Article Text

Abstract
BACKGROUND Non-invasive assessment of inflammation is likely to be useful in the management of cystic fibrosis (CF). Exhaled carbon monoxide (CO) concentrations are increased in patients with clinically stable CF. A study was undertaken to determine whether this marker of oxidative damage is further increased during exacerbations of the disease.
METHODS Exhaled CO concentrations were measured in 12 healthy non-smoking control subjects (six men) of mean (SE) age 37 (2) years with forced expiratory volume in one second (FEV1) 95 (1)% predicted and in 44 patients with CF (20 men) of mean (SE) age 29 (1) years with FEV1 56 (3)% predicted using an on-line CO analyser.
RESULTS Twenty nine patients were in a stable condition while 15 had clinically defined respiratory exacerbations (increased cough and production of sputum, change in the quality of the sputum, shortness of breath, sensation of chest congestion, and deterioration of FEV1) and represented the unstable group. Exhaled CO concentrations were 2.0 (0.15) ppm in the control group, were increased in the stable CF group to 2.7 (0.13) ppm (differences between means –0.67 (0.22), 95% confidence interval (CI) 0.22 to 1.12, p<0.01) and further increased in the unstable group to 4.8 (0.3) ppm (differences between means –2.15 (0.32), 95% CI 1.50 to 2.79, p<0.001). A significant correlation was found between the deterioration in FEV1 and exhaled CO concentrations.
CONCLUSIONS This study shows that the measurement of exhaled CO is of potential value as an indicator of exacerbations in patients with CF and could be used as a simple method to monitor the course of the disease.
- carbon monoxide
- nitric oxide
- cystic fibrosis
- exhaled gases
Statistics from Altmetric.com
In patients with cystic fibrosis (CF) increased concentrations of markers of oxidative damage to lipids and proteins and lower concentrations of antioxidants in the plasma suggest increased oxidative stress.1 ,2 There is also evidence for increased oxidative stress in the epithelial lining fluid of patients with CF.3 ,4 These oxidants activate heme oxygenase-1 (HO-1), an enzyme that catalyses the initial reaction in heme catabolism leading to the production of biliverdin, iron, and carbon monoxide (CO).5 Exhaled CO concentrations are increased in asthma,6 upper respiratory tract infections,7and bronchiectasis,8 indicating increased oxidative stress in these inflammatory conditions. We have recently reported an increase in exhaled CO concentrations in patients with CF.9
Nitric oxide (NO) is synthesised in the airways by NO synthase (NOS)10 and is rapidly metabolised to nitrite (NO2) and nitrate (NO3). Exhaled NO concentrations are raised in inflammatory airway diseases,11-13 as well as sputum concentrations of NO2 and NO3.14 Surprisingly, exhaled NO concentrations are not increased in patients with CF15 ,16 and the possible explanations for this finding include poor diffusion of NO across thick and viscous airway secretions, failure of upregulation of epithelial inducible NOS (iNOS),17 ,18 and reaction of NO with superoxide to form peroxynitrite, nitrite, and nitrate.19 In agreement with the latter hypothesis, Ho et al reported increased levels of nitrite in breath condensate from patients with CF.20 There was no difference in sputum concentrations of nitrite or nitrate between CF patients with stable disease and patients with pulmonary exacerbations,21 whereas increased sputum concentrations of total nitrite plus nitrate have been reported in acute pulmonary infections in patients with CF.22
In order to find a reliable marker of respiratory exacerbations other than NO or its metabolites in patients with CF we hypothesised that HO-1 activity may be increased in response to inflammation and oxidative stress in CF patients who had infective exacerbations, resulting in increased exhaled CO concentrations.
Methods
SUBJECTS
Twelve healthy non-smoking subjects were included in the normal control group. They were free of respiratory disease, with no upper or lower airway infection within the last four weeks, and presented with normal spirometric values. Forty four patients with a diagnosis of cystic fibrosis from the CF Clinic of the Royal Brompton Hospital were evaluated for the patient group. Patients with a severe exacerbation, asthma, upper respiratory tract infection within the last four weeks, cigarette smoking, liver disease (CF related or other aetiology), haemolytic anaemia, or inability to perform an acceptable manoeuvre for the CO measurement were excluded. After the initial evaluation patients were divided into two groups according to the presence or absence of a respiratory exacerbation. Criteria for a respiratory exacerbation were considered the presence of one or more of the following symptoms: increased cough, increased sputum production, change in the quality of the sputum (more purulent, increased “thickness”, or presence of blood), sensation of increased chest congestion, increased dyspnoea, or decreased exercise tolerance and worsening of FEV1. 23 According to these criteria 29 patients were included in the stable CF group and 15 patients with mild to moderate respiratory exacerbations were included in the unstable CF group. The characteristics of the healthy subjects and patients are summarised in table 1.
Subject characteristics
STUDY DESIGN
This was a cross sectional study of a population of CF patients with and without exacerbations. In order to assess whether exhaled CO was reduced during the course of intravenous antibiotics we measured exhaled CO concentrations in seven patients admitted with a respiratory exacerbation for the administration of intravenous antibiotics. All subjects and patients gave informed consent to participate in the study which was approved by the local ethical committee.
MEASUREMENTS
Exhaled CO was measured by a modified electrochemical sensor with sensitivity from 1 part per million (ppm) to 500 ppm of CO, simultaneously with exhaled NO and carbon dioxide (CO2) by LR2000 chemiluminescence analyser (Logan Research Ltd, Rochester, Kent, UK) to control exhalation parameters (resistance 3 (0.4) mm Hg; exhalation flow 5–6 l/min). The detection limit for CO was 0.1 ppm. The analyser was calibrated weekly with a CO calibration gas and daily with NO calibration gas (Bedfont Scientific Ltd, Kent, and BOC Gases, Guildford, respectively). Ambient CO was recorded before every measurement of exhaled CO in all subjects. For exhaled CO and NO measurements the subjects exhaled slowly from total lung capacity over 15–20 seconds at an exhalation flow rate of 5–6 l/min. The mean value of the two measurements was recorded and the ambient CO was subtracted from the CO value to obtain the final result. All patients whose exhaled CO and NO concentrations were measured found it very easy to perform and all of them were able to do a correct manoeuvre after a single training session. No special skills were needed to perform this test and none of the patients was excluded because of an incorrect technique.
FEV1 was recorded using a Vitalograph Compact (Vitalograph Ltd, Buckingham, UK). The deterioration in FEV1 was calculated using the FEV1 measured at the moment of the initial evaluation and the FEV1 recorded in a stable condition within the last year.
STATISTICAL ANALYSIS
All variables are expressed as mean (SE). Patients and control groups were compared using the Student's ttest. FEV1 and exhaled CO were analysed by linear regression. A p value of <0.05 was considered statistically significant. Analysis of results was performed by using GraphPad Prism (GraphPad Software Inc, San Diego, USA).
Results
CLINICAL PARAMETERS
Age and sex distribution were comparable between the stable and unstable CF groups (table 1). In the unstable group all 15 patients presented with increased cough and sputum production, nine patients also had increased dyspnoea or decreased exercise tolerance and changes in the quality of sputum, and eight had the sensation of chest congestion.
In the stable CF group the mean FEV1 was 2.24 (0.2) l which was comparable to a previous stable FEV1 recorded within the last year of 2.31 (0.2) l. In the unstable CF group the mean FEV1 was 1.6 (0.1) l while the previously measured FEV1 when the patients were stable was 1.87 (0.1) l. The deterioration in FEV1 was not statistically significant but the overall fall in FEV1 in the unstable group was 14.8 (2.9)% (table 2).
Change in forced expiratory volume in one second (FEV1) in patients with respiratory exacerbation
Thirty two sputum cultures were performed. Of the 20 sputum cultures from patients with stable CF 12 (60%) were positive forPseudomonas aeruginosa(>105 cfu/ml), seven (35%) had other pathogens (Staphylococcus aureus,Haemophilus influenzae), and one sputum culture had normal flora. All 12 sputum cultures from patients with unstable CF were positive for Pseudomonas aeruginosa (>105 cfu/ml).
EXHALED CO
The exhaled CO concentration was 2.0 (0.1) ppm in the control group, 2.7 (0.1) ppm in the stable CF group (difference between means –0.67 (0.22), 95% confidence interval (CI) 0.22 to 1.12, p<0.01), and 4.8 (0.3) ppm in the unstable group (difference between means –2.82 (0.44), 95% CI 1.91 to 3.72, p<0.0001). When the values from stable and unstable CF patients were compared the mean differences were statistically significant (differences between means –2.15 (0.32), 95% CI 1.50 to 2.79, p<0.001; fig1).

Exhaled carbon monoxide (CO) in normal subjects and in cystic fibrosis patients with stable disease (stable CF) and with infective respiratory exacerbations (unstable CF).
EXHALED NO
The exhaled NO concentration was 7.3 (0.24) ppb in normal controls, 5.7 (0.29) ppb in stable CF patients, and 6.1 (0.72) ppb in unstable CF patients. There was a significant difference between control subjects and CF stable patients (difference between means 1.58 (0.48), 95% CI –2.54 to –0.62, p<0.01) but the difference between control subjects and unstable patients was not significant.
CORRELATIONS
There was a significant correlation between exhaled CO concentrations and the percentage change in FEV1(r = –0.46, p<0.01; fig 2) but there was no correlation between exhaled NO concentrations and FEV1(r = 0.06, p>0.05).

Correlations between percentage change in forced expiratory volume in the first second (FEV1) and exhaled carbon monoxide (CO).
EFFECT OF PSEUDOMONAS INFECTION
Exhaled CO concentrations in stable CF patients with a positivePseudomonas aeruginosa sputum culture were 2.82 (0.1) ppm compared with 2.88 (0.2) ppm in stable CF patients infected with other pathogens. The mean difference was not statistically significant.
EFFECT OF CORTICOSTEROID TREATMENT
Eleven patients were treated with corticosteroids (oral or inhaled), six in the stable CF group and five in the unstable CF group. Exhaled CO and NO concentrations from patients receiving corticosteroid treatment were not significantly different from those who were not.
EFFECT OF ANTIBIOTIC TREATMENT
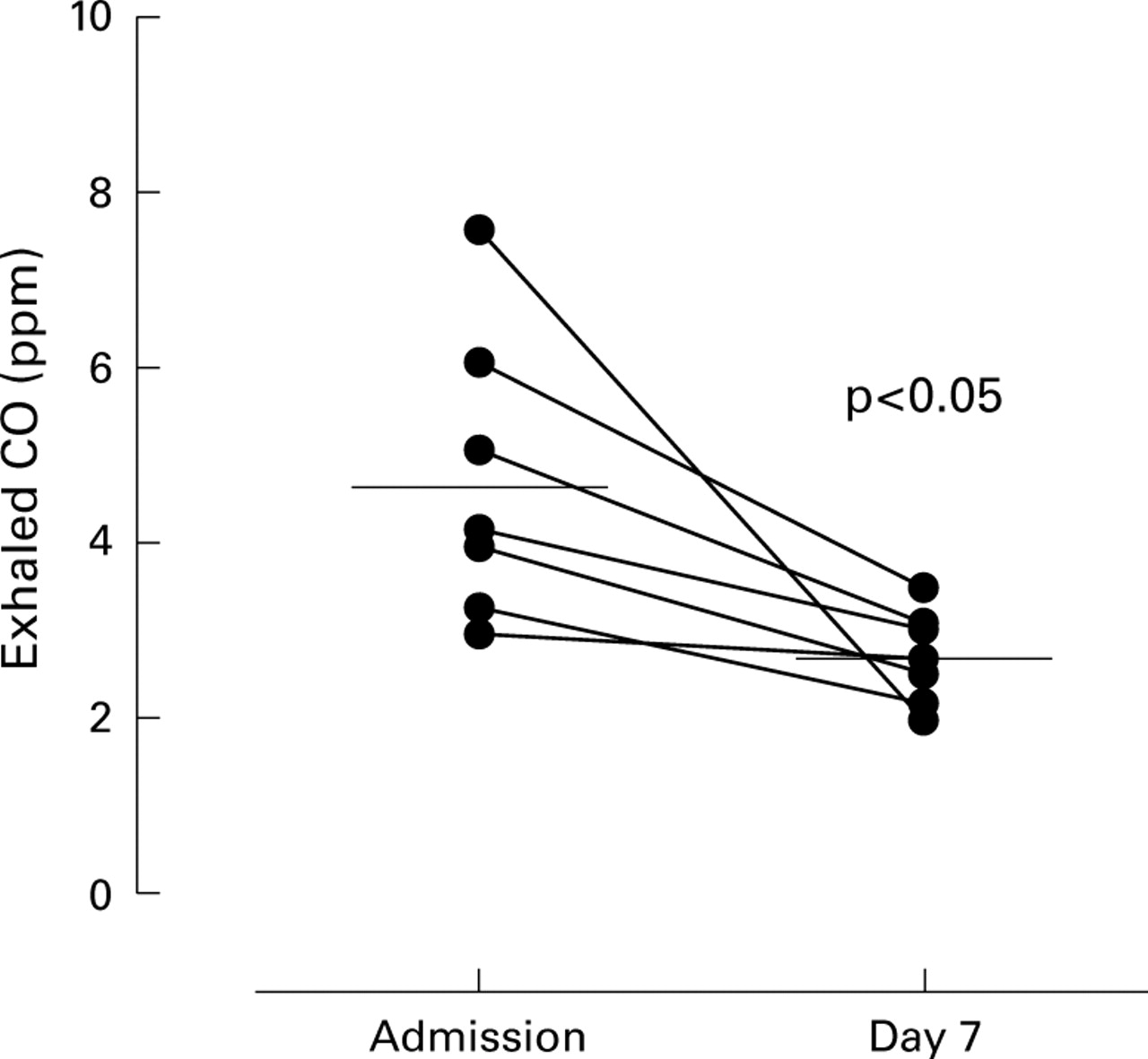
In order to assess whether exhaled CO is reduced during the course of intravenous antibiotics we measured exhaled CO concentrations in seven patients who were admitted with a respiratory exacerbation for the administration of intravenous antibiotics. At the time of admission their exhaled CO concentration was 4.7 (0.6) ppm and after seven days of treatment and improvement of symptoms and FEV1 it decreased to 2.7 (0.1) ppm (mean of differences 2.04, 95% CI 0.45 to 3.64, p<0.05; fig 3).
{kind=link}
{kind=link}
{kind=link}
Exhaled carbon monoxide (CO) in patients with infective respiratory exacerbation at admission and after seven days of intravenous antibiotics.
Discussion
This study shows that exhaled CO concentrations are increased in patients with CF and there is a further increase when a clinical worsening of the lung disease is present. Exhaled CO concentrations are increased in inflammatory lung diseases including asthma,6upper respiratory tract infections,7bronchiectasis,8 and cystic fibrosis.9Furthermore, increased levels of exhaled CO were found to be associated with increased expression of HO-1 in airway macrophages from asthmatic patients.24 These data suggest increased HO-1 activity in response to inflammation and oxidative stress and this may serve as an adaptive mechanism to protect cells from oxidative damage.25 ,26 In our study stable CF patients had higher levels of exhaled CO than controls. This agrees with previous findings of Konstan et al 1 who demonstrated significant infection and inflammation in adolescents and adults with mild lung disease without symptoms of active infection. There is also agreement with our data showing increased levels of exhaled CO in stable CF patients when compared with normal controls,9 although the levels of exhaled CO in our current study were different because of differences in the methodology of CO measurement. The higher concentration of exhaled CO in the unstable group may reflect further induction and activation of HO-1 in the airways in response to infection, increased inflammation, and increased oxidative stress.
The most characteristic feature of inflammation in the lungs of patients with CF is the persistent infiltration of large numbers of activated neutrophils which release reactive oxygen species and proteases (including elastase) that cause direct damage to the airway wall.27 The activation of neutrophils induces a respiratory burst which results in increased production of superoxide anions (O2 –) and hydrogen peroxide (H2O2).28 These data support our hypothesis that during exacerbations there is further oxidative stress as reflected by increased exhaled CO. The presence ofPseudomonas aeruginosa in the sputum culture from stable CF patients did not modify the levels of exhaled CO and suggests that no further activation of HO-1 may be possible in the presence of Pseudomonas aeruginosa.
There was a significant correlation between exhaled CO levels and the change in FEV1, showing that a deterioration in FEV1 along with the presence of respiratory symptoms of an infectious exacerbation are linked to an increase in exhaled CO. The overall trend shows a negative correlation between change in FEV1 and exhaled concentration of CO.
Increased levels of exhaled CO measured at the time of admission were significantly reduced following antibiotic treatment, suggesting that the activation of HO-1 during an exacerbation was downregulated by antibiotics. We found that measurement of the concentration of exhaled CO may be a useful test for the assessment of patients with CF and an indicator of deterioration and recovery from a respiratory exacerbation. In addition, we found a wide range of baseline levels of exhaled CO among stable and unstable patients which probably led to the overlap of CO values seen in figs 2 and 3 so we hypothesised that there is a different degree of oxidative stress in patients with a similar clinical condition. Exhaled CO values should therefore be considered as an individual measurement in each patient, and exhaled CO values recorded at the best clinical condition represent a baseline value with which future measurements can be compared during follow up.
Exhaled NO levels in stable CF patients were lower than controls and, although there was a statistical difference between controls and stable CF patients, it was not clinically relevant; there was no significant difference between stable and unstable CF patients. These data support previous reports showing a reduced expression of iNOS in airway epithelial cells from patients with CF,17 ,18 or a reduced exhaled NO due to combination of oxygen radicals released from neutrophils with NO to form peroxynitrite.29 It also shows that exhaled CO is a better marker of oxidative stress in cystic fibrosis.
In summary, exhaled CO concentrations are increased in stable CF patients and there is a further increase during mild to moderate exacerbations of the lung disease. The measurement of exhaled levels of CO could therefore be a useful test for monitoring patients with CF in order to assess airway inflammation in a non-invasive way, and prospective studies of its value in detecting early deterioration are now indicated.