symptoms of RDS requiring nCPAP. No safety concerns were identified. Compared with controls, AeroFact-treated infants had non-significant trends towards less progression to treatment failure and reduced rates of instilled surfactant. There were no significant differences in the rates of key outcomes of prematurity between treated patients and historical controls. It is important to note that this was a small pilot trial, not powered to show significant improvement in AeroFact-treated infants. Our safety findings are consistent with other studies in preterm infants demonstrating the safety of aerosolised surfactants of both natural and synthetic origin.8–11 21–24
Other studies, using larger particles and continuous nebulisation, have shown variable responses to aerosolised surfactant. In a small pilot study, Sood et al 22 reported failure of aerosol surfactant in patients below 28 weeks. Minocchieri et al 21 reported a reduced risk of intubation and surfactant instillation in a subset of infants 32 weeks and 6 days through 33 weeks and 6 days gestation randomised to aerosol surfactant. However, their control group had an unexpectedly high intubation rate compared with data from a larger comparable population.25 Cummings et al 23 showed a decreased need for bolus surfactant in some infants treated with aerosolised surfactant compared with controls. More recently, Sood et al 24 showed a decreased need for bolus surfactant in infants treated with several methods of aerosolised surfactant compared with historical controls.
Compared with prior studies of aerosolised surfactant, AeroFact produces smaller aerosol droplets (<3 µm MMAD) in synchrony with inspiration, with higher output of undiluted surfactant (>0.3 mL/min) than conventional nebulisers.5 9–11 15 26 During in vitro testing, placement of the AeroFact system between nCPAP gas flow and the nasal interface with breath synchronisation produced an inhaled dose up to 50% of the nominal dose (preclinical data on file). The AeroFact device/drug combination of small particles, nebuliser placement and breath synchronisation may provide more efficient aerosol delivery to preterm infants than has been achieved with other surfactant aerosol device/drug combinations. If so, it may be an attractive alternative to other surfactant installation techniques that require intubation or installation of liquid surfactant via catheter.
The limitations of this pilot study include its small sample size, open-label design and use of historical controls. The study was designed to limit exposure of an investigational product, while generating feasibility and safety data to guide design of subsequent trials.
Conclusion
AeroFact is safe and well tolerated in this population of premature infants. Treatment with AeroFact may reduce the need for rescue therapy, including the need for intubation and treatment with instilled liquid surfactant. Future trials of AeroFact are planned.
Data availability statement
Data are available upon reasonable request. Data not included in the article text may be available for subsequent meta-analysis. Please contact the corresponding author for details.
Ethics statements
Patient consent for publication
Ethics approval
This study was approved by the Human Research Ethics Committee for both the Sydney South Eastern Local Health District and Mater Misericordiae, Brisbane.
References
Footnotes
Contributors LJ, KL, HGL and TS participated in the acquisition of patients and data, as well as revision and review of the paper. JF, JA and DD participated in the design of the study and analysis of data, as well as preparation, revision and review of the paper.
Funding This work was supported by Aerogen Pharma under clinical trial protocol APC-AF-CLN-001.
Competing interests At the time of the study, JF and JA were employed by Aerogen Pharma. DD is currently employed by Aerogen Pharma, but was not at the time of this study.
Provenance and peer review Not commissioned; externally peer reviewed.