Article Text

Abstract
Background The indications for intestinal transplantation (ITx) are still debated. Knowing survival rates and causes of death on home parenteral nutrition (HPN) will improve decisions.
Methods A prospective 5-year study compared 389 non-candidates (no indication, no contraindication) and 156 candidates (indication, no contraindication) for ITx. Indications were: HPN failure (liver failure; multiple episodes of catheter-related venous thrombosis or sepsis; severe dehydration), high-risk underlying disease (intra-abdominal desmoids; congenital mucosal disorders; ultra-short bowel), high morbidity intestinal failure. Causes of death were defined as: HPN-related, underlying disease, or other cause.
Results The survival rate was 87% in non-candidates, 73% in candidates with HPN failure, 84% in those with high-risk underlying disease, 100% in those with high morbidity intestinal failure and 54%, in ITx recipients (one non-candidate and 21 candidates) (p<0.001). The primary cause of death on HPN was underlying disease-related in patients with HPN duration ≤2 years, and HPN-related in those on HPN duration >2 years (p=0.006). In candidates, the death HRs were increased in those with desmoids (7.1; 95% CI 2.5 to 20.5; p=0.003) or liver failure (3.4; 95% CI 1.6 to 7.3; p=0.002) compared to non-candidates. In deceased candidates, the indications for ITx were the causes of death in 92% of those with desmoids or liver failure, and in 38% of those with other indications (p=0.041). In candidates with catheter-related complications or ultra-short bowel, the survival rate was 83% in those who remained on HPN and 78% after ITx (p=0.767).
Conclusions HPN is confirmed as the primary treatment for intestinal failure. Desmoids and HPN-related liver failure constitute indications for life-saving ITx. Catheter-related complications and ultra-short bowel might be indications for pre-emptive/rehabilitative ITx. In the early years after commencing HPN a life-saving ITx could be required for some patients at higher risk of death from their underlying disease.
- Intestinal failure
- home parenteral nutrition
- intestinal transplantation
Statistics from Altmetric.com
Significance of this study
What is already known about this subject?
Patients with irreversible intestinal failure are destined to remain on life-long home parenteral nutrition (HPN) or to undergo intestinal transplantation (ITx).
The current indications ITx are based on retrospective analysis of case series and are represented by risk of death due to HPN complications (HPN failure) or to the underlying disease.
Recently, the results of a 3-year prospective study including non-candidates and candidates for ITx supported the use of HPN as the primary treatment for intestinal failure, and showed that only HPN failure due to HPN-associated liver failure or major central venous catheter-associated complications were appropriate indications for a life-saving ITx.
More recent data from experienced ITx centres have been compared favourably with the survival reported in retrospective series of HPN patients. It was suggested that the role of ITx should be expanded from a life-saving procedure for patients developing HPN failure to a pre-emptive/rehabilitative procedure applicable to all patients with irreversible IF.
What are the new findings?
HPN is confirmed as the treatment of choice for intestinal failure.
An early referral for a life-saving ITx is mandatory for patients with HPN-associated liver failure or invasive intra-abdominal desmoids.
Central venous-catheter-related major complications and ultra-short bowel might be indications for a pre-emptive/rehabilitative ITx in case by case selected patients.
The risk of death on HPN is greater in the early years of treatment and the causes of death on HPN are mainly underlying disease-related in the early years and mainly HPN-related in the late years of HPN.
How might it impact on clinical practice in the foreseeable future?
Patient referral for a life-saving ITx should be limited to HPN-related liver failure and to invasive intra-abdominal desmoids.
An early referral to expert intestinal failure centres is mandatory for all patients with irreversible intestinal failure, to devise the most appropriate case-by-case treatment strategy.
Studies are required:
To compare the cost-utility of HPN and ITx, in order to define the indications for a pre-emptive or a rehabilitative ITx in patients with central venous-catheter-related major complications or ultra-short bowel.
To identify patients at early risk of death on HPN due to the underlying disease and who could be candidates for an early life-saving ITx.
Introduction
Intestinal failure (IF) results from obstruction, dysmotility, surgical resection, congenital defect or disease-associated loss of absorption, and is characterised by the inability to maintain protein energy, fluid, electrolyte or micronutrient balance.1 Patients with irreversible IF are destined to remain on life-long home parenteral nutrition (HPN) or to undergo intestinal transplantation (ITx). The choice between these treatments should reflect the data on their relative safety and efficacy for different indications.
A recent 3-year prospective follow-up including both adults and children on HPN for IF, compared ‘non-candidates’ for ITx, having neither indications nor contraindications, with ‘candidates’ who had an indication without a contraindication for ITx.2 3 Indications for ITx were categorised as HPN failure, according to the USA Center for Medicare and Medicaid Services definitions,4 and high risk of death or high morbidity related to the underlying intestinal failure, according to the American Society of Transplantation position paper.5 The results supported the use of HPN as the primary treatment for IF, and showed that only patients with HPN failure due to HPN-associated liver failure or major central venous catheter (CVC)-associated complications had a statistically significant increased risk of death on HPN. It was suggested that ITx should be proposed only as a life-saving procedure for patients with HPN failure.6
More recent data from experienced ITx centres in the USA showed a 5-year patient survival of 70% and were compared favourably with the survival reported in retrospective series of HPN patients.7 It was suggested that the role of ITx should be expanded from a life-saving procedure for patients developing HPN failure to a pre-emptive/rehabilitative procedure applicable to all patients with irreversible IF, aiming to avoid the development of HPN-failure and to recover patient autonomy more fully.7–9 However, such a comparison is biased on several criteria10 and the indications for ITx remain controversial. Thus, our unique cohorts of patients on HPN for irreversible IF were subject to survey for two more years. The present results give new information about the survival rates and the causes of death when on HPN, which could improve decisions in referral for ITx.
Methods
Details of the study design and its methodology have been previously published.2 3 The essential information is described in figure 1 and can be summarised as follows.

Study design.
Baseline patient enrolment
The two cohorts of patients were selected in January 2004, through a cross-sectional survey on the prevalence of candidature for ITx.2 Forty-one European HPN centres enrolled all their patients currently on HPN for benign IF. Sex, age, primary disease, cause of IF, duration of HPN (years), and indication and/or contraindication for ITx, were recorded. Causes of IF were classified as short bowel syndrome, chronic motility disorders, intestinal fistulas or extensive small bowel mucosal disease. The patients' ages were categorised as adult (>18 years) or children (≤18 years).
Indications for ITx were classified into three categories according to the criteria of the USA Medicare and Medicaid Services4 and the American Society of Transplantation5:
Failure of HPN
1a) Impending (total bilirubin above 3–6 mg/dl/54–108 μmol/l, progressive thrombocytopenia, and progressive splenomegaly) or overt liver failure (portal hypertension, hepatosplenomegaly, hepatic fibrosis or cirrhosis) due to HPN/IF-associated liver injury
1b) CVC-related thrombosis of ≥2 central veins
1c) Frequent and severe CVC-related sepsis: two or more episodes per year of systemic sepsis secondary to line infections requiring hospitalisation; a single episode of line-related fungaemia; septic shock and/or acute respiratory distress syndrome
1d) Frequent episodes of severe dehydration despite intravenous fluids in addition to HPN
High risk of death attributable to the underlying disease
2a) Intra-abdominal invasive desmoid tumours
2b) Congenital mucosal disorders
2c) Ultra-short bowel syndrome (gastrostomy, duodenostomy, residual small bowel <10 cm in infants and <20 cm in adults)
IF with high morbidity or low acceptance of HPN
3a) Need for frequent hospitalisation, narcotic dependency or inability to function
3b) Patient's unwillingness to accept long-term HPN
As a residual short bowel of <50 cm in adults and <25 cm in children was reported to be a risk factor for HPN dependency and for HPN failure but not for survival,11 in the present survey, shorter lengths of residual small bowel were arbitrarily used to define ultra-short bowel as an indication for ITx.
Contraindications for ITx were taken from the guidelines for patients eligible for solid organ transplantation,12 and were categorised as absolute or relative. Patients having an indication and no contraindication, or a relative contraindication with a positive clinical judgement for candidacy, were considered candidates for ITx.2
A total of 854 patients was evaluated (688 adults and 166 children): 418 were non-candidates with no indication and no contraindication for ITx; 271 were non-candidates with at least one contraindication for ITx; 165 were candidates for ITx, six of whom had a relative contraindication associated with positive clinical judgement for ITx.2
Follow-up study
The group of non-candidates with no contraindication for ITx and the group of candidates were compared. Twenty-nine non-candidates and nine candidates were lost at/or shortly after baseline. Follow-up was carried out on 389 non-candidates and 156 candidates.
Data were collected through a structured questionnaire. Each patient's status on 31 December of each year was recorded as: weaned off HPN (date), stable on HPN, referred or listed for ITx (date and indication criteria), transplanted (date and type of transplant), deceased: on HPN or after ITx (date and description of the primary pathological condition from which the final event originated). The descriptions of the causes of death on HPN were classified as HPN-related, related to underlying disease, or other unassociated causes. Three authors (LP, AVG, MS) independently allocated each patient into one category. The final classification was based on consensus agreement. Causes of death after ITx were considered ITx-related if due to graft rejection, intractable infection or surgical complications.
The questionnaire was completed for each individual patient by the local medical team in anonymised form, codified for linkage with previous years' data. The research was thus based on information taken from that already present in the patient records at the time of the data collection. The study was conducted with full regard to confidentiality and protection of the individual patient.
Statistical analysis
Patients were deemed to have irreversible IF if they were still on HPN or had received a transplant by the end of the follow-up period.
Survival on HPN was defined as the time from baseline (1 January 2004) to the date of death, of ITx, or the end of follow-up (31 December 2008). Survival after ITx was defined as the time from the date of ITx to the date of death or the end of follow-up. For patients lost during follow-up, the data used were those up to 31 December in the last full year of observation.
Patient survival was estimated by the Kaplan–Meier method, and group comparisons were made with the log-rank test. Means, standard deviations and frequencies were used as descriptive statistics. The χ2 and Fisher's exact tests were applied as appropriate.
Survival probability on HPN or after ITx was evaluated according to the patient characteristics at baseline. ITx recipients were also categorised by their status at time of call for transplantation (at home or in hospital) and by the type of ITx (without or with liver).
In non-transplanted candidates, the HRs for death associated with having an indication for ITx were compared with those in non-candidates using the Cox regression model.
The SSPS/PC+ statistical package for Windows, version 8.0 was used for the analyses. Probabilities of survival and relative risks of death are presented with their 95% CIs. A two-tailed p value less than 0.05 was considered as statistically significant.
Results
Table 1 shows the yearly and the 5-year outcome of the two cohorts of patients. The frequency of weaning from HPN was higher in non-candidates, whereas the frequencies of death on HPN and of those who underwent ITx were higher in candidates (p<0.001).
Yearly and 5-year outcome of patients on home parenteral nutrition for intestinal failure included in the follow-up. Baseline inclusion, 1 January 2004
Five-year survival rate, causes of death and factors associated with probability of survival in patients with irreversible IF
The 97 patients who were weaned from HPN were excluded from the statistical analysis, therefore 297 non-candidates and 151 candidates, all deemed to have irreversible IF were compared.
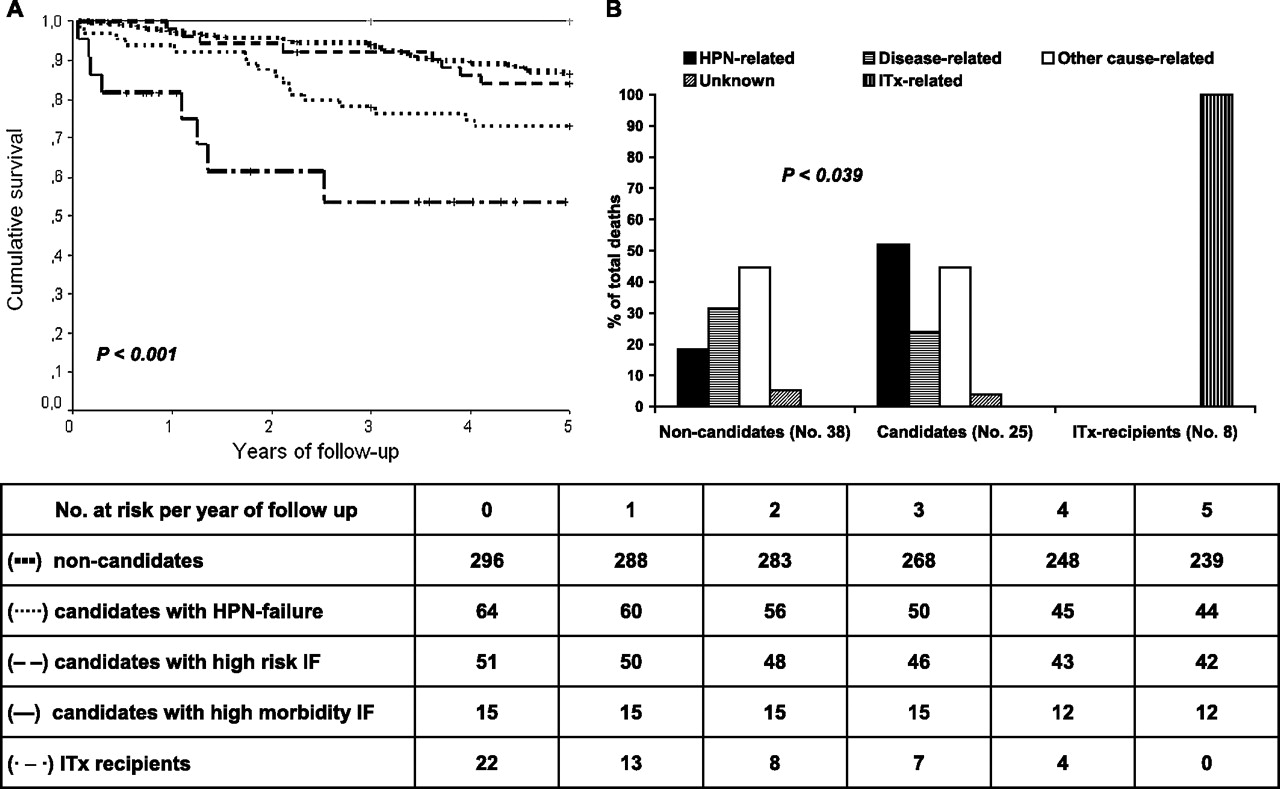
The probability of survival was 87% (CI: 83% to 91%) in non-candidates, 73% (CI: 62% to 84%) in candidates with HPN-failure, 84% (CI: 74% to 94%) in those with high-risk underlying disease, 100% in those with high morbidity IF/low acceptance of HPN and 54% (CI: 29% to 79%) in ITx recipients (p<0.001) (non-candidates vs HPN-failure p<0.003, vs high-risk underlying disease p=0.631; vs high morbidity IF/low acceptance of HPN p=0.168; ITx recipients vs non-candidates p<0.001, vs HPN-failure p=0.036, vs high-risk underlying disease p=0.003; vs high morbidity IF/low acceptance of HPN p<0.001) (figure 2A).
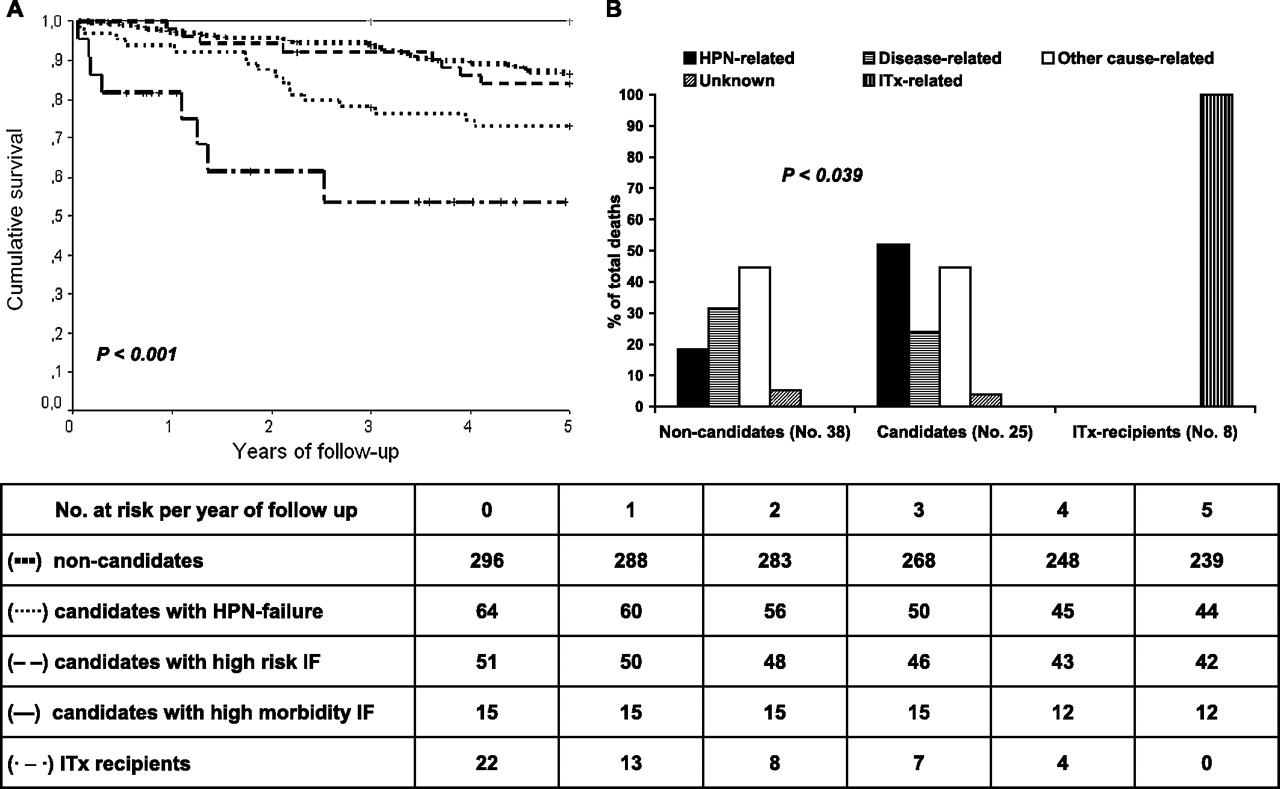
Five-year survival rates (Kaplan–Meier analysis) and causes of death on home parenteral nutrition (HPN) and after intestinal transplantation (ITx) in patients with irreversible intestinal failure. (A) Survival rate in non-candidates (▪▪▪), candidates with HPN-failure (···), candidates with high-risk underlying disease (- -), candidates with high morbidity IF/low acceptance of HPN (—), ITx recipients (·─·). Non-candidates versus HPN-failure p<0.003, versus high-risk underlying disease p=0.631, versus high morbidity IF/low acceptance of HPN p=0.168, versus ITx recipients p<0.001); ITx recipients versus HPN-failure p=0.036, versus high-risk underlying disease p=0.003, versus high morbidity intestinal failure/low acceptance of HPN (p<0.001). (B) Causes of death. Non-candidates on HPN (total deaths 38): HPN-related (7), underlying disease-related (12), other causes related (17), unknown (2). Candidates on HPN (total deaths 25): HPN-related (13), underlying disease-related (6), other causes related (5), unknown (1). ITx recipients (total deaths 8): ITx-related (8).
In the total group of patients who remained on HPN, there were 63 deaths. The causes were HPN-related in 20 (32.7%), underlying disease related in 18 (28.6), other cause-related in 22 (34.9%) and unknown in three (4.8%). In non-candidates, the cause of death was mainly independent of HPN or the underlying disease, whereas in candidates death was mainly HPN-related (p=0.039). In ITx recipients, all the deaths were related to the ITx (graft rejection three, intractable infection five) (figure 2B).
The mortality rate was significantly associated: with the HPN duration at baseline in non-candidates; with the age category and with the individual indications for ITx in candidates; with gender and patient status at the time of transplantation in ITx recipients (table 2).
Five-year mortality rate in patients with irreversible intestinal failure, according to the characteristics at baseline (1 January 2004). Patients weaned off home parenteral nutrition were excluded from the analysis
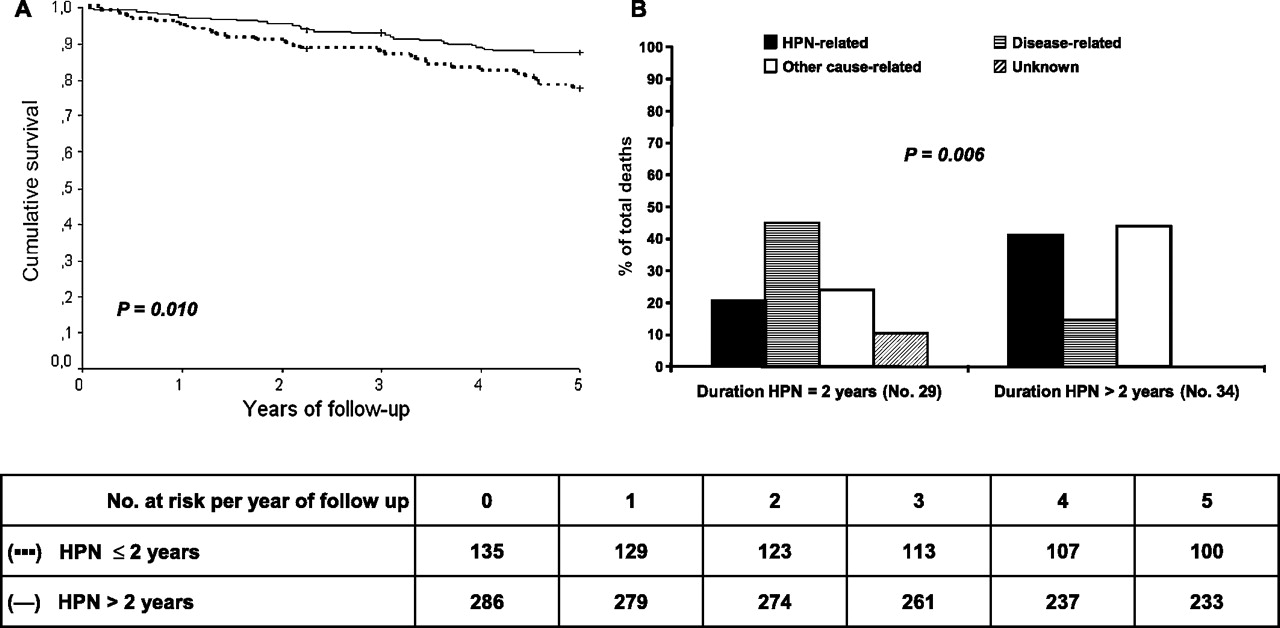
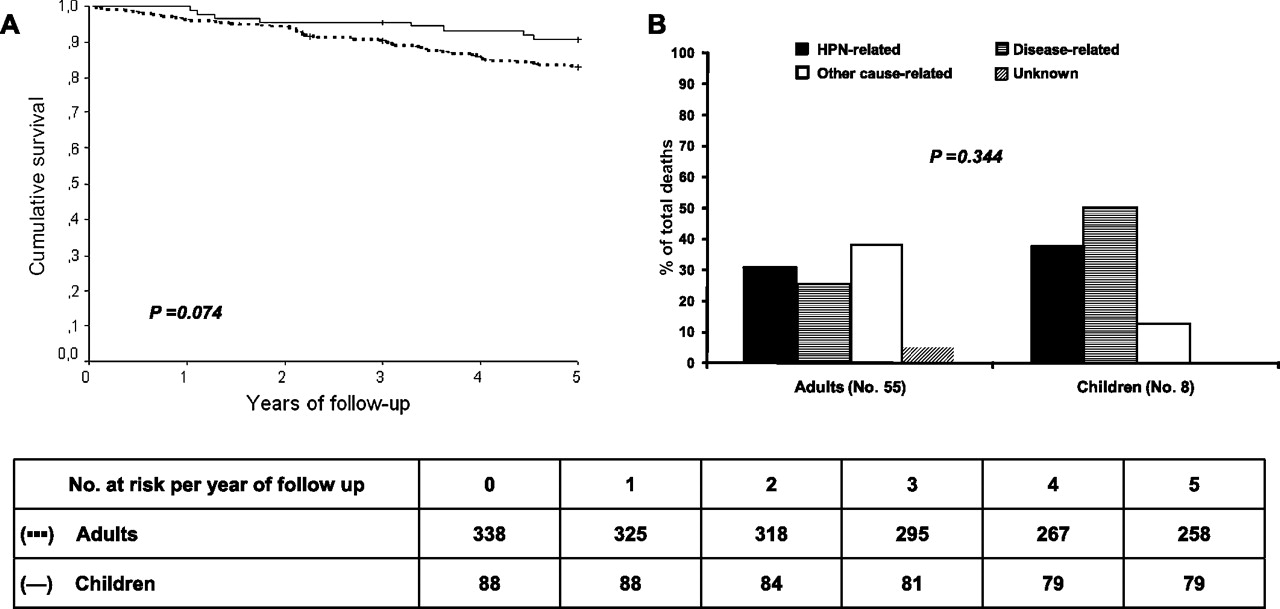
Pooling the non-candidates and candidates, the 5-year survival rate was significantly associated with the HPN duration at baseline, ≤2 years, 78% (CI: 71% to 85%), >2 years 88% (CI: 84% to 92%) (p=0.010) (figure 3A), but not with the age category, adults 83% (CI: 79 to 87), children and adolescents 91% (CI: 85% to 97%) (p=0.074) (figure 4A).The primary cause of death was generally the underlying disease in patients with HPN duration ≤2 years, and HPN-related in those on HPN duration >2 years (p=0.006) (figure 3B), whereas no statistically significant difference was observed between the age categories (figure 4B).

Five-year survival rates (Kaplan–Meier analysis) and causes of death on home parenteral nutrition (HPN) in patients with irreversible intestinal failure. (A) Survival rate on HPN in non-candidates and candidates for intestinal transplantation pooled together, categorised for the HPN duration at baseline (time of inclusion in the study): (···) ≤2 years and (—) >2 years. (B) Causes of death. Duration of HPN ≤2 years (total deaths 29): HPN-related (6), underlying disease-related (13), other causes related (7), unknown (3). Duration of HPN >2 years (total deaths 34): HPN-related (14), underlying disease-related (5), other causes related (15).
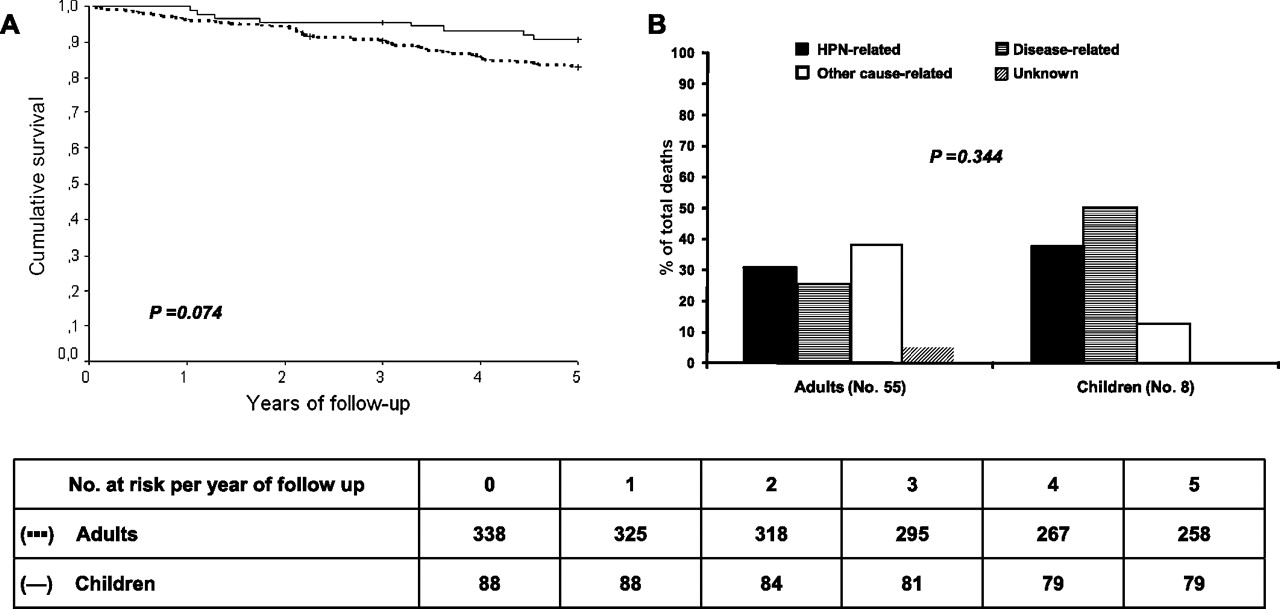
Five-year survival rates (Kaplan–Meier analysis) and causes of death on home parenteral nutrition (HPN) in patients with irreversible intestinal failure. (A) Survival rate on HPN in non-candidates and candidates for intestinal transplantation pooled together, categorised for age: (···) adults and (—) children (≤18 years). (B) Causes of death. Adults (total deaths 55): HPN-related (17), underlying disease-related (14), other causes related (21), unknown (3). Children (total deaths 8): HPN-related (3), underlying disease-related (4), other causes related (1).
In comparison with non-candidates, the 5-year HR for death on HPN according to the individual indications for ITx was significantly increased only for intra-abdominal desmoids and liver failure.
The cause of death was directly due to an indication for ITx in 11 of the 12 deceased patients (91.7%) who were candidates because of liver failure or desmoids, and in five of the 13 deceased (38.5%) who were candidates because of the other indications (p=0.041) (table 3).
Cox regression model for the HR for death on home parenteral nutrition and causes of death on home parenteral nutrition, according to the indications for intestinal transplantation in candidates who completed the 5-year follow-up
Life-saving and pre-emptive or rehabilitative intestinal transplantation
According to the HRs for death and to the causes of death in patients on HPN observed for individual indications for ITx, the reasons for ITx candidacy were categorised as life-saving (liver failure or desmoids) or pre-emptive/rehabilitative (CVC-related complications or ultra-short bowel).
Among the 37 candidates for a life-saving ITx, the survival was 56% (CI: 38% to 75%) at 5 years in the 28 who remained on HPN and 19% (CI: 51% to 100%) at 2 years in the nine who underwent ITx (six with liver and three without liver) (p<0.001). Among the six who died after ITx, one was a re-transplant and three were in hospital at the time of calling for ITx.
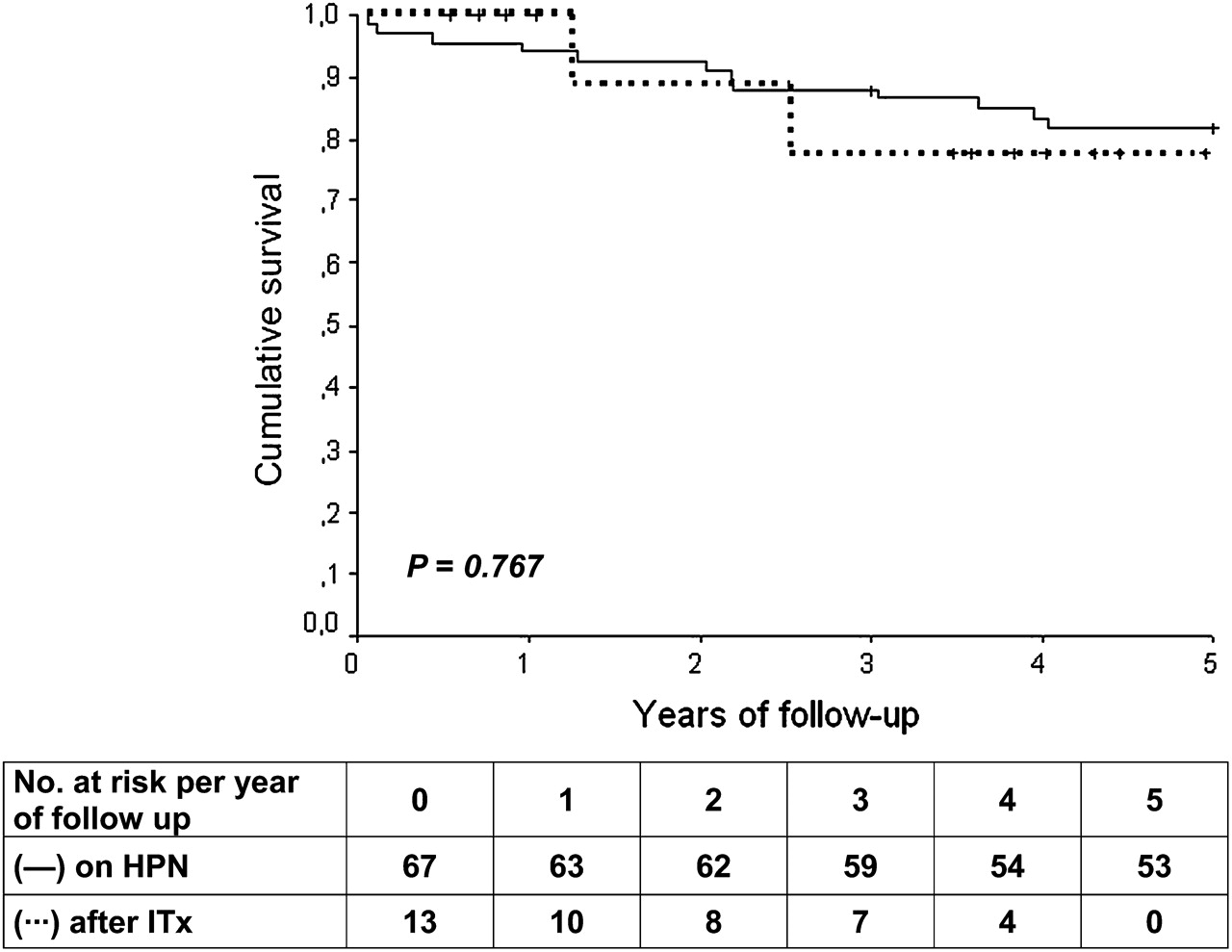
Among the 80 candidates for a pre-emptive/rehabilitative ITx, the 5-year survival was 83% (CI: 73% to 91%) in the 67 who remained on HPN, and 78% (CI: 51% to 100%) in the 13 who underwent ITx (all without liver and all at home at the time of calling for ITx) (p=0.767) (figure 5).
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Five-year survival rates (Kaplan–Meier analysis) on home parenteral nutrition (HPN) and after intestinal transplantation (ITx) in patients with irreversible intestinal failure candidates for ITx because of central venous catheter-related complications or ultra-short bowel who remained on HPN (—) or who underwent ITx (···).
Discussion
Prolonging the observation time from 3 to 5 years added weight to the confirmation of HPN as the primary treatment for irreversible IF, and helps to define the more appropriate relative roles for HPN and ITx. In agreement with previous results, in patients clinically stable on HPN, survival probability was greater and treatment-related death was less likely than that in ITx recipients, with a non-statistically significant better trend in children and adolescents.13–22 Three key observations emerge: (a) the mortality rate on HPN was higher during the first years after starting the treatment, when it was primarily related to the underlying disease, whereas in long-term survivors, mortality was mainly related to complications of HPN; (b) HPN/IF-associated liver disease or intra-abdominal desmoids were the only conditions associated with a statistically significant increased risk of death on HPN; (c) the survival probability of patients with CVC-related major complications or with ultra-short bowel who underwent timely ITx was similar to that of those who remained on HPN.
This survey is unique through the large number of patients enrolled and the characteristics of the study protocol, represented by its prospective design, the exclusion of patients with contraindication for ITx, the inclusion in the statistical analysis of only those patients deemed to have irreversible IF, and the evaluation of both adults and children. Furthermore, no criteria were adopted to select the HPN centres which participated in the study, in order to include centres with different level of experience, thus making the survey representative of the actual management of patients on HPN for chronic intestinal failure in Europe.2 The aim was to learn which indications for ITx were associated with an increased risk of death on HPN and if death was actually due to causes that could be rescued by an ITx. Patients with contraindications for ITx, who could have been at higher risk of death, were therefore excluded from this prospective study. They constituted 271 patients, 26% of whom had malignancy, organ failure or immunological deficiency and 41% were older than 65 years.2 This was not the case in previous retrospective studies, raising the suspicion that mortality on HPN could have been increased by risk factors other than IF or HPN.8 15–22 Patients who were weaned off HPN during the 5-year follow-up were excluded from the statistical analysis, which included only those patients who remained on HPN for at least five consecutive years, who were therefore deemed to have irreversible IF. The evaluation of both children and adults allows either the analysis of differences between the age categories and an appropriate comparison with case series of patients who underwent ITx, most of which did not analyse age categories separately.7 13 14 Even though a greater frequency of HPN/IF-associated liver disease and CVC-related complications in children than in adults could be expected, in our cohorts, the indications for ITx were mainly related to HPN-failure in adults and to the underlying disease in children.2 3 Indeed, the rate of HPN complications cannot automatically reflect the rate of patient referral for ITx, because only a fraction of patients with a HPN complication may have a progression of the diseases leading to an indication for ITx. The prevalence of HPN/IF-associated liver disease is estimated to be approximately 40–60% in infants and up to 85% in neonates who are receiving HPN for intestinal failure.23 However, only 15% of patients on long-term HPN eventually develop an end-stage liver disease, which leads to combined intestinal and liver transplant.24
The patient categorisation at baseline and the small number of those who underwent ITx during the follow-up have to be considered in the interpretation of the results. At baseline, patients were categorised according to the presence or absence of indications for ITx, objectively evaluated by the doctors in charge of the patients. Patient weaned off HPN as well as referral for ITx of those patients with an indication were not regulated by the study protocol, because no guidelines for intestinal rehabilitation and no objective criteria to prioritise patients for listing for ITx have yet been defined.9 This could have caused either a low referral rate or a referral of only those candidates with a more compromised clinical status and therefore at higher risk of death after ITx. However, notwithstanding the small number of patients who underwent ITx, the 5-year 54% survival rate observed in the whole group of ITx recipients, as well as the outcomes of recipients who were at home or in hospital at time of transplantation, were similar to the results reported by the USA United Network for Organ Sharing report13 and the International Transplant Registry.14 Furthermore, the 78% survival rate observed in the 13 patients who received an ITx without liver for CVC-catheter complications or ultra-short bowel, all of whom were at home at time of calling for ITx, is similar to the results observed in the most experienced centres in the USA.7
The risk of death decreased and the causes of death changed with time on HPN. These data confirm the observations from previous retrospective studies of survival on HPN, adding the information about the causes of death in relation to time on treatment. Overall only one third of deaths which occur on HPN were related to the treatment. The risk of death during the early years of HPN was mainly attributable to the underlying disease, whereas in long-term survivors, the risk due to HPN-related complications prevailed. This would imply a time-related indication for a life-saving ITx. In the early period after starting HPN, it could be required because of a high-risk underlying disease. The survival rate and the causes of death of patients entered in the study more than 2 years after starting HPN demonstrate that only a few long term survivors will need a life-saving ITx, and then mainly because of the development of HPN/IF-associated liver failure.
When the indication for ITx was HPN/IF-related liver failure or intra-abdominal desmoid there was an increased risk of death on HPN directly attributable to the indication for ITx. Therefore, these conditions are those for which a life-saving transplantation is justified. The survival rate observed in the nine patients with these indications who underwent ITx was lower than that reported in largest series.13 14 This could be due to the poor health status observed in four of them at the time of calling for transplantation, as three were hospitalised and one was waiting for a re-transplant. This confirms clinical status as a major predictive factor for ITx outcome, and reinforces the recommendation for timely referral for life-saving transplantation in patients with HPN/IF-related liver failure or intra-abdominal desmoids.
CVC-related major complications, as described by Medicare, were not associated with a statistically significant increased risk of death on HPN. The RR of death was 2.08 in candidates because of CVC-related multiple deep vein thrombosis, but only three of the eight deaths which occurred in this group of patients were actually due to the indication for ITx. Furthermore, in candidates because of frequent/severe CVC-related sepsis the RR of death was 1.09 and the only one death which occurred in this group was not CVC-related (table 3). Considering that intractable infection is a main cause of death after ITx,9 our data definitively rule out frequent/severe CVC-related infection as an indication for ITx. Patients with ultra-short bowel or congenital mucosal disease showed a high survival rate on HPN, and no death on HPN was observed in candidates because of frequent and severe dehydration or high morbidity intestinal failure. Only one-third of deaths on HPN which occurred in patients with CVC-related major complications, ultra-short bowel or congenital mucosal disease were directly related to the indications themselves. For these reasons, they should not, alone, be considered indications for direct listing for life-saving ITx. A case-by-case decision is necessary, for which early referral to an experienced IF centre with medical, HPN, non-transplant and transplant surgery expertise is strongly recommended, and where the most appropriate treatment strategy can be devised. This should avoid both the development of life-threatening complications of HPN, as well as too late a referral for ITx as a consequence of suboptimal management.25
In patients with CVC-related major complications or ultra-short bowel, the survival rate in those who underwent ITx didn't differ from that in those remaining on HPN. In these conditions ITx could have a pre-emptive/rehabilitative role. The decision for referral for ITx should probably be based on a combination of cost and quality of life comparisons between HPN and ITx. These analyses were not addressed in the present study, which aimed to know survival and causes of death. At present, data on costs are lacking and only a few studies, using non-specific tools, have compared the quality of life on HPN and after ITx.26–28 The results show that quality of life is improved after successful ITx.28 However, in patients with these indications for ITx who died on HPN, death was related to the indications themselves in 38.5% of those who remained on HPN and to ITx complications in 100% of those who underwent transplantation. Furthermore, graft failure requiring HPN or retransplantation may occur in about 25% of ITx recipients.13 14 Therefore, studies comparing the cost-utility of HPN and ITx seem more appropriate than studies evaluating cost and quality of life separately.
In conclusion, our data: (a) confirm HPN as the primary maintenance therapy for IF; (b) indicate HPN/IF-associated liver failure or intra-abdominal desmoids as the only indications for a timely life-saving ITx; (c) indicate that CVC-related major complications as well as ultra-short bowel and congenital mucosal disease could be indications for a pre-emptive/rehabilitative ITx, depending on the results of cost-utility studies comparing HPN and ITx; and (d) suggest that in the early years of HPN a life-saving ITx could be required for some patients who are at higher risk of death related to the underlying disease.
Acknowledgments
We are grateful for the assistance given by our colleagues at the participating centres: Belgium A. Van Gossum, Brussels Denmark M. Staun, Copenhagen E. Hylander, Koege France F. Joly, B. Messing, Clichy D. Laharie, Bordeaux E. Lerebours, Rouen M. Gérard-Boncompain, Lyon J-L. Bornet, Toulouse M. Pagenault, Rennes P. Beau, Poitiers E. Fontaine, Grenoble C. Chambrier, P. Bouletreau, Lyon S. Schneider, X. Hébuterne, Nice F. Gottrand, Lille V. Colomb, O. Goulet, Paris Germany P. Thul, Berlin Italy L. Pironi, E. Lanzoni, Bologna L. Gallitelli, Paderno-Dugnano C. Gavazzi, Milan G. Chiavenna, Lecco E. Limido, Busto-Arsizio L. Santarpia, F. Contaldo, Naples P. Orlandoni, Ancona P. Gandullia, Genova M. Gambarara, M.S. Basso, Rome FW. Guglielmi, Bari D. De Francesco, A. Palmo, Torino M. Candusso, Bergamo Poland M. Lyszkowska, Warsaw Spain M. Planas, Barcelona J M Moreno Villares, Madrid C. Cuerda, Madrid C. Pedron, Madrid L. Gomez, Barcelona Sweeden G. Kurlberg, Östra, Göteborg United Kingdom J. Baxter, Dundee A. Davidson, A. Forbes, Harrow J. M. Woodward, Cambridge
References
Footnotes
Competing interests None.
Ethics approval Not required. The questionnaire used in this study was completed for each individual patient by the local medical team in anonymised form, codified for linkage with previous years' data. The research was thus based on information taken from that already present in the patient records at the time of the data collection. The study was conducted with full regard to confidentiality and protection of the individual patient.
Provenance and peer review Not commissioned; externally peer reviewed.