Article Text

Abstract
Background Neonatal endotracheal intubation is often associated with physiological instability. The Neonatal Resuscitation Program recommends a time-based limit (30 s) for intubation attempts in the delivery room, but there are limited physiological data to support recommendations in the neonatal intensive care unit (NICU). We aimed to determine the time to desaturation after ceasing spontaneous or assisted breathing in preterm infants undergoing elective endotracheal intubation in the NICU.
Methods Observational study at The Royal Women’s Hospital, Melbourne. A secondary analysis was performed of video recordings of neonates ≤32 weeks’ postmenstrual age undergoing elective intubation. Infants received premedication including atropine, a sedative and muscle relaxant. Apnoeic oxygenation time (AOT) was defined as the time from the last positive pressure or spontaneous breath until desaturation (SpO2 <90%).
Results Seventy-eight infants were included. The median (IQR) gestational age at birth was 27 (26–29) weeks and birth weight 946 (773–1216) g. All but five neonates desaturated to SpO2 <90% (73/78, 94%). The median (IQR) AOT was 22 (14–32) s. The median (IQR) time from ceasing positive pressure ventilation to desaturation <80% was 35 (24–44) s and to desaturation <60% was 56 (42–68) s. No episodes of bradycardia were seen.
Conclusions This is the first study to report AOT in preterm infants. During intubation of preterm infants in the NICU, desaturation occurs quickly after cessation of positive pressure ventilation. These data are important for the development of clinical guidelines for neonatal intubation.
Trial registration number ACTRN12614000709640
- resuscitation
- neonatology
Data availability statement
All data relevant to the study are included in the article or uploaded as supplementary information. This was a secondary analysis of a randomised trial comparing two different facemask sizes used to deliver positive pressure ventilation to preterm infants prior to undergoing elective endotracheal intubation at The Royal Women’s Hospital (RWH), Melbourne, Australia. As part of this randomised trial, video recordings of the endotracheal intubations were collected. Data for this study Data were recorded in a paper-based Case Record From then entered into an electronic database (REDCap)
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
What is already known on this topic?
Neonatal intubation is often associated with physiological instability, and the duration of attempts may be longer than the maximum suggested in international guidelines.
The Neonatal Resuscitation Program recommends a time-based limit (30 s) for intubation attempts in the delivery room; however, there are limited physiological data to support recommendations after birth in the neonatal intensive care unit (NICU).
Apnoeic oxygenation time (AOT) is the time from the last positive pressure or spontaneous breath until desaturation (SpO2 <90%).
What this study adds?
This is the first study to report the time to desaturation after ceasing positive pressure or spontaneous breaths in preterm neonates undergoing intubation in the NICU.
AOT is substantially shorter in preterm infants compared with paediatric patients, and desaturation occurs quickly after ceasing assisted or spontaneous breaths.
Background
Neonatal endotracheal intubation is frequently associated with physiological instability.1 Adverse events, including bradycardia, fluctuations in blood pressure and severe desaturation, commonly occur during intubation attempts.1–4 Half of attempted intubations of preterm infants are associated with a fall in peripheral oxygen saturation (SpO2) levels of ≥20%.2 5 Adverse events often result in the termination of the intubation attempt, and are the most common reason for an unsuccessful intubation.6
The duration of intubation attempts varies with the experience of the operator and may be longer than the maximum suggested in international guidelines.7 In the delivery room (DR), the Neonatal Resuscitation Program (seventh edition, American Academy of Pediatrics, 2016) recommends that intubation attempts in neonates should be limited to 30 s or stopped when there is physiological instability (bradycardia, oxygen desaturation). However, there are no specific recommended heart rate (HR) or oxygen saturation (SpO2) thresholds at which the intubation attempt should be stopped, and there are limited physiological data to support time-based recommendations in the neonatal intensive care unit (NICU).8
Apnoeic oxygenation time (AOT) has been defined as the time from the last positive pressure or spontaneous breath until desaturation (SpO2 <90%). Desaturation occurs more rapidly in apnoeic children than in apnoeic adults receiving general anaesthesia.8 The increased instability of apnoeic children may be explained by a smaller functional residual capacity, greater metabolic demand and greater tendency for airway collapse compared with apnoeic adults.9 10 Kinouchi et al 11 studied the AOT in children aged 1 month to 12 years and concluded that SpO2 decreases to <95% more quickly in younger children compared with older children. Patel et al 12 measured the time until desaturation (SpO2 <90%) during apnoea in healthy children (2 days to 10 years) and showed that SpO2 declines more rapidly in infants and children (SpO2 <90% in 94–214 s) than in adolescents (SpO2 <90% in 364 s).
These observations suggest that the desirable duration for endotracheal intubation of newborn infants may be even shorter. To date, AOT has not been reported in preterm infants. The aim of this study was to describe the AOT of preterm infants undergoing elective endotracheal intubation in the NICU.
Methods
This was a secondary analysis of a randomised trial comparing two different facemask sizes used to deliver positive pressure ventilation (PPV) to preterm infants prior to undergoing elective endotracheal intubation at The Royal Women’s Hospital (RWH), Melbourne, Australia.13 As part of this randomised trial, video recordings of endotracheal intubations were collected. RWH is a tertiary perinatal centre with >7500 births per year. Eligible infants were those ≤32 weeks’ corrected gestation who required PPV before elective intubation in the NICU. Elective intubations were defined as those in which infants received sedation and muscle relaxation prior to the procedure. Infants with known facial or airway anomalies were excluded.
Infants were first administered continuous positive airway pressure via a facemask and a Neopuff Infant Resuscitator T-piece (Fisher & Paykel, Auckland, New Zealand). Any increase in positive end-expiratory pressure (PEEP) during PPV prior to intubation was at clinician discretion. Preoxygenation was not provided routinely, but infants did receive additional oxygen if hypoxaemic, to the unit-specific target (SpO2 91%–95%). All infants received sedation (fentanyl, 5 μg/kg) and muscle relaxation (suxamethonium, 2 mg/kg), along with atropine (20 μg/kg). Facemask ventilation was then administered using the Neopuff Infant Resuscitator T-piece. Intubation was performed by paediatric doctors (residents, registrars, fellows or consultants), supervised by a neonatal fellow or consultant. All intubations were performed using sterile, single-use, uniform internal diameter, plastic endotracheal tubes (Mallinckrodt Medical, Athlone, Ireland) under direct laryngoscopy. Only the first intubation attempt of each infant was included in the analysis and each infant was included only once.
Continuous SpO2 and HR data were recorded during the intubation attempt using a pulse oximeter (Masimo Radical 7; Masimo Corporation, Irvine, California, USA) and measurements of SpO2 and HR were recorded every 2 s during the apnoeic period. Infants were excluded if continuous pulse oximetry data (showing both HR and SpO2) were not available for the entire period of apnoea. Video recordings were made of all episodes of facemask PPV using an angled webcam (Logitech) and continued until successful endotracheal intubation.
Outcomes
The primary outcome measure was AOT, defined as the time from the last positive pressure inflation or spontaneous breath until desaturation (SpO2 <90%). This outcome was chosen to be consistent with other studies.12 14 15 Secondary outcomes included patient instability during the intubation attempt, as measured by the infant’s lowest HR, the lowest SpO2 during apnoea, desaturations (SpO2 <80% and SpO2 <70%) and severe hypoxaemia (SpO2 <60%).
Data collection
All video recordings were reviewed by a study investigator (RK) and the AOT was determined. A sample of 20 videos was independently reviewed by three study investigators (RK, EOC, KAH) to ensure consistency. Inconsistencies were resolved by group review. The duration of an intubation attempt was defined as the time from the last positive pressure inflation or last spontaneous breath until PPV recommenced (either via a T-piece with face mask or an endotracheal tube). Demographic data collected included gestational age (GA), birth weight, age and weight at intubation. Data were recorded on a paper-based Case Record Form and then entered into an electronic database (REDCap16).
Sample size and statistical analysis
This was a convenience sample of videos recorded in a randomised trial. Continuous data at each time point were analysed as mean (SD) if normally distributed, otherwise as median (IQR). SpO2 (median, IQR) was graphically represented. Kaplan-Meier survival curves were produced to determine the probability of desaturation.
Results
Videos of endotracheal intubation were available from 119 patients in the original randomised controlled trial. Forty-one infants were excluded because continuous SpO2 data for the apnoeic period were not available. The remaining 78 infants were included in the analysis (figure 1). Their median (IQR) GA at birth was 27 (26–29) weeks and birth weight 946 (773–1216) g. Median (IQR) age at intubation was 36 (10–312) hours. Baseline infant characteristics are presented in table 1.

Flow diagram of included patients.
Baseline characteristics
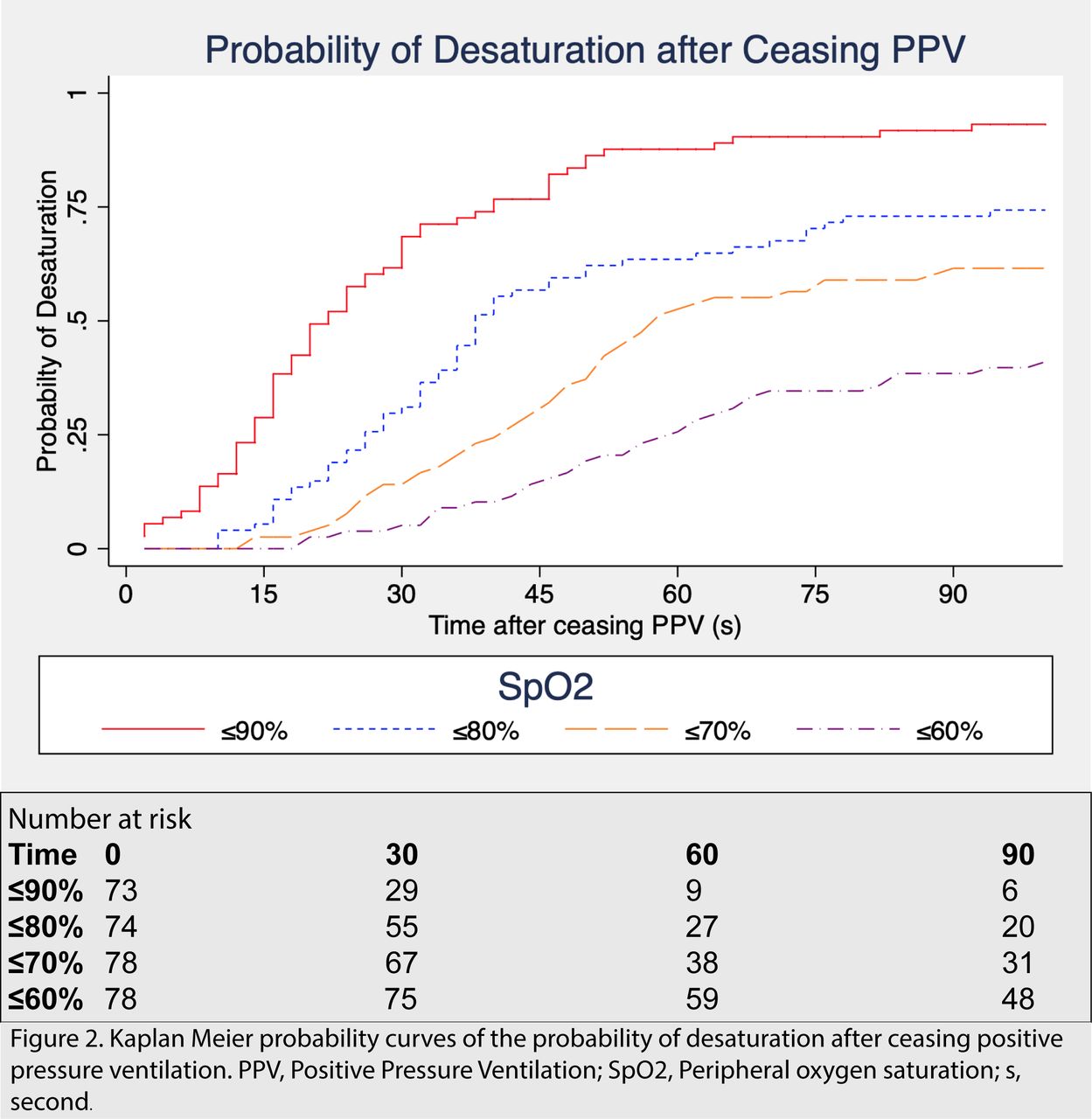
Residents/registrars (paediatric trainees) performed 62/78 (79%) intubation attempts, fellows (advanced neonatal trainees) 14/78 (18%) and consultants 2/78 (3%). Practitioners with <1 year experience performed 52/78 (67%) of attempts. The most common reasons for intubation were respiratory failure (58/78 (74%) infants), apnoea (13/78 (17%)) and elective endotracheal tube change (4/78 (5%)). All infants received PPV following muscle relaxation; therefore, the last positive pressure inflation marked the beginning of the apnoeic period in all infants. The maximum fraction of inspired oxygen (FiO2) before intubation was median (IQR) 0.81 (0.60–1.00) and maximum PEEP delivered via facemask was 6 (5–7) cm of water (cm H2O). All infants were intubated orally. All but five infants (73/78, 94%) desaturated to SpO2 <90% during the apnoeic period (figure 1). The median (IQR) AOT (time to SpO2 <90%) for these 73 infants was 22 (14–32) s. The median (IQR) time to SpO2 <80% (58/78 infants) was 35 (24–44) s, to SpO2 <70% (47/78 infants) was 46 (32–56) s and to SpO2 <60% (31/78 infants) was 56 (42–68) s (figure 2). No bradycardia (HR <100 bpm) was observed in any infant. The median (IQR) lowest SpO2 during the apnoeic period was 84% (70%–95%).

Kaplan-Meier probability curves of the probability of desaturation after ceasing PPV. PPV, positive pressure ventilation; SpO2, peripheral oxygen saturation; s, second.
Figure 3 shows the median and IQR of the peripheral oxygen saturation at each second after ceasing PPV.

{kind=link}
{kind=link}
{kind=link}
Change in peripheral oxygen saturation after ceasing PPV in premature infants undergoing elective intubation. PPV ceased at time 0. PPV, positive pressure ventilation; SpO2, peripheral oxygen saturation.
Discussion
To our knowledge, this is the first study to report AOT in preterm infants and to characterise the changes in SpO2 and HR after ceasing PPV in preterm infants undergoing endotracheal intubation. AOT is shorter in preterm infants than that reported in older children and adults.
It is increasingly recognised that neonatal endotracheal intubation may be technically challenging, and clinical instability is common. The National Emergency Airway Registry for Neonates (NEAR4NEOS) recently reported a severe desaturation rate (≥20% decrease from baseline) of 48%.2 Adverse events were common during neonatal intubation, even in the relatively controlled setting of the NICU.2 Adverse events are the most common cause of an intubation attempt being stopped in neonates.17 This results in some infants being exposed to multiple intubation attempts before the endotracheal tube is successfully placed.3 With an increasing number of intubation attempts, there is an increase in important complications including cardiac arrest, laryngospasm and air leak (pneumothorax and/or pneumomediastinum).18
Neonatal intubation is a mandatory skill for neonatal trainees, but one that is increasingly difficult to master and maintain, possibly due to increasing use of non-invasive ventilation and less-invasive surfactant administration techniques.19 To date, very little evidence is available to guide the optimal duration of an intubation attempt. Even when practitioners with considerable experience attempt intubation, many preterm infants are not intubated within the 30 s limit suggested by the Neonatal Resuscitation Program.7 17 This guideline does not distinguish between term and preterm infants. To our knowledge, no previous studies have reported the AOT in preterm infants. Our data allows physiological targets to be correlated with time during intubation attempts. This study showed that the average AOT in preterm infants (time to desaturation <90%) was about 25 s.
Similar to other studies,2 3 5 20 we found a high rate of physiological instability in preterm infants during endotracheal intubation. The AOT in this trial was significantly shorter than values previously published by Patel and colleagues,12 reflecting the clinical impression that preterm infants become desaturated more rapidly than older infants and children. In contrast to older infants and children, preoxygenation is not universally applied in the neonatal population, due to concerns regarding potential adverse effects of hyperoxia, particularly in very preterm infants.
Previous studies have demonstrated that premedication before endotracheal intubation increases the speed of intubation and reduces the likelihood of associated adverse sequelae in infants.4 21–23 Krick et al 24 showed that premedication with a muscle relaxant was associated with fewer intubation attempts, fewer adverse events and less bradycardia. In our study, the average HR decreased after ceasing PPV, but changes were minimal and not clinically important. There was no bradycardia, despite the observed severe desaturations, which might be explained by the routine administration of atropine.
Our study has several strengths. It provides insight into an important but underinvestigated issue in neonatal medicine. The detailed data collection enables an accurate measurement of AOT in neonates. We also acknowledge some limitations to our study. Some eligible neonates were not included in the analyses due to missing data. The accuracy of pulse oximeter data may not be maintained below lower saturation thresholds (eg, SpO2 <70%).
This single site study was performed in a large perinatal centre and may not be generalisable to other settings, or to the DR, or to patients being intubated without premedication. There was a range of operator experience that may have influenced intubation success rates and therefore AOT. Furthermore, only very preterm infants undergoing elective endotracheal intubation in the neonatal unit were included; these data are not generalisable to apnoeic infants undergoing intubation in the DR, where functional residual capacity may not yet have been established.
In paediatric and adult populations, routine preoxygenation using 100% oxygen prior to endotracheal intubation may mitigate the risk of desaturation during the procedure.25 In neonates, the balance of potential adverse effects from hyperoxia and hypoxia should be considered. In line with local practice, infants in this study were not routinely preoxygenated, which may have influenced the time to desaturation.
Improving neonatal intubation safety requires consideration of multiple factors. This study was not powered to describe correlation between SpO2 or HR thresholds and clinical outcomes, but our data suggest that physiological stability criteria may be more appropriate than time-based criteria for intubation attempts. For some infants, especially if premedicated, this would allow for a more prolonged attempt, which might improve intubation success and reduce adverse events due to repeated intubation attempts. A randomised controlled trial showed that continuous delivery of transnasal high-flow humidified oxygen during apnoea significantly prolonged the AOT in older infants and children with healthy lungs.9 This is a topic that needs further research and is currently being studied in the neonatal population.26 Further research should also focus on other variables that may influence AOT in preterm infants, particularly the baseline clinical condition including preoxygenation, medications administered and physiological stability prior to the intubation attempt.
Conclusion
To our knowledge, this is the first study to report AOT in preterm infants. Desaturation occurs quickly after cessation of PPV and therefore the AOT is substantially shorter in preterm infants compared with paediatric patients. These data provide important clinical information for the development of clinical guidelines and studies to improve the safety of neonatal intubation.
Data availability statement
All data relevant to the study are included in the article or uploaded as supplementary information. This was a secondary analysis of a randomised trial comparing two different facemask sizes used to deliver positive pressure ventilation to preterm infants prior to undergoing elective endotracheal intubation at The Royal Women’s Hospital (RWH), Melbourne, Australia. As part of this randomised trial, video recordings of the endotracheal intubations were collected. Data for this study Data were recorded in a paper-based Case Record From then entered into an electronic database (REDCap)
Ethics statements
Patient consent for publication
Ethics approval
The Royal Women’s Hospital Research and Ethics Department approved the project in accordance with National Health and Medical Research Council guidelines (approval number 14/04) and the original trial was prospectively registered with the Australian New Zealand Clinical Trials Registry.
References
Footnotes
Contributors RK was responsible for collection of data, analysis of data, drafting the manuscript and revising the final manuscript. EOC conceptualised and designed this current secondary analysis. KAH and EOC assisted with data collection. RK, KAH, BJM, MT, PGD and EOC participated in analysis and interpretation of data and revising of the manuscript. All authors approved the final version of the manuscript.
Funding National Health and Medical Research Council Centre for Research Excellence in Newborn Care (#1153176) and National Health and Medical Research Council Program Grant (#1113902).
Disclaimer The views expressed in the article are the authors own and are not an official position of the institution or funder. The authors have no financial relationships relevant to this article to disclose.
Competing interests None declared.
Provenance and peer review Not commissioned; externally peer reviewed.
Linked Articles
- Fantoms