Article Text

Statistics from Altmetric.com
Although considerable effort has been invested in the development of screening programmes to detect congenital heart disease before and after birth, a large proportion of infants with congenital heart defects remain undetected by these programmes and come to the attention of the medical profession only after they develop symptoms.1 These symptomatic infants can present in extremis and die rapidly. A study of 1590 babies with congenital heart disease who presented in the northern region of the United Kingdom was published in this journal in 1999: one in 10 presented with cardiac symptoms before the first neonatal screening examination and more than half were considered to have a normal cardiovascular system at this examination.1 Of these, almost 40% presented with symptoms or died before the routine 6 week check. These observations are consistent with data from abroad, including the large Baltimore-Washington Study, in which it was observed that, of all infants with cardiovascular malformations who died in the first week of life, one in four did not have the cardiovascular malformation identified before death.2 It is likely that, with the trend towards earlier discharge of apparently well neonates, these numbers may increase in the future, rather than decrease.
Advances in surgical technique have substantially reduced the perioperative mortality for neonates with congenital heart lesions. In the best centres, the in hospital mortality for patients who undergo the arterial switch operation for simple complete transposition of the great arteries now approaches 1%.3 As a result of these advances, death before surgery is becoming proportionally of greater significance: in a recent series reported from Toronto, 4% of neonates presenting with simple transposition died before surgery.4
It thus appears that for certain lesions, an era is approaching when the time of greatest hazard to the infant is not while under the surgeon's knife or in the intensive care unit after surgery, but before actually being admitted to the specialist centre. The recent “Framework for the future” document emphasised the importance of efficient stabilisation of the sick child in the local hospital while awaiting transfer to a lead centre.5 This article will address some of the principles on which resuscitation and stabilisation of the symptomatic neonate with congenital heart disease may be based.
Use of prostaglandin
WHO SHOULD BE GIVEN PROSTAGLANDIN?
Most textbooks of paediatric cardiology contain comprehensive lists of the types of lesion that may warrant prostaglandin infusion. Although these lists are diagnosis based, a full sequential diagnosis will rarely be available during the initial phase of the resuscitation, so that the decision has to be based on clinical findings. A study that applied information theory6 to this decision making process concluded the following.
- (1)
- The risk of withholding prostaglandin infusion in a patient with a prostaglandin sensitive lesion will depend on the patient's clinical condition. Thus, although a relatively well patient with a prostaglandin sensitive lesion may well survive a transport without prostaglandin, it is unlikely that a patient in extremis will. As a result, the threshold for starting prostaglandin should be lower in the latter group.
- (2)
- The most useful clinical finding to discriminate patients with potentially prostaglandin sensitive lesions is the presence of cyanosis. In the cyanosed neonate, the probability of a prostaglandin sensitive lesion is increased by the presence of a murmur, whereas in a non-cyanosed patient, it is increased by the presence of abnormal pulses.
- (3)
- Using the combination of signs (cyanosis, a murmur, or abnormal pulses), in association with the general condition of the patient, the study concluded that, in an infant in extremis, the presence of cyanosis or abnormal pulses alone was associated with a sufficient probability of a prostaglandin sensitive lesion to indicate prostaglandin infusion. In the cyanosed infant, without a murmur and in whom the peripheral pulses were normal, although this point may be debated, it may be appropriate to withhold prostaglandin infusion for transfer, if the child is otherwise well.
THE CRITICALLY ILL NEONATE WITH CONGENITAL HEART DISEASE WHO IS UNRESPONSIVE TO PROSTAGLANDIN
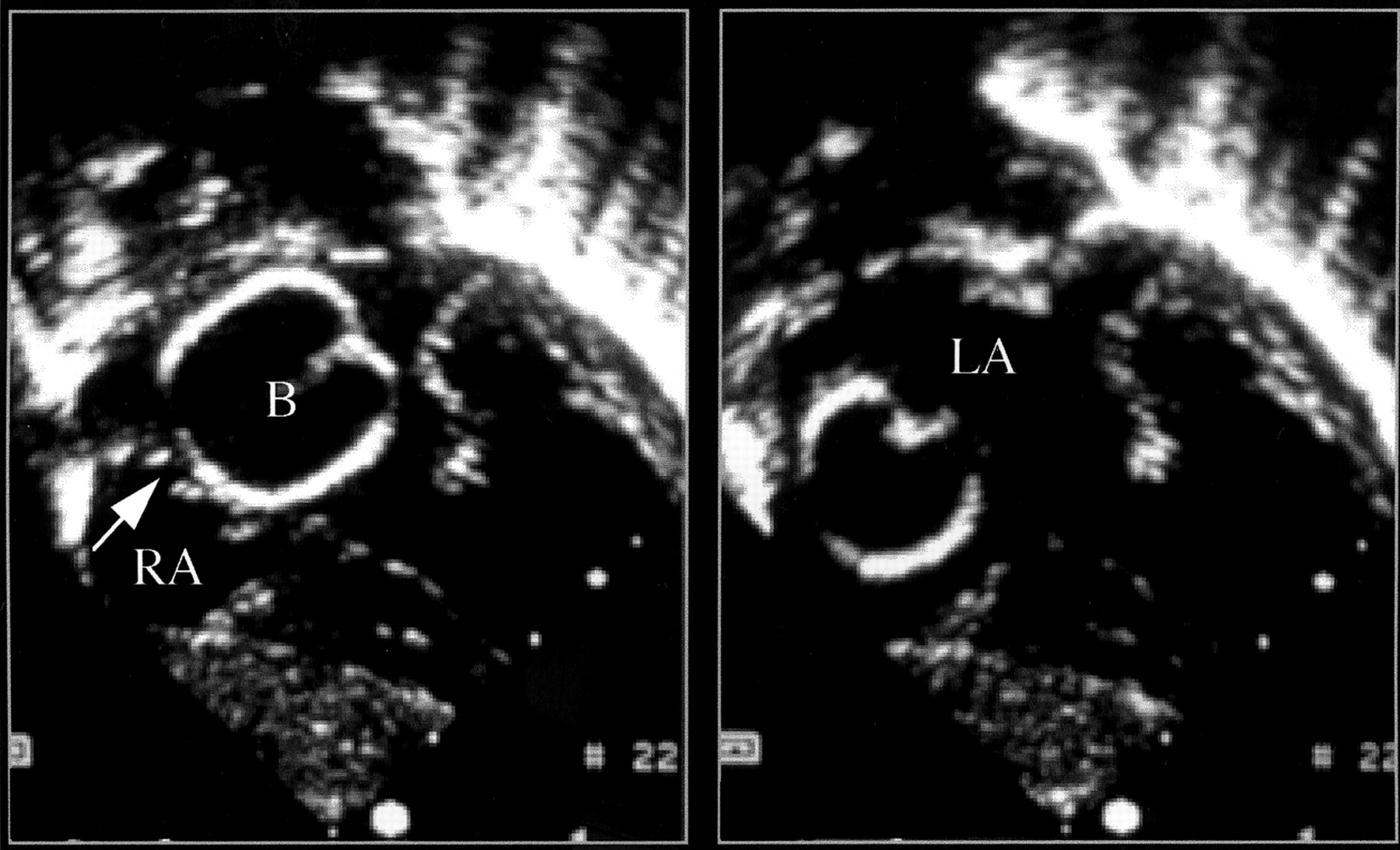
Although there are no congenital cardiac lesions for which prostaglandin is contraindicated as such, not all cyanosed neonates respond to prostaglandin. The most commonly seen example of this is obstructed total anomalous pulmonary venous drainage, for which, at best, the agent will reduce the pulmonary vascular resistance but, by increasing pulmonary blood flow, may exacerbate the venous congestion because of obstructed return. Another example is transposition of the great arteries with intact ventricular septum and an intact or restrictive atrial septum, when emergency atrial septostomy (fig 1) is the only measure that will keep these patients alive.
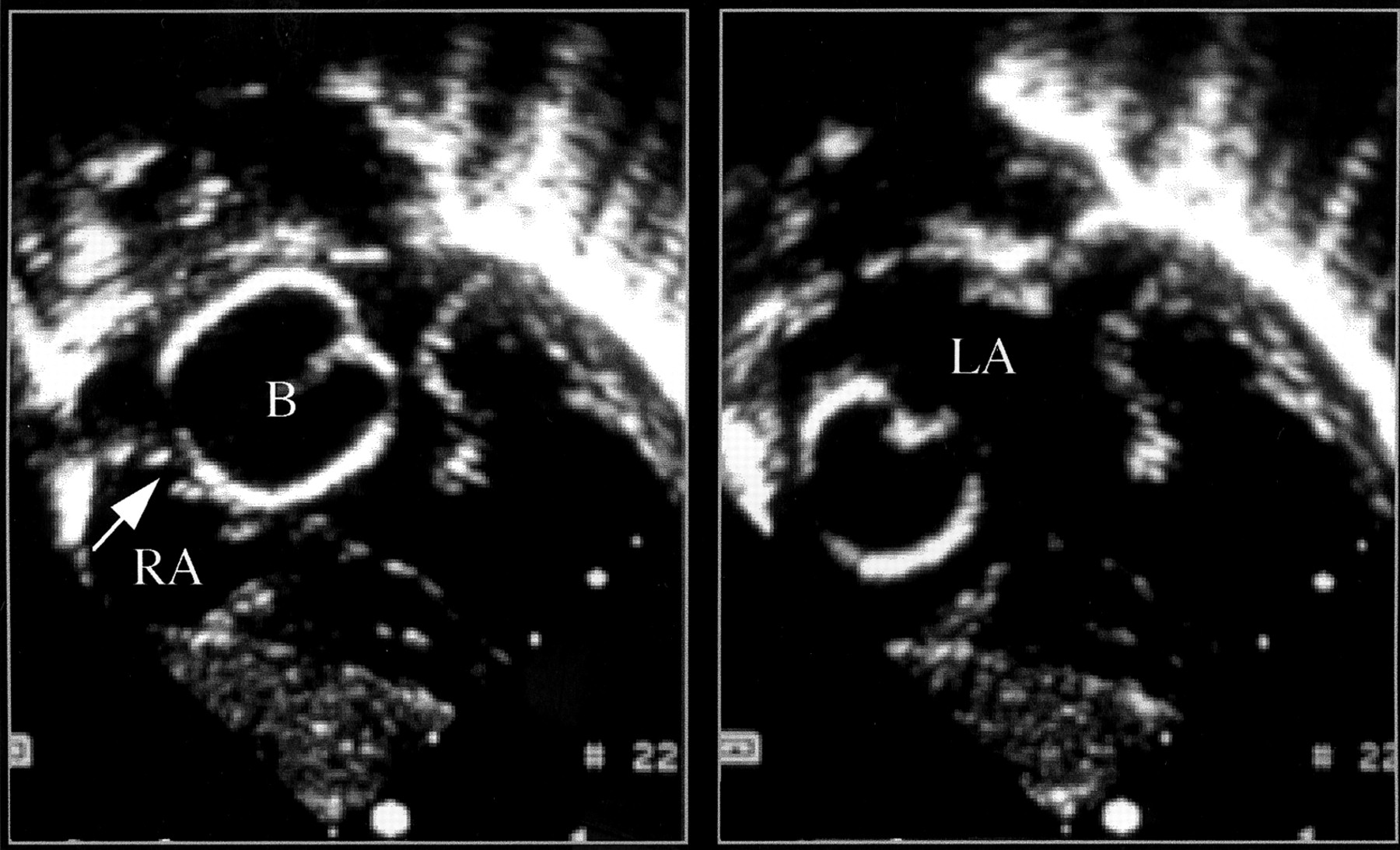
Balloon atrial septostomy in a neonate with transposition of the great arteries. The septostomy catheter has been inserted into the umbilical vein, and has been passed from the right atrium (RA) across the foramen ovale (arrow). After inflation of the balloon (B) in the left atrium (LA), the catheter is pulled back across the atrial septum, thus enlarging the interatrial communication.
Differential diagnosis of congenital heart lesions: common diagnostic challenges
DIFFERENTIATING A CRITICALLY OBSTRUCTED SYSTEMIC CIRCULATION FROM SEVERE SEPSIS
Most neonates who are referred to a specialist cardiac centre will have been empirically started on antibiotics before transfer. The clinical distinction between an obstructed systemic circulation—for example, coarctation of the aorta, critical aortic stenosis, hypoplastic left heart syndrome—and severe sepsis remains extremely difficult, as the incidence of the two is about the same. A study that assessed the use of clinical findings to distinguish these two entities suggested that most of the available clinical variables, either alone or in combination, had insufficient sensitivity to provide an accurate differentiation.7 In this study, although a murmur or weak pulses occurred commonly in infants with an obstructed systemic circulation, 22 of the 47 patients with this type of cardiac lesion did not have a cardiac murmur at presentation.7 Furthermore, it would be fair to say that a sick neonate with systemic sepsis may have reduced peripheral pulses secondary to a low cardiac output. It may be considered therefore that, given the insensitivity of clinical examination, on site echocardiography should be available.
ARRHYTHMIA
In all neonates with suspected congenital heart disease, 12 lead electrocardiography (ECG) should routinely be performed. Arrhythmias, for example congenital complete heart block or tachyarrhythmias, can be caused by congenital heart disease8 (Ebsteins malformation, congenitally corrected transposition of the great arteries, etc) or intracardiac tumours,9 but can also occur in the neonate with a structurally normal heart.8The key features to establish when examining a neonatal ECG are that there is a regular narrow QRS complex, with a rate of 100–150, each complex being preceded by a P wave, which is upright in lead I and aVF. Of course, these guidelines are not absolute, as sinus rates exceeding these levels may be encountered in the sick neonate.
Neonatal bradyarrhythmia or tachyarrhythmia can present with shock, with clinical signs and symptoms similar to those of a critically obstructed systemic circulation. One potential clinical manifestation of longstanding (in other words in utero) arrhythmias may be the presence of hydrops,10 ,11 which carries with it a poor prognosis.11 All neonates with an arrhythmia require echocardiography to exclude associated intracardiac defects, but prompt diagnosis and treatment of a tachyarrhythmia can often rapidly reverse a spiralling clinical situation, and should not be delayed. A diagnosis of complete heart block in the neonate with a low cardiac output should prompt the neonatologist to seek early advice from a paediatric cardiologist, as medical treatment—for example, isoprenaline—and urgent transfer for insertion of a pacemaker may be necessary.10
DIFFERENTIATING CRITICALLY OBSTRUCTED PULMONARY CIRCULATION OR OBSTRUCTED PULMONARY VENOUS DRAINAGE FROM PERSISTENT PULMONARY HYPERTENSION
The clinical distinction between persistent pulmonary hypertension and a duct dependent pulmonary circulation can be extremely challenging without echocardiography. This is especially difficult in the term neonate with persistent fetal circulation (PFC) without parenchymal lung disease. Indeed cyanotic congenital heart disease “masquerading as PFC” was diagnosed in 9% of neonates after institution of extracorporeal membrane oxygenation (ECMO) support for treatment of apparent intractable hypoxic respiratory failure.12Infants with PFC may well fail a nitrogen washout test because of right to left shunting at the intracardiac and ductal levels, and early radiological examination is often of little help because the lung fields in both settings will be oligaemic, albeit for completely different reasons.
A prostaglandin infusion may provide a useful “diagnostic test” in this situation, normally resulting in considerable improvement in the infant with duct dependent congenital heart disease. However, its beneficial effects on the pulmonary vascular resistance may also lead to improved oxygenation with prostaglandin treatment in patients with PFC. The algorithm for treating PFC will often include a trial of inhaled nitric oxide; this is unlikely to provide much benefit to the patient with congenital heart disease, unless, of course, this coexists with a degree of transient pulmonary hypertension! In summary, if there remains any doubt as to the causes of persistent cyanosis in the neonate in whom CO2 clearance is relatively easy to achieve, with radiologically normal (or oligaemic) lungs, early echocardiography should be sought.
DIFFERENTIATING CONGENITAL HEART DISEASE FROM PARENCHYMAL LUNG DISEASE
An important lesion that can masquerade as “parenchymal” lung disease with persistent pulmonary hypertension is obstructed total anomalous pulmonary venous drainage (TAPVD). Again, this is quite often diagnosed echocardiographically at the stage when neonates with “respiratory failure” present for ECMO support.12Infants presenting with obstructed TAPVD often have an unremarkable clinical cardiovascular examination. Textbooks describe the traditional cottage loaf or snowman radiographic appearance in obstructed TAPVD; however, radiographs of these infants are often obtained as an emergency measure in suboptimal conditions. In practice, TAPVD is often clinically and radiologically indistinguishable from diseases of the lung parenchyma, such as pneumonia, meconium aspiration, and early emphysema (fig 2), and in this situation early echocardiography should be considered to either make or exclude the diagnosis.

{kind=link}
{kind=link}
Chest radiograph of a hypoxic infant referred on the first day of life for extracorporeal membrane oxygenation support with a presumed diagnosis of persistent pulmonary hypertension secondary to meconium aspiration. Cardiac echocardiography showed an obstructed infradiaphragmatic total anomalous pulmonary venous connection.
In short, unless there is a clear cut cause for parenchymal lung disease, or indeed an appropriate response to conventional therapeutic manoeuvres, the diagnostic test required to make this distinction remains echocardiography.
“BALANCING THE CIRCULATIONS” IN THE INFANT WITH CRITICALLY OBSTRUCTED SYSTEMIC CIRCULATION
These infants most commonly present with clinical signs of systemic hypoperfusion, with acidosis and hypotension, and often with signs of end organ impairment. Peripheral pulses are often globally reduced; if there is obstruction within the aortic arch, the femoral pulses will be weaker than the right brachial pulse, or indeed may be absent. In these infants, resuscitation should aim to optimise systemic oxygen delivery and prevent metabolic acidosis, which can be the cause of increased operative mortality.13
Two fundamental principles underlie the resuscitation of these infants. Firstly, ductal patency (to provide systemic blood flow) is vital for early survival; thus all patients in whom this diagnosis is suspected should be started on prostaglandin infusion at a rate appropriate to maintain ductal patency. Apnoea secondary to prostaglandin infusion is a relatively common indication for intubation in these patients, but not necessarily an indication to reduce the dose and never an indication to stop the infusion. Secondly, when ductal patency has been established, attention must be directed to the balance between the systemic and pulmonary blood flows. In these patients, the systemic, myocardial, and pulmonary circulations are in parallel and in constant dynamic competition with one another. In short, increases in pulmonary blood flow lead to reductions in systemic and myocardial blood flow,14 ,15 with continuing signs of poor peripheral perfusion, metabolic acidosis, oliguria, and myocardial dysfunction. Pulmonary overcirculation should be pre-emptively managed by using measures that restrict pulmonary blood flow, in order to allow adequate perfusion of the systemic and myocardial vascular beds. In summary:
- (1)
- Prostaglandin infusion must be started at a rate sufficient to maintain ductal patency.
- (2)
- Ventilatory parameters should be adjusted to manipulate the pulmonary vascular resistance to avoid pulmonary overcirculation, so as to maintain a pulmonary to systemic blood flow ratio of about 1:1. This goal can usually be achieved by applying a modest level of positive end expiratory pressure (4–6 cm H2O), ventilating in room air in the first instance, and adjusting inspiratory pressures, rate, or tidal volumes to achieve an arterial CO2 tension of 5–6 kPa and a systemic saturation of 75–85%, avoiding respiratory alkalosis.
- (3)
- If signs of low cardiac output persist, the patient should be reassessed to ensure that the prostaglandin infusion is adequate and intravascular volume is satisfactory, and anaemia should be corrected. If the systemic blood pressure allows, a low dose nitroprusside infusion may improve metabolic acidosis. Otherwise, a low dose inotrope infusion may be of benefit in arresting the vicious cycle of metabolic acidosis and worsening ventricular function. In general, high dose inotrope infusions should be avoided because they may increase systemic vascular resistance, thus forcing more blood into the lungs and worsening the pulmonary to systemic blood flow distribution.
The patient after in utero diagnosis of congenital heart disease
It was hoped that the antenatal diagnosis of congenital heart defects would reduce subsequent mortality by ensuring early intervention in affected infants, in some cases before the onset of symptoms that would otherwise accompany ductal closure. Interestingly, most large screening studies suggest that this ambition has not been realised.16 A study from the United States suggests that delivery at a tertiary care centre does not improve SNAP scores (score for neonatal acute physiology) of infants with major structural heart defects,17 and a study from the United Kingdom indicates that overall survival for infants with hypoplastic left heart syndrome is similar after in utero and ex utero diagnosis.18Similarly, there are few data to support improved outcome after delivery of these infants in a specialist centre; indeed it has been suggested that prenatally diagnosed cardiac disease can be safely delivered outside regional cardiac centres.19 However, when one takes into account factors such as local expertise and transport facilities, one could still speculate that, for some infants with duct dependent circulations, expert anticipatory management in tertiary centres may still be preferable.
Although in general it appears that antenatal diagnosis and in utero transfer have not had the impact on neonatal mortality that had been predicted, for certain lesions, particularly transposition of the great arteries, antenatal diagnosis may reduce mortality and, at least in some, be an indication for in utero transfer.20 A particular consideration in these patients is the status of the atrial septum, which in some cases can be virtually intact; this prevents mixing and may be associated with death within the first few hours of life, unless emergency balloon atrial septostomy is performed.4 We consider therefore that the detection of transposition in utero is one of the few definite indications for delivery at a specialist centre, particularly if it is expected that the atrial septum may be restrictive.
Transport of the neonate with congenital heart disease
In general, postnatal transport of the neonate with congenital heart disease follows similar guidelines to transport of all critically ill neonates, and ideally should take place when the infant has been sufficiently stabilised.
The key to optimal management of these patients is to establish early communication with a specialist cardiac centre. The timing of transfer to a cardiac centre is determined by the diagnosis, which in turn guides timing of cardiological or surgical intervention. An important factor that relates in part to the underlying diagnosis and equally to the early management of the infant is its clinical condition. Often the infant with a duct dependent lesion will improve greatly once ductal patency has been achieved with prostaglandin infusion. This improvement can be fairly rapid in the cyanosed infant with critical pulmonary stenosis and a duct dependent pulmonary circulation, and in the non-cyanosed neonate with a coarctation and duct dependent systemic circulation. If a desirable response to prostaglandin has occurred and airway stability and vascular access have been appropriately secured, transport to a cardiac centre need not necessarily be an out of hours emergency. Indeed, transfer may be better carried out at times when medical and nursing staff with appropriate levels of skill are available to safely undertake this.
However, often, despite appropriate resuscitative measures, clinical improvement and stability are not achieved. Assuming that prostaglandin and not prostacyclin is being infused and that venous access is adequate, this can be because of inadequate ductal flow in a duct dependent situation or ventricular dysfunction in a patient with obstructed systemic ventricular outflow or because a patient has been profoundly shocked and acidotic for a period of time. Finally, as mentioned above, prostaglandin infusion will make little clinical difference to the cyanosed infant with transposition and a restrictive atrial septum or the neonate with obstructed TAPVD. Thus, despite every effort, “stabilisation” may not be possible in all cases. Early recognition of a failure to respond to resuscitative procedures should stimulate prompt transfer to a cardiac unit.
There is no specific algorithm as to which neonates should be intubated before transfer and which can be safely left self ventilating. Often, the decision has been made by alternative mechanisms: many cyanosed neonates will have already been intubated because of a lack of response to less invasive modes of oxygen delivery. However, in a cyanosed neonate who is neither acidotic nor in respiratory distress, a nitrogen washout test can be performed without intubation. If as a result of this the diagnosis is cyanotic congenital heart disease, prostaglandin can be infused peripherally and the infant observed for a period of time. Prostaglandin induced apnoeas are not an indication for dose reduction (assuming that the infusion rate is correct), but are usually an indication for intubation, as airway security is essential both before and during transport. Other neonates with congenital heart disease who may require intubation are those who present in a shocked state, typically those with a duct dependent systemic circulation. In our opinion, continuing metabolic acidosis, which is often associated with tachypnoea in an attempt to compensate for this, and poor systemic perfusion would be an indication for mechanical ventilation in these infants.
Mechanical ventilation should aim to optimise systemic and pulmonary flows, as described above. Intravenous sedation (morphine infusion) is usually necessary; muscle relaxants should be considered for the shocked neonate who remains tachypnoeic. Where appropriate, an “ambu-bag” should be available for hand ventilation to avoid administration of additional oxygen when it may be detrimental.
Neonatal echocardiography
It has recently been suggested that echocardiography “should not be limited to cardiologists in the diagnosis and assessment of congenital heart disease, but should be extended to the routine care of critically ill neonates . . . Paediatric cardiologists should not be worried about neonatologists learning echocardiography, rather they should encourage, support and supervise them.”21 The recent development of telemedicine technology has greatly increased the utility of on site echocardiography in many centres in this country and abroad. In one study, 133 neonatal echocardiograms were transmitted 400 miles from North Dakota to Rochester Minnesota.22 Of these, 132 were performed for “urgent indications”. Transmitted echocardiograms provided adequate diagnostic information in all. For 79 neonates there was a change in medical management or cardiology follow up. An immediate change in management of 32 patients (24%) occurred on the basis of the echocardiogram, including seven for whom emergency transfer was either arranged or avoided. In a series from Belfast, the transmitted echocardiograms were of sufficient quality to make a reliable diagnosis in 62 of 63 patients aged between 1 and 42 days. In 74%, the need to transfer the babies to obtain a diagnosis was avoided.23 The idea that neonatal echocardiography should not be restricted to the cardiologist should be embraced whole heartedly.
Conclusion
In the current era, technology, resources, and distribution of expertise do not generally allow access to rapid postnatal diagnosis in symptomatic neonates with suspected congenital heart disease. Furthermore, although availability of, and training in, prenatal diagnosis of congenital heart disease is improving, national antenatal detection rates for congenital heart disease are probably no more than 25% (with considerable lesion specific and geographic variation).24 Most cases of congenital cardiac abnormalities are therefore unexpected. We must therefore have a high index of suspicion for including congenital heart disease (or arrhythmia) in the differential diagnosis for a cyanosed neonate or one who becomes shocked in the first minutes, hours, or days of extrauterine life. Early discussion with a cardiac centre and institution of appropriate treatment in suspected cases may avoid the pursuit of other less likely diagnoses, the treatments for which may worsen the clinical situation.
References
1st Asia Pacific Forum on Quality Improvement in Health Care Three day conference Wednesday 19 to Friday 21 September 2001 Sydney, Australia
We are delighted to announce this forthcoming conference in Sydney. Authors are invited to submit papers (call for papers closes on Friday 6 April), and delegate enquiries are welcome.
The themes of the Forum are:
Improving patient safety
Leadership for improvement
Consumers driving change
Building capacity for change: measurement, education and human resources
The context: incentives and barriers for change
Improving health systems
The evidence and scientific basis for quality improvement.
Presented to you by the BMJ Publishing Group (London, UK) and Institute for Healthcare Improvement (Boston, USA), with the support of the the Commonwealth Department of Health and Aged Care (Australia), Safety and Quality Council (Australia), NSW Health (Australia), and Ministry of Health (New Zealand).
For more information contact: quality{at}bma.org.ukor fax +44 (0)20 7383 6869