Article Text

Abstract
The attitudes of Australian practitioners working in clinical genetics and obstetrical ultrasound were surveyed on whether termination of pregnancy (TOP) should be available for conditions ranging from mild to severe fetal abnormality and for non-medical reasons.These were compared for terminations at 13 weeks and 24 weeks. It was found that some practitioners would not facilitate TOP at 24 weeks even for lethal or major abnormalities, fewer practitioners support TOP at 24 weeks compared with 13 weeks for any condition, and the difference in attitudes to TOP between 13 weeks and 24 weeks is most marked for pregnancies which are normal or involve a mild disorder.
It is argued that a fetal abnormality criterion for late TOP is inconsistently applied, discriminatory and eugenic. Four possible moral justifications for current practice are examined, each of which would require significant changes to current practice. I argue in favour of a maternal interests criterion for any TOP.
- Termination of pregnancy
- abortion
- eugenics
- clinical genetics
Statistics from Altmetric.com
Introduction
In 1990, the Human Fertilisation and Embryology Act in the United Kingdom reduced the limit for “social termination” to 24 weeks, but placed no upper gestational limit on termination of pregnancy (TOP) when there is “substantial risk of serious handicap” (fetal disability ground) or if it is necessary to prevent “grave permanent injury to the physical or mental health of the pregnant woman” (maternal health ground).1
In Australia, law on TOP varies from state to state. Nearly all include a maternal interests criterion. A maternal health ground is the sole criterion in Victoria (Crimes Act 1958),2 NSW (Crimes Act 1900)3 and Queensland (Criminal Code Act 1899),4 where abortion is legal provided it is both necessary to preserve the woman from serious danger to her life or her physical/mental health and not out of proportion to the danger to be averted.5
The Australian Capital Territory (Crimes Act 1900) probably follows this principle.6 Western Australia (Acts Amendment (Abortion) Act 1998)7 has a similar maternal interest criterion until 20 weeks. South Australia (Criminal Law Consolidation Act 1935)8 includes both maternal interest and fetal disability grounds: abortion is lawful if continuance of the pregnancy would involve greater risk to the life or physical or mental health of the pregnant woman or there is a substantial risk that the child would suffer from such physical/mental abnormalities as to be seriously handicapped. The Northern Territory (Criminal Code Act 1997)9 has similar provisions to South Australia until 14 weeks. Tasmania (Criminal Code Act 1924)10 makes unlawfully procuring an abortion a crime, but does not define “unlawfully”.
When the Human Fertilisation and Embryology Act was passed, concern was expressed about what constituted a “substantial risk” and a “serious handicap.” Lilford and Thornton claimed that the issue might raise public attention in a dramatic way and expressed their “deep personal uncertainty”.11
In 1993, Green performed a survey of 391 obstetric consultants in the UK, asking them how late they would be prepared to offer TOP for anencephaly, spina bifida and Down's syndrome.12 She showed that 89% of consultants would offer TOP for anencephaly at 24 weeks. This fell to 64% after 24 weeks. For Down's syndrome, 60% would offer TOP at 24 weeks and this fell to 13% after 24 weeks. For open spina bifida, 53% would offer TOP at 24 weeks, 21% after 24 weeks. Green called for clarification of the law and willingness of obstetricians to implement it.
The aim of this survey was to examine professional attitudes to TOP for a range of conditions and the ethical justifications for these. Late TOP (LTOP) is defined as termination occurring at or after 20 weeks and early TOP (ETOP) as termination occurring before 20 weeks.
Methods
All practitioners involved in clinical genetics attending the Human Genetics Society of Australasia conference in Sydney, August 29-September 1, 1999, were surveyed. Obstetricians with specialist training in obstetric ultrasound who perform prenatal scanning were also surveyed. This was conducted at the Australian Association of Obstetrical and Gynaecological Ultrasonologists Conference, Sydney, October 14-17, 1999.
The survey of attitudes to selective TOP
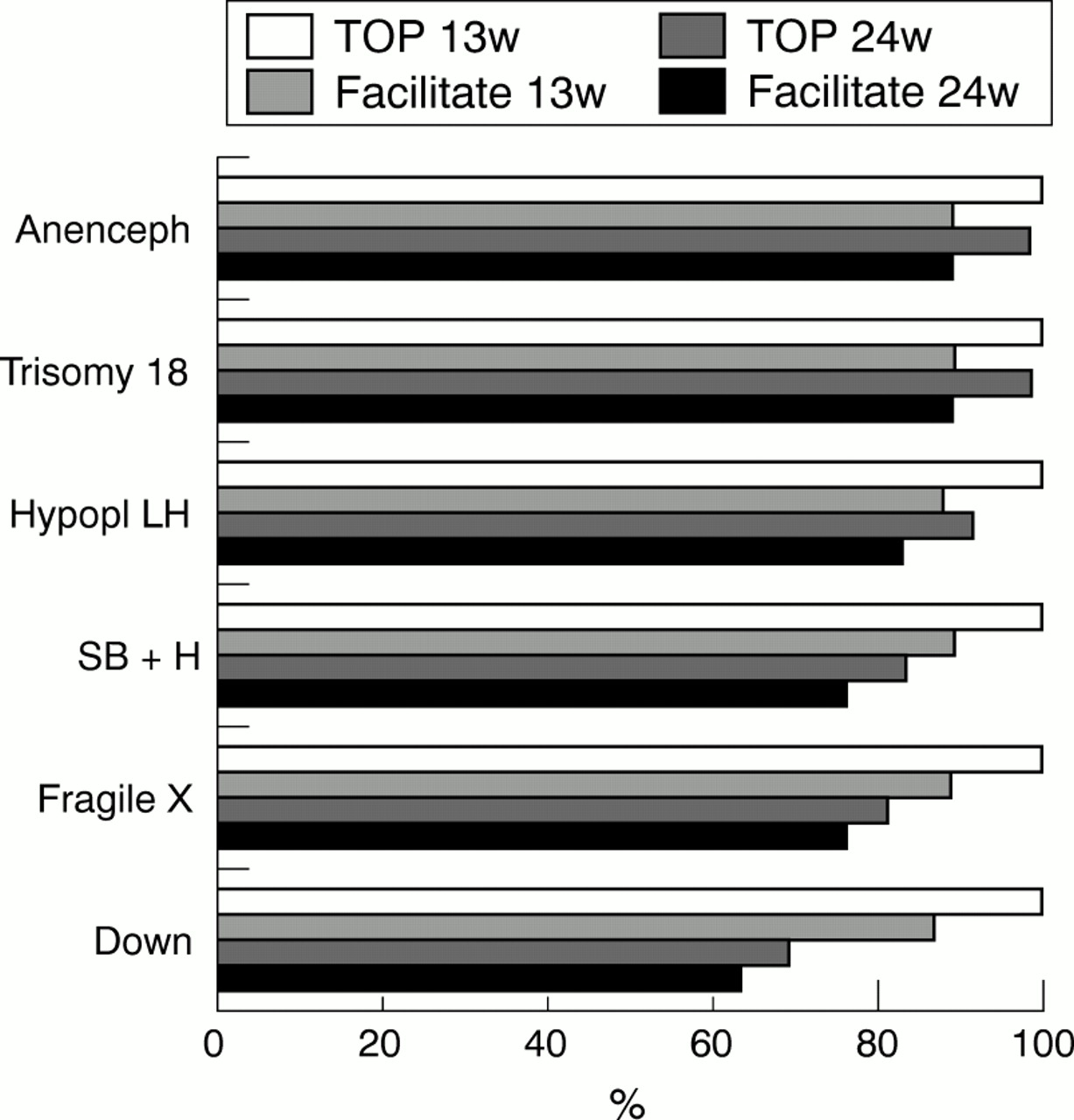
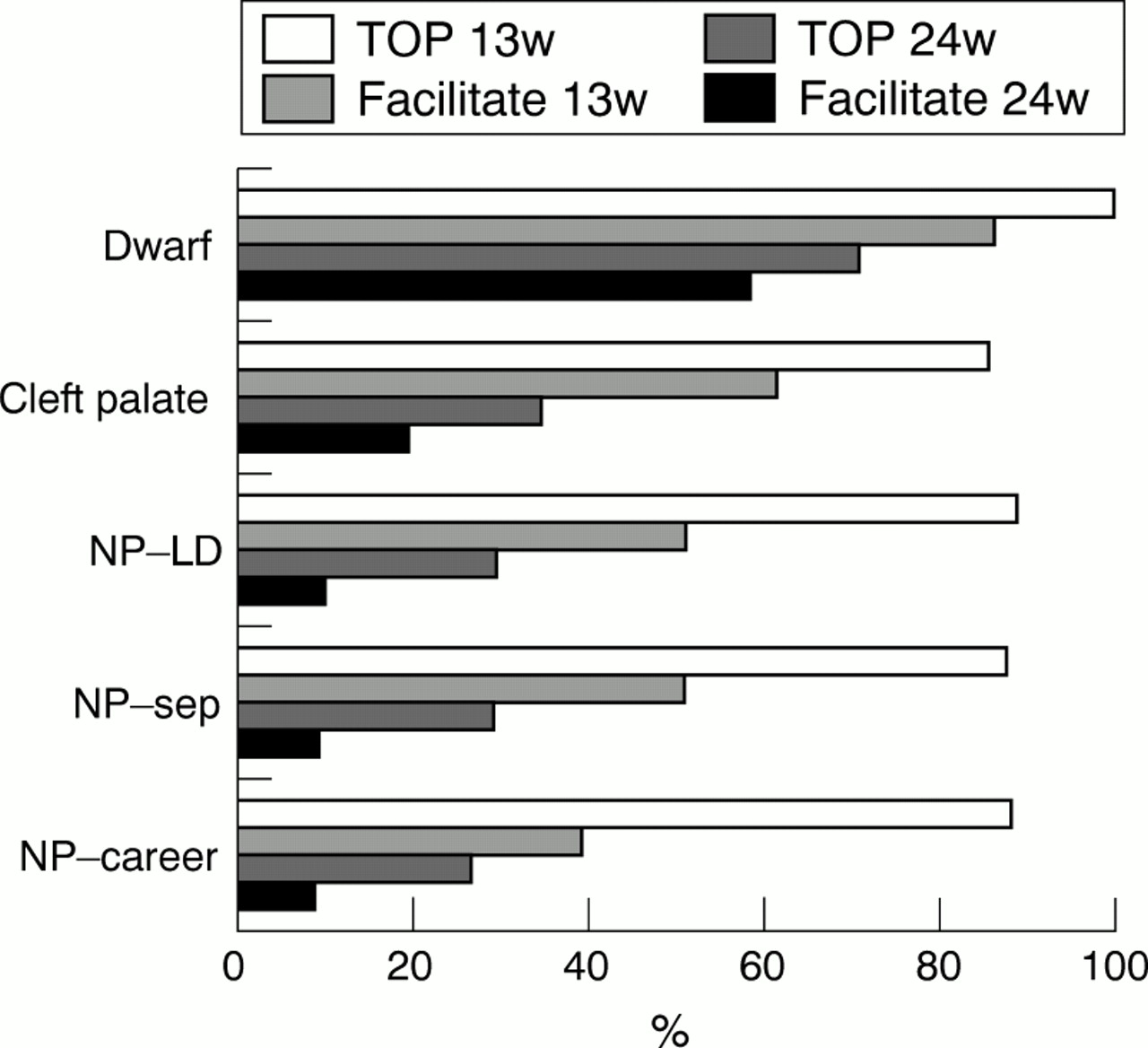
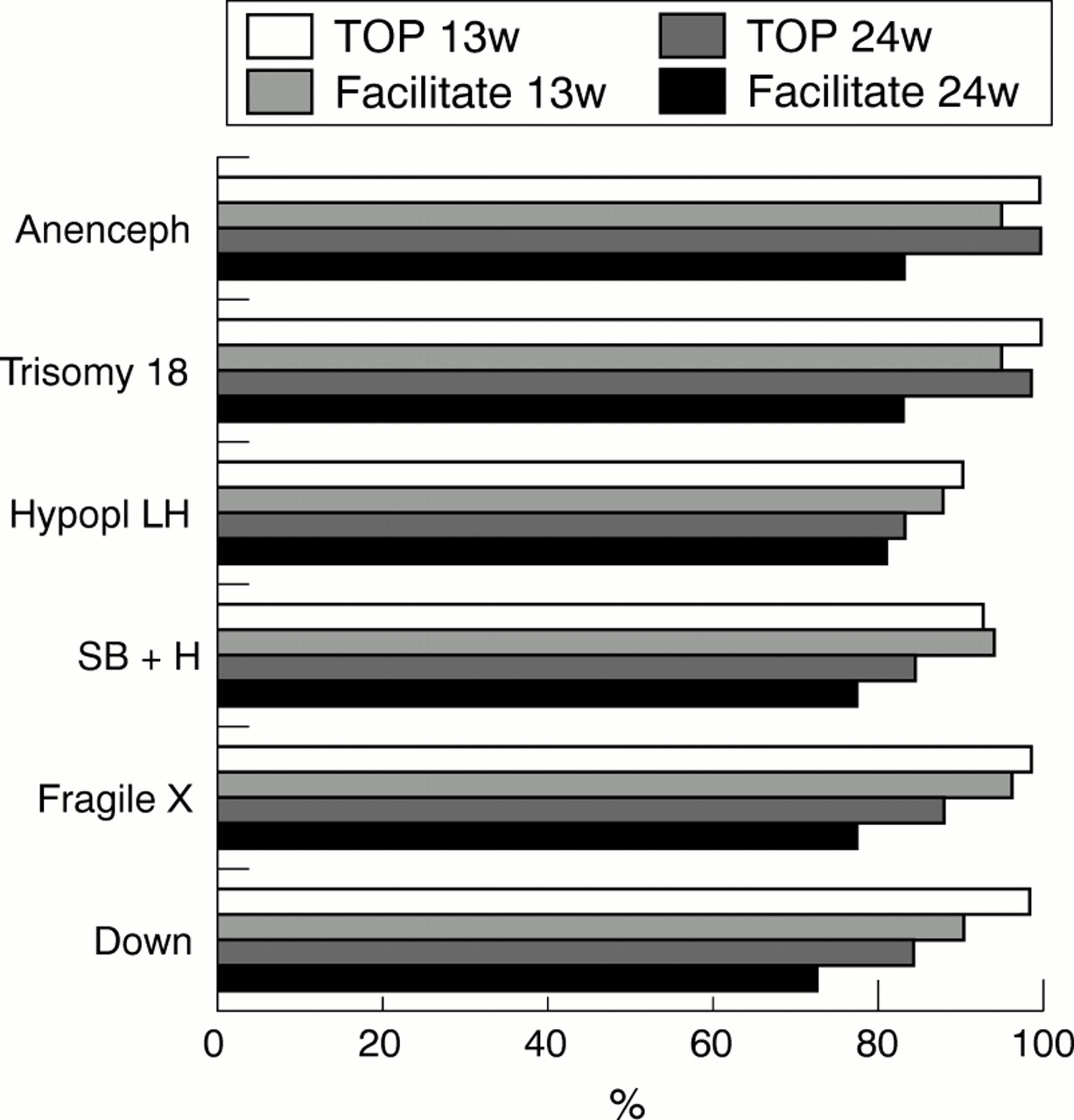
Respondents were asked to imagine that a pregnant woman presents after prenatal testing (including ultrasound and chorionic villus sampling) with one of several diagnoses. These included anencephaly (anenceph), trisomy 18, hypoplastic left heart (hypopl LH), spina bifida with hydrocephalus (SB+H), male fetus with full mutation for fragile X (severe mental retardation), Down's syndrome, achondroplasia (dwarf), and cleft palate. Respondents were also asked about pregnancies in which the fetus was normal but the pregnant woman had a learning disability and did not want the child (NP-LD), the pregnant woman's relationship had broken up (NP-sep), and the pregnant woman did not want child for career reasons (NP-career). For each condition, respondents were asked whether they believed TOP should be made available for the woman at 13 weeks and at 24 weeks gestation. Respondents were asked to ignore legal considerations. Respondents were also asked whether they personally would be prepared to facilitate a TOP for that condition at that gestation.
Results
Sixty responses were received from practitioners involved in clinical genetics from a possible total of approximately 80 respondents. These comprised 31 clinical geneticists, 23 genetic counsellors, five other and one did not specify which category. From the obstetrical ultrasound specialists, 41 responses were received from a possible 50 responses. Questionnaires were anonymous. Results are shown in figures 1-4. These data are compared to those of Green from English obstetricians in 1993, see table 1.
Comparison of Green's survey of obstetricians regarding willingness to offer termination at 24 weeks with our results regarding willingness to facilitate termination at 24 weeks

Responses of practitioners of clinical genetics
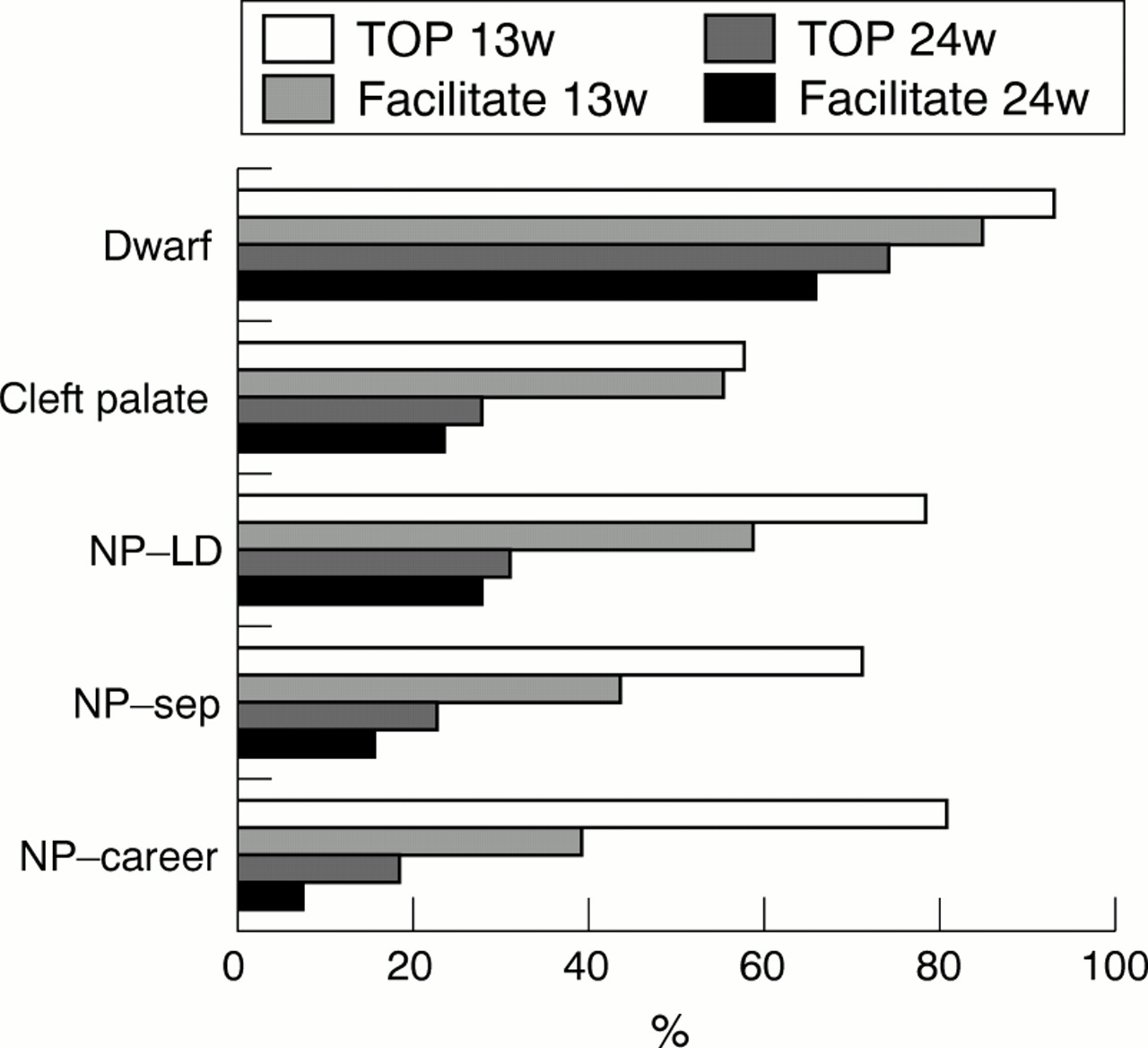
Responses of practitioners of clinical genetics
Responses of practitioners of obstetric ultrasound
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Responses of practitioners of obstetric ultrasound
These data showed that: (1) some practitioners would not facilitate TOP at 24 weeks even for lethal abnormalities; (2) fewer practitioners support TOP or would facilitate TOP at 24 weeks compared with 13 weeks for any condition; (3) the difference in (2) was most marked for pregnancies which are normal or involve a relatively mild disorder.
Discussion of the results
1. LACK OF PROFESSIONAL CONSENSUS AND SUBJECTIVE ASSESSMENTS
There was a lack of consensus around which abnormalities were severe enough to warrant termination, and up to what gestation TOP is acceptable. This implies that the options open to a particular patient are likely to be determined by the subjective values of the practitioner she happens to see. For example, around 75% of clinical geneticists and obstetricians specialising in ultrasound believed termination should be available for dwarfism at 24 weeks, though 25% did not.
2. GAP BETWEEN VALUES AND PRACTICE: PROFESSIONAL FAILING?
There was a gap between what practitioners thought “should be available” and “what they would facilitate”. Termination of pregnancy is a medical service. Practitioners may believe that TOP should be legally available in some circumstances, even though they believe it is wrong. However, in Australia and the UK TOP is a medical service funded from community resources. It should be offered in a consistent and reasonable way. The gap between values and practice raises questions about availability of abortion services.
There is a right of conscientious objection in both Australian and UK legislation (except in emergencies). But if individual value judgments preclude the delivery of a satisfactory and consistent medical service to a whole population, then selection and training of professionals should be examined.
While practitioners in this study were instructed to ignore the law, it is nevertheless possible that practitioners' willingness to facilitate TOP was influenced by state legislation. However, the consistency of these results with Green's suggests that differences in law are unlikely to account for different attitudes.
3. DISCRIMINATION: WHAT CONSTITUTES A “SERIOUS” FETAL ABNORMALITY?
United Kingdom law allows TOP on the ground of fetal abnormality after 24 weeks if the abnormality is “serious”. In current practice, after 16-20 weeks, or even as early as 13 weeks,13 TOP is only widely available for major or lethal abnormality. This survey has demonstrated wide variation in views of individual Australian practitioners. Some regard cleft palate as major, while some do not require any abnormality of the fetus, even at 24 weeks. A significant proportion of obstetricians and geneticists (over 10%) do not believe TOP should be offered at 24 weeks for usually lethal conditions including anencephaly and trisomy 18. Current practice around LTOP is discriminatory against women. Some women have access to LTOP while others do not. Some determined women learn the varying rules and travel interstate to obtain LTOP. Some simply acquiesce, go along with their doctor's personal values, and have a child which they do not want, sometimes with a serious abnormality.
4. EUGENICS
Current practice of LTOP is discriminatory in another way: it institutionalises killing of fetuses with abnormalities perceived to be severe, but not of fetuses with perceived minor abnormalities. This is discrimination against fetuses with disability. It is also a form of eugenics. “Eugenics” means “well born” and is tied to the notion of selective breeding. It is generally understood to be the intentional attempt to bring about a healthier or better population,14 especially by coercion or limiting options available, especially when there is state involvement.15
When a pervasive professional practice (or law) only allows TOP when there is fetal abnormality, this discriminates against abnormal fetuses. While pregnancy termination may not be compulsory, its effect is eugenic. In a similar way to that in which active and passive euthanasia are distinguished, active eugenics can be defined as offering the option of an intervention which directly promotes some eugenic outcome, for example offering financial inducements to the “fit” to reproduce. Passive eugenics is the closing off of options with the result that a eugenic outcome is more likely, for example not offering child support to people who choose to have a disabled child. Allowing LTOP for serious abnormality but disallowing it for minor or no abnormality is passive eugenics.
Many would object that current practice is not eugenic because the intention is to offer choice regarding continuing a pregnancy with a major abnormality, and not to promote a healthier population.16 It is true that practice may not be driven by primary eugenic intention, but the effect is the same. And the effect is foreseeable. I do not see any moral distinction between the intended effects of an action, and the foreseeable but unintended effects of that action.17 Not allowing women to terminate normal pregnancies has the same foreseeable effect as requiring the termination of abnormal pregnancies, at least in a culture where prenatal diagnosis is promoted and disability is viewed negatively. However, there is reasonable disagreement over whether there is a moral distinction between acts and omissions, and between intended and foreseen consequences.18
Can present practice be justified?
Four possible ways to justify current practice are explored below. It is argued that, in each of the four cases, current practice should change.
1. THE FETAL PATIENT VIEW
What happens at 20 weeks which might justify a change in practice from a permissive approach to ETOP to a eugenic approach to LTOP? Shortly after 20 weeks, the fetus becomes viable (currently about 24 weeks). Chervenak, McCullough and Campbell argue that before viability, the only link between the fetus and the pregnant woman is the woman's autonomy. They claim it is up to the pregnant woman to confer moral status before viability.19 However, after viability, the fetus becomes a patient, to whom doctors have duties. Chervenak and colleagues claim that LTOP is only appropriate for anomalies which are lethal or associated with absence of cognitive capacity.20
This view implies that many LTOP practices are wrong. It would not justify LTOP for achondroplasia, Down's syndrome, cleft palate or if the woman were suicidal. Many practitioners are prepared to offer LTOPs for these conditions.
Can viability justify limiting LTOP to lethal or very severe abnormalities? It is hard to see how—we cannot legally kill children with disabilities, even lethal ones. Infanticide of an anencephalic newborn is not thought to be justifiable by most doctors. (Indeed, it is murder.) If doctors should not kill these patients to whom they owe duties, why can they kill a 30-week fetal patient with similar rights and interests? Late termination of pregnancy seems equivalent to infanticide on the fetal patient view.
How might those attracted to viability respond? They might claim that there are social policy reasons for treating infanticide differently from feticide. A number of social, cultural, legal and historical institutions are founded upon birth having moral significance. The disruption of changing this would be enormous, with little benefit in practice.
But there are other problems. Viability is dependent on the state of technology. Over the last 20 years, it has dropped from 28 weeks to 24 weeks. So, if the fetus's right not to be killed is determined by viability, a fetus has a right not to be killed at 24 weeks now, but it did not have this right 20 years ago. Indeed, whether a fetus has a right to life will depend on its gestation, the extent of its abnormalities, the country and even the centre in which it is born. But why should our rights depend on these contingencies? A person with incurable cancer still has a right to life even if technology cannot save her.
How might those who appeal to viability respond? They might claim that viability, although necessary for moral status, is not sufficient. The fetus may become conscious at around the same time. Most estimates put consciousness commencing after 24-26 weeks.21, 22
Consciousness is important to having a life worth living. In recent years, courts have sanctioned the withdrawal of treatment from patients who are permanently unconscious.23 However, there are problems moving from this claim to the claim that a being acquires a right to life when it is conscious. Many non-human animals are conscious and are killed with impunity.24 Moreover, consciousness and viability do not seem enough to justify refraining from killing. There have been a number of Anglo-American cases in which the limitation of treatment was sanctioned where the patient was conscious and “viable” but suffering from cognitive impairment.25 In one case, there was no brain pathology at all.26
Those attracted to the fetal patient view could point to the difference between the fetal patient and these patients: the fetal patient normally has the potential to develop a richer life. Thus it is viability and consciousness, together with the potential to have a good life, which justifies the right to life of the fetal patient.
But once we admit potential onto the moral scales, we face problems. The 13-week fetus has much the same potential as a 24-week fetus. While it is true that a fetus which has survived until 24 weeks has a greater chance of surviving and living a good life, the magnitude of the difference in this probability may not be great. True, the 13-week fetus is not conscious and viable, but it will be in about 11 weeks. If potential matters, it has the potential to be conscious and viable. Once potential is admitted it is hard to see how any termination of pregnancy can be justified.
In summary, the fetal patient view may justify limiting LTOP to lethal or severe abnormalities. However, there are problems with relating an interest in life to viability, mere consciousness or potentiality. It may also require significant changes to our practices around ETOP or newborns, depending on which version is employed.
2. LATER FETAL MORAL STATUS: SELF CONSCIOUSNESS
According to the self-consciousness view, what is bad about death is the frustration of a being's desires for what should happen to its own life in the future. On this view, a human being acquires an interest in living when it becomes self-conscious, which is not until very late in pregnancy or after birth.27 This view is able to account for why it is acceptable to kill non-human animals, while it is wrong to kill humans.
According to this view, if there were nothing wrong with killing a fetus until very late into pregnancy, then killing a fetus which was severely disabled would not be wrong. However, the self-consciousness view would also justify LTOP of normal pregnancies. This view has the implication that infanticide is as acceptable as feticide (although there may be social policy reasons for treating these differently—see above). Many have found infanticide difficult to accept.
3. OBJECTIVE GOOD (PERFECTIONISTIC AND HEDONISTIC) CONSEQUENTIALIST THEORIES
Another justification for eugenic LTOP is appeal to a theory which aims to maximise objective good. The simplest is hedonistic utilitarianism. This view claims that what matters is happiness, and that we should maximise happiness. One version implies that it is good to bring happy beings into existence. Similar arguments would apply to more perfectionistic versions of consequentialism, which claim that what is good includes human beings achieving worthwhile things, developing their talents, etc.
In so far as major disability results in unhappiness, it is worse that seriously disabled children are born rather than healthy children. While hedonistic or perfectionistic versions of utilitarianism would justify selective LTOP of pregnancies involving major abnormalities, they would also not allow ETOP of normal pregancies. These theories also imply that it is wrong to use contraceptives to avoid having children who will have good lives.
Utilitarianism also urges us not only to include the good of the child produced, but also the good of all those affected by the existence of that child. Thus if having a child (disabled or abled) would cause a couple unhappiness (and that child unhappiness because its parents would be unhappy), those are reasons not to have the child. In practice, however, the happiness which a child would still experience over the whole of its life, even if moderately disabled, is likely to outweigh any decrement in the happiness of parents who must care for that child.
4. MATERNAL/FAMILY INTERESTS
The Human Fertilisation and Embryology Act includes a maternal health ground for LTOP which states that TOP is legal if continuation of the pregnancy will cause “grave permanent injury to the physical or mental health of the pregnant woman”. Most conservatives would allow LTOP if the life of the pregnant woman was threatened. That is the least controversial ground.
Two versions of the maternal interest view can be distinguished. According to the sufficient version, protecting maternal interests (for example, saving her life) is a sufficient ground for LTOP. The Abortion Act 1967 is one example.28 Another example is section 174 of the Criminal Code Act 1997 in the Northern Territory of Australia29 which states that it is lawful for a doctor to procure an abortion at any stage in pregnancy “if the treatment is given in good faith for the purpose only of preserving her life”.
The second version is the necessary version. This states that maternal interests (for example, saving her life) is a necessary condition for LTOP. An example is the Criminal Law Consolidation Act 1935 in South Australia which states that TOP is legal if it is necessary to save the pregnant woman's life.8
Imagine that Jane is 24 weeks pregnant and experiences severe high blood pressure. The only way to control her high blood pressure is to remove the fetus. Jane requests LTOP because she believes there is a significant chance the fetus will be disabled even with intensive care, which is available.
On the sufficient version of maternal interests, a LTOP could be performed because it would be sufficient to save her life. On the necessary version, LTOP should not be performed because it is not necessary to save her life—delivery and resuscitation of a 24-week fetus could equally achieve the goal of saving her life. Termination of pregnancy is sufficient but not necessary to save the Jane's life.
Which version should we accept? Much legislation which includes a maternal interest ground is framed in terms of the sufficient version. The necessary version is very restrictive. There will be virtually no cases today when the fetus must be killed rather than delivered after 24 weeks to protect the pregnant woman's life.
If we do accept the sufficient version, we have made an important assumption: we have assumed that the fetus does not have an interest in living. Why? When we are considering TOP after 24 weeks, we are considering killing a being who could live outside of the woman's body. If the fetus has any interest in living, then it would be preferable to deliver the baby alive rather than kill it (as the necessary version requires). My point is that if we accept the sufficient rather than the necessary verison of the maternal interests view—as many liberals and conservatives do—we have assumed that the fetus after 24 weeks does not have a right to life.
The sufficient version of a maternal interests view of the kind articulated in the Abortion Act 1967 is internally incoherent in one way. If it is implicitly based on the assumption that the fetus does not have a right to life, why is it is necessary for the TOP to be sufficient to prevent grave and permanent injury? From the fetal perspective, TOP at 24 weeks is like TOP at 14 weeks. Any maternal interest would be sufficient to justify TOP. Moreover, if the fetus does not have significant interests in living, imposing a fetal disability criterion for LTOP is unnecessary, discriminatory against some women, and has eugenic effects.
The sufficient version of the maternal interests view is consistent with practice around ETOP and LTOP. It assumes that the fetus does not have a significant interest in living. It implies that we should liberalise our approach to LTOP, and eschew consideration of fetal abnormality as a ground for LTOP. If we are to give any weight to maternal interests, this should be the sole ground for justifying TOP, early or late.
It is important to remember that some families gain much from rearing a child with a disability. If families want to continue a pregnancy, disabled or abled, they should be supported. Termination of pregnancy is also occasionally associated with great anxiety, stress and sometimes depression. Even so, some parents who have cared for a child with a disability stress the difficulty of such care.30 The evaluation of the impact of a child on maternal interests should generally be the woman's to make.
The effect of any child on maternal wellbeing should not be underestimated. Bringing up a child for 18 years is an enormous physical, emotional and financial effort. Recent decisions in Australia have extended maternal health interest justifications for abortion to include the impact of care of a child after birth on the woman's health (the Kirby ruling),31 at least in ETOP.
Significance of LTOP and the law relating to it
Doctors who are involved in LTOPs are in a tenuous legal position. The Infant Life (Preservation) Act 1929 in the UK makes it a serious crime unlawfully to destroy a viable fetus.32 Montgomery, however, claims its importance “is marginal”. “Where a doctor has a defence under the Abortion Act, it will be a defence to a prosecution under the Infant Life Preservation Act”.33 This remains untested.
Legislation relevant to LTOP varies from state to state in Australia. In Victoria (Crimes Act 1958)2 and South Australia (Criminal Law Consolidation Act 1935)8 it is a criminal offence of child destruction to unlawfully terminate a 28-week fetus, and probably a fetus capable of being born alive of earlier gestation. While Victorian law gives no indication as to what might constitute a lawful LTOP, in South Australia (Criminal Law Consolidation Act 1935) LTOP is legal if two doctors have examined the pregnant woman and judge it to be necessary to save her life.34 Queensland, Western Australia and the Northern Territory all have child destruction offences which apply when a pregnant woman is about to deliver a child. It is not clear whether these apply only to very late pregnancy when the woman is about to go into labour, or to any viable fetus. In Western Australia, for a TOP to be lawful (at or after 20 weeks gestation) two members of an appointed panel of at least six medical practitioners must judge that the mother or the unborn child has a “severe medical condition”. In the Northern Territory, termination after 23 weeks is legal to save the pregnant woman's life. New South Wales and Tasmania do not have separate offences of child destruction. The Australian Capital Territory (ACT) also has child destruction legislation, but it is not clear whether it applies only at the very end of pregnancy when delivery is imminent.6
Although doctors are unlikely to be prosecuted, these laws bring inconsistency and unclarity into existing legislation relating to LTOP.35 The law should be clarified to state that LTOP is permissible in the pregnant woman's interests.
The Royal College of Obstetricians and Gynaecologists' (RCOG) ethics committee produced a report on the ethics of LTOP in 1998.36 It stated that over 100 terminations of pregnancy were performed after 24 weeks in England in 1996. The report documented TOP for dwarfism diagnosed at 28 weeks in a pregnant woman who was a dwarf. The TOP was prompted by “the mother's compelling description of her own life and suffering and her genuine repeated request”. The RCOG also reported two TOPs for Down's syndrome and spina bifida at 34 weeks. It recognised that LTOP has become “a standard management option in tertiary referral centres for serious abnormalities diagnosed after 24 weeks”.
The number of women presenting for LTOP may increase. Firstly, some abnormalities may not be detected until late in the mid trimester, for exmaple, dwarfism. Secondly, it may be preferable to do prenatal ultrasound anomaly scans at 22 weeks to detect as many anomalies as possible. This has become standard in some UK centres. Thirdly, the number of genetic tests is increasing, and these tests may only be considered after an anomaly is seen on the 18-22 week ultrasound. If a genetic condition is rare, then it may take much longer to obtain a result.
Changing the law and practice: the maternal interest standard
I have argued that current practice around TOP is inconsistent, discriminatory and eugenic. There are three options.
OPTION 1
Allow LTOP only for fetal abnormalities which result in at least severe cognitive or functional impairment. This is supported by the fetal patient view, which may also require similar restrictions on ETOP if we give weight to potentiality.
OPTION 2
Allow LTOP for fetal abnormality but also some normal pregnancies. This is supported by one version of the maternal/family interests view. It assumes that the fetus does not have a moral status until birth or afterwards. It is most consistent with current law in this area. It is the least discriminatory and eugenic option.
OPTION 3
Do not allow TOP of normal pregnancies at any gestation but allow termination of abnormal pregnancies at any gestation. This is supported by hedonistic or perfectionistic utilitarianism.
Whichever option we choose, current practice should change. I favour option 2. It is most consistent with current law in Australia and the UK, which includes a maternal interests ground for LTOP. Admitting a fetal disability ground, as UK legislation and current practice do, introduces discrimination, is a form of passive eugenics and probably cannot be supported by any plausible account of fetal moral status without significant revision of practice.
Acknowledgments
The author wishes to thank Gillian Vallance and all those who made invaluable contributions to this paper who prefer to remain anonymous.
Footnotes
-
Julian Savulescu BMedSci (Hons), MB, BS (Hons), PhD, is Director of the Ethics Program at the Murdoch Children's Research Institute and Associate Professor of Medical Ethics, University of Melbourne, Australia.
Other content recommended for you
- Dilemma for appeals to the moral significance of birth
- Conscientious objection in medicine
- Reproductive autonomy and the ethics of abortion
- Thomson, the right to life, and partial birth abortion or two MULES* for Sister Sarah
- Preserving women’s reproductive autonomy while promoting the rights of people with disabilities?: the case of Heidi Crowter and Maire Lea-Wilson in the light of NIPT debates in England, France and Germany
- Why there is no dilemma for the birth strategy: a response to Bobier and Omelianchuk
- Avoiding anomalous newborns: preemptive abortion, treatment thresholds and the case of baby Messenger
- Palliative care for prenatally diagnosed lethal fetal abnormality
- Terminating pregnancy after prenatal diagnosis—with a little help of professional ethics?
- About abortion in Britain