Article Text

Abstract
Objective Neonatal sepsis is a major cause of neonatal deaths in Asia but data remain scarce. We aimed to investigate the causative organisms and antibiotic resistance in neonatal care units in China, Malaysia, Hong Kong and Thailand.
Methods Prospective cohort study of neonatal sepsis defined as positive culture of a single potentially pathogenic organism from blood or cerebrospinal fluid differentiated into early-onset sepsis (EOS) occurring <3 days of birth and late-onset sepsis (LOS) ≥3 days after birth.
Results During the study period, there were 963 episodes of neonatal sepsis. The incidence of EOS was 0.62 (95% CI 0.45 to 0.82) per 1000 live births or 4.91 (95% CI 4.22 to 5.68) per 1000 admissions while the incidence of LOS was 5.00 (95% CI 4.51 to 5.53) per 1000 live births or 21.22 (95% CI 19.79 to 22.77) per 1000 admissions. The incidence of Group B Streptococcus (GBS) sepsis was low but remained the most common single pathogen for EOS among inborn babies. Klebsiella spp. was the most common Gram-negative organism causing most deaths. The case-fatality was 7.0% (95% CI 3.9% to 12.0%) for EOS and 16.0% (95% CI 13.7% to 19.0%) for LOS, and was significantly different between participating units after adjusting for potential confounders. Of all Gram-negative organisms, 47%, 37% and 32% were resistant to third-generation cephalosporins, gentamicin or both, respectively.
Conclusions The pattern of EOS in Asian settings is similar to that in industrialised countries with low incidence of GBS sepsis. The important features of neonatal sepsis in Asia are the burden of Klebsiella spp. and high level of antibiotic resistance. These should be addressed while developing measures to reduce neonatal mortality due to infection.
Statistics from Altmetric.com
-
In recent years, there was substantial reduction in under-five mortality but neonatal mortality remained practically unchanged and its contribution to under-five mortality is increasing.
-
Neonatal sepsis is a major cause of neonatal mortality and hindered achieving the fourth Millennium Development Goal.
-
Identifying incidence, causative organisms and antibiotic resistance of neonatal sepsis are essential to reduce neonatal mortality particularly in Asia where most neonatal deaths occur.
What this study adds
-
Similar to developed countries, the incidence of GBS sepsis is low in Asian units but remained a major contributor to EOS sepsis.
-
Sensitivity of Klebsiella should be considered in the initial management of sepsis because it caused most Gram-negative infections and one third of deaths.
-
Non-fermenting Gram-negative bacteria like Pseudomonas and Acinetobacter are emerging as important pathogens in Asian neonatal care units.
Introduction
The fourth Millennium Development Goals (MDG-4) aimed to improve child survival and reduce under-5-year-old mortality by two-thirds by 2015. To achieve this goal, efforts have focused on vertical programmes to reduce pneumonia, diarrhoea, malaria and vaccine-preventable conditions, which are all important causes of death after the neonatal period, and as a result, a remarkable reduction in under-five mortality occurred but little progress was made on neonatal mortality which accounts for 38% of all deaths among children under-5 years.1 Instead the proportion of child deaths in the neonatal period is likely to increase and hence further reduction of under-five mortality requires substantial reduction in neonatal mortality. In areas with very high neonatal mortality, almost 50% of deaths are due to severe infections,1 so a substantial reduction in neonatal infection will be essential to meet MDG-4, particularly in South-East Asia, a region where most deaths in the neonatal period occur.
Neonatal sepsis may be classified according to the time of onset into early-onset sepsis (EOS) and late-onset sepsis (LOS) which has clinical importance. EOS is acquired before or during delivery and is caused mainly by microorganisms from the maternal genital tract, while LOS is primarily due to organisms acquired after delivery and considered nosocomial or community-acquired infections. As a result, the spectrum of organisms causing EOS differs from that causing LOS, a trend that becomes most obvious 48 h after birth.2 Group B Streptococcus (GBS) is a common cause of EOS in industrialised countries, although its burden has been reduced substantially in areas where intrapartum antibiotic prophylaxis (IPAP) has been implemented3–7 while Gram-positive bacteria mainly Coagulase-negative staphylococci (CONS) are the most common cause of LOS in industrialised and developing countries.8–12
Surveillance of organisms causing neonatal sepsis, which may differ from one place to another, and in the same place over time, and of their antimicrobial sensitivities can guide the appropriate empirical treatment and help develop cost-effective interventions to prevent neonatal deaths where they are needed most. While this essential information is collected and updated regularly in developed countries, data remain scarce from Asian countries, where most neonatal deaths occur. This study aimed to investigate the incidence of EOS and LOS and describe the spectrum of the causative organisms and their antimicrobial resistance in four Asian neonatal care units.
Methods
Four neonatal care units participated in a prospective surveillance study and collected data on neonatal sepsis using a standardised data collection form. Data collection was from 1 January 2006 to 31 December 2009 inclusive in Kuala Terengganu in Malaysia (KT-Malaysia) and Centro Hospitalar Conde de Sao Januario in Macau (CHCSJ-Macau) while from 1 January 2007 to 31 December 2009 in Hat Yai Hospital in Thailand (HYH-Thailand) and Children's Hospital of Hebei Province in China (CHHP-China). The online supplementary table S1 shows the number of live births in each hospital and the neonatal mortality rate in areas where the hospitals serve.
Neonatal sepsis was defined as the growth of a single potentially pathogenic organism (bacterium or fungus) from blood or cerebrospinal fluid in infants with clinical and laboratory findings consistent with infection.13 EOS was defined as an infection among infants younger than 3 days while LOS among infants 3 days of birth or older. Likely contaminants were excluded by clinical judgment. The isolated organism from blood and their susceptibility or resistance to antibiotics were recorded using recognised methods of antibiotic susceptibility testing but this was not standardised between the different sites. In particular, the sensitivity of Gram-negative bacilli to the third-generation cephalosporins (cefotaxime or ceftazidime) and to gentamicin was recorded. Sensitivity of Staphylococcus aureus to methicillin was also tested. In KT-Malaysia resistance of Gram-negative organisms to imipenem and amikacin was also recorded. Data were collected on gestational age, birth weight, sex, the age (in days) at which the positive blood culture was obtained, and whether the baby was born in the hospital (intramural admission) or outside the hospital (extramural admission). Data on the number of admissions to the neonatal units were also collected in addition to the number of live births if the unit is attached to a maternity unit (only in KT-Malaysia, HYH-Thailand and CHCSJ-Macau).
Data were analysed using Stata V.8 (Stata Corp., College Station, Texas, USA). The incidence of EOS and LOS was calculated by dividing the number of inborn infants with sepsis by the number of live births in the hospital. Except for the unit in CHHP-China, data on live births were available from all units. Rates of EOS and LOS were also calculated by dividing the number of infants (inborn or outborn) with sepsis by the number of infants admitted to the same unit. The 95% CI were calculated using the Poisson distribution. The χ2 test was used to evaluate the differences in proportion, while χ2 for linear trend was used to test for trends in the incidence of neonatal sepsis over the study period. Multivariate unconditional logistic regression was used to investigate the differences in mortality between different units while adjusting for potential confounders such as type of organism and birth weight. The study was approved by the Research and Development Ethics Committee of the Royal Alexandra Hospital for Children (Project 2005/020).
Results
During the study period, there were 963 neonatal infections, of which 345 (35.82%) occurred in KT-Malaysia, 459 (47.66%) in CHHP-China, 143 (14.85%) in HYH-Thailand and 16 (1.66%) in CHCSJ-Macau. Out of 963 neonatal infections, 433 (44.96%) occurred among inborn and 530 (55.0%) among outborn babies and 181 were EOS while 782 were LOS (≥3 days of birth). Although five infections occurred among inborn infants in CHHP-China, all neonatal infections in CHHP-China occurred among extramural admissions. The yearly incidence of overall neonatal sepsis, EOS and LOS out of live births in the units attached to maternity wards (KT-Malaysia, HYH-Thailand and CHCSJ-Macau) is shown in table 1. The overall incidence of neonatal sepsis among inborn infants out of live births in these three units was 5.62 (95% CI 5.10 to 6.17) per 1000 live births while the incidence of EOS and LOS was 0.62 (95% CI 0.45 to 0.82) and 5.00 (95% CI 4.51 to 5.53) per 1000 live births, respectively. The incidence of EOS did not differ significantly between the three units (p=0.08) and did not change over the study period (p=0.11) while the incidence of LOS was significantly different between the three units (p<0.001) and declined significantly over the study period, particularly in KT-Malaysia (p<0.001).
Incidence of early-onset sepsis (EOS) (<3 days of birth) and late-onset sepsis (LOS) (≥3 days of birth) among inborn infants out of 1000 live births in three Asian centres, 2006–2009
We calculated the incidence of neonatal sepsis for admissions including infections among inborn and outborn babies using the data from the unit in CHHP-China (table 2). The incidence of overall neonatal sepsis for admissions in all units was 26.14 (95% CI 24.51 to 27.84) per 1000 admissions while the incidence of EOS and LOS was 4.91 (95% CI 4.22 to 5.68) and 21.22 (95% CI 19.79 to 22.77) per 1000 admissions, respectively. The incidence of EOS and LOS was significantly different between units even after stratification by birth weight (see online supplementary table S2). The incidence of LOS declined significantly over the study period, particularly in KT-Malaysia (p<0.001).
Incidence of early-onset sepsis (EOS) (<3 days of birth) and late-onset sepsis (LOS) (≥3 days of birth) among inborn and outborn infants out of 1000 admissions in four Asian centres, 2006–2009
Spectrum of organism causing EOS and LOS
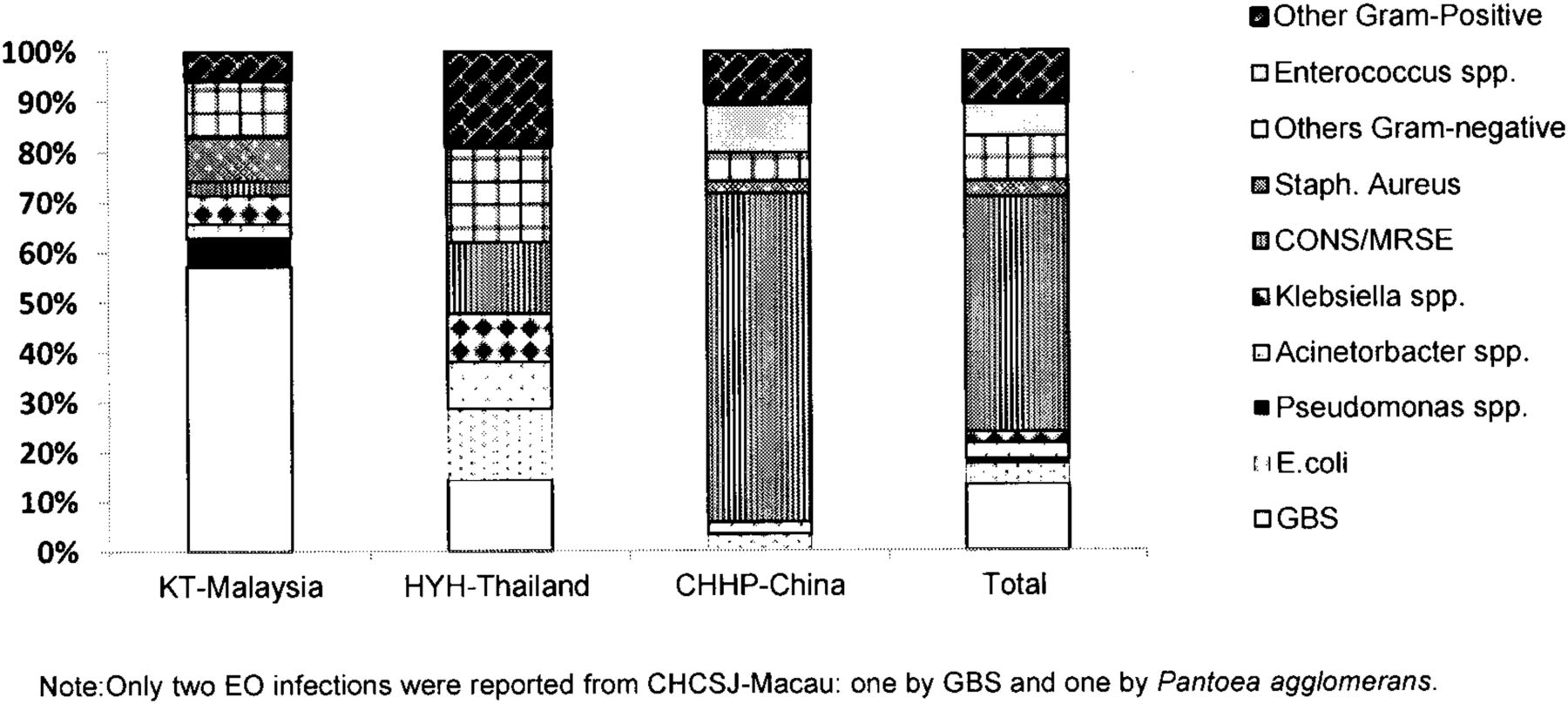
The spectrum of organisms causing EOS in different study sites is shown in figure 1. GBS infection was more common in KT-Malaysia compared to CHHP-China or HYH-Thailand. Twenty of 35 EO infections in KT-Malaysia, were due to GBS while none of 123 EO infections in CHHP-China, were due to GBS. In HYH-Thailand only three (14.3%) EO infections were due to GBS. The incidence of GBS infection (whether EOS or LOS) among inborn infants was 0.41, 0.47, and 0.14 per 1000 live births in KT-Malaysia, CHCSJ-Macau and HYH-Thailand, respectively (p>0.05). Escherichia coli caused no EO infections in KT-Malaysia while it accounted for three (14.3%) infections in HYH-Thailand and four (3.2%) in CHHP-China. CONS accounted for 81 (65.8%) EO infections representing the commonest cause in CHHP-China while, only one and three EO infections were due to CONS in KT-Malaysia and HYH-Thailand, respectively. All Gram-negative organisms accounted for 33 (18.2%) of EO infections, which did not change significantly during the study period (p=0.6). The incidence of Gram-negative infection among inborn babies in the three units (KT-Malaysia, HYH-Thailand, CHCSJ-Macau) was 0.22 per 1000 live births and did not change significantly over time (χ2 for trend p=0.2). One case of Listeria monocytogenes was reported from KT-Malaysia and one case of Salmonella spp. was reported from CHHP-China. One case of Morganella spp. was reported from HYH-Thailand. Only two EO infections were reported from CHCSJ-Macau between 2006 and 2009: one by GBS and the other by Pantoea agglomerans.
{kind=link}
Spectrum of organism causing early-onset neonatal sepsis (<3 days of birth) in four Asian centres.
The spectrum of organisms causing LOS is shown in table 3. CONS was the most common cause of LOS in KT-Malaysia, HYH-Thailand and CHHP-China. All Gram-negative bacteria accounted for 281 (35.9%) of LO infections which did not change significantly over time (p=0.14). This was 159 (51.3%) in KT-Malaysia, 56 (45.9%) in HYH-Thailand, six (42.9%) in CHCSJ-Macau and 59 (17.6%) in CHHP-China (p<0.001). Despite the unit in CHCSJ-Macau, Klebsiella was the most common Gram-negative organism, and accounted for more than 40% of LOS Gram-negative infections in each unit. Pseudomonas and Serratia accounted for more infections in KT-Malaysia than in any other study site (table 3).
Organisms causing late-onset neonatal sepsis (≥3 days of birth) in four Asian centres, 2006–2009
Case-fatality
Out of 963 neonatal infections, 140 (14.5%, 95% CI 12.4% to 16.9%) died from infection (table 4). Of 181 EOS, 13 (7.2%, 95% CI 3.9% to 12.0%) died from infection and out of 782 LOS, 127 (16.2%, 95% CI 13.7% to 19.0%) died from infection. Case-fatality of sepsis was 99 (28.7%) in KT-Malaysia, 21 (14.5%) in HYH-Thailand, 18 (3.9%) in CHHP-China and two (12.5%) in CHCSJ-Macau (p<0.001). Case-fatality was significantly higher in KT-Malaysia for each Gram-positive (p<0.001) and Gram-negative (p<0.001) compared to other sites. Overall case-fatality remained significantly higher in KT-Malaysia after adjusting for the type of organism, gestational age and birth weight.
Case-fatality of specific pathogens among infants with neonatal sepsis in four Asian centres
Antimicrobial resistance
Resistance of Gram-negative organisms to third-generation cephalosporins, gentamicin or both is shown in table 5. Sensitivity to third-generation cephalosporin and gentamicin was recorded for 285 (91%) of all isolated Gram-negative organisms. Overall 47%, 37%, and 32% of all Gram-negative organisms were resistant to third-generation cephalosporins, gentamicin or both, respectively. This showed significant differences between the study sites, table 5. Resistance of all Gram-negative organisms to Gentamicin or third-generation cephalosporin was not significantly different between inborn and outborn babies, p=0.84 and p=0.06, respectively.
Antibiotic resistance of the main Gram-negative organisms causing early-onset and late-onset neonatal sepsis in four Asian centres
In KT-Malaysia, out of 70 Gram-negative infections that were tested for Amikacin, 21 (30%) were resistant, table 6. Similarly out of 96 Gram-negative organisms tested for imipenem, seven (7%) were resistant. Only one of 54 Gram-negative organisms tested for meropenem was resistant (data not shown). As mentioned above, 16 (5.2%) of neonatal infections were attributed to methicillin-resistant Staphylococcus aureus (MRSA) which represent 52% of infection by S aureus in this study site, table 3. All MRSA were sensitive to vancomycin in KT-Malaysia. One of 15 GBS infections tested, was reported as resistant to ampicillin and none of 26 tested was resistant to penicillin, while 60% of E coli was resistant to ampicillin (47 tested).
Resistance to Amikacin and imipenem among Gram-negative organisms causing neonatal infections in KT-Malaysia
Discussion
This study aimed to investigate the incidence of neonatal sepsis and describe the main causative organisms and their antibiotic resistance in four Asian study sites. While the incidence of GBS infection was low in KT-Malaysia and CHCSJ-Macau (0.42 per 1000 live births), GBS remained the main cause of EOS in these units among both inborn and outborn babies, causing more than half of EO infections. The profile of EOS in KT-Malaysia and CHCSJ-Macau seems to be similar to that reported recently from USA, where the incidence of GBS was low but remained the most frequent EOS pathogen.14 ,15 However, the role of E coli seems to be less obvious in these two units compared to other developed settings.14 ,16 IPAP against GBS should be strengthened and audited in KT-Malaysia and CHCSJ-Macau and the risk-based strategy can be used if low incidence is used as an argument against implementing the screening programme. The burden of GBS in CHHP-China seems to be low as not a single EO or LO infection was due to GBS during the study period. GBS is reported to be a rare cause of EOS in Asia and other developing countries,17 although this has been recently challenged18 and GBS being reported as a major pathogen in developing countries.19 ,20 Approximately, 18% of EOS was due to Gram-negative organisms which did not change significantly over time nor the incidence of Gram-negative infection changed during the study period which is consistent with the recent findings from USA that Gram-negative infections are no longer increasing.14
CONS was the most common organism for LOS, which is similar to that previously reported in Asian countries12 and developed countries.8–11 The predominance of CONS in Latin America, the Middle East and South East Asia had been attributed to adoption of sophisticated tertiary care without strict measures against infections.21 ,22 However, there is significant disagreement between different centres in considering CONS as a true infection or a contaminant. In a recent multicentre study in the USA, some centres considered all CONS as true infections, whereas others considered them all contaminants.14 In a hospital-based study in Canada7 and in a population-based surveillance in Florida,23 CONS were reported as the most common pathogen for EOS. In CHHP-China, the spectrum of organisms causing neonatal sepsis has a distinctive pattern with CONS being the main pathogen for EOS and LOS. CONS are likely to be true pathogen in preterm infants especially those with a central catheter.24 ,25 Although the proportion of low birth weight (LBW) among admitted infants was three times higher in CHHP-China than other units, it cannot explain the predominance of CONS in this unit, as most infections in this unit occurred among admitted infants with normal birth weight (see online supplementary table S2). It is likely that the different pattern of neonatal sepsis in this unit is due to blood culture contamination. However, we support the recent calls to investigate the role of CONS, particularly in EOS and whether they are emerging as an important pathogen.14
Approximately 36% of LOS were due to Gram-negative organisms. Despite the unit CHHP-China which had lower burden of Gram-negative infections, approximately half of LOS was due to Gram-negative organisms which is similar to that reported previously.12 Similar to that reported from Eastern26 and South India27 and Kuwait,22 Klebsiella was the most common Gram-negative organism causing LOS. Non-fermenting Gram-negative bacteria like Pseudomonas and Acinetobacter have also contributed to neonatal sepsis, being particularly prevalent in KT-Malaysia. Surprisingly, for four consecutive years, there was no EOS or LOS due to Klebsiella in CHCSJ-Macau. While MRSA was an important pathogen for EOS and LOS in KT-Malaysia, there was no infection by MRSA in HYH-Thailand or CHSC-Macau. Such striking differences may be attributable to different discharge policies but suggest that surveillance and policies for neonatal sepsis is required at local level and generalisation of findings to wider geographical areas is not always appropriate.
Case-fatality for EOS was similar to that reported previously from Asian countries12 ,20 but lower than that reported recently from the USA.14 Klebsiella (mainly K pneumoniae) was responsible for approximately one third of all deaths caused by LOS. The case-fatality of Gram-negative infections was significantly higher in KT-Malaysia compared with other units, even after adjusting for LBW and prematurity, which may require a review of the current practices to achieve timely initiation of appropriate antibiotic therapy.
Similar to that previously reported from Asian units,12 approximately half of Gram-negative organisms were resistant to third-generation cephalosporins and more than one third were resistant to gentamicin while one third were resistant to both. This was significantly different between study sites, being particularly high in HYH-Thailand where more than 60% of Gram-negative organisms were resistant to both third-generation cephalosporin and gentamicin. Approximately 62%, 45% and 41% of Klebsiella infections were resistant to third-generation cephalosporin, gentamicin or both, respectively. Although this is similar to that previously reported,12 ,21 ,28 it is worrying as Klebsiella infection was common pathogen and caused most deaths. Consistent with the recent reports from China,29 imipenem remained strongly active against Klebsiella in KT-Malaysia, where no isolate was resistant to imipenem (48 tested). Of particular concern, more than 42% of E coli were resistant to gentamicin although penicillin and gentamicin continue to be the recommended treatment for infants with suspected EOS in Asian countries. E coli was not a major cause of EOS in KT-Malaysia and CHCSJ-Macau compared to developed settings14 ,16 but their resistance to gentamicin seems to be higher than that reported from developed countries.14 In Asian settings, sensitivity of Klebsiella to various antibiotics should be a major determinant of the recommended initial management of infants suspected with sepsis since it is common and causes most deaths.
Our findings may lack generalisability, because the units reporting data are likely to be better resourced than other Asian units. Tertiary units may also attract high number of pre-term infants and urban patients of high socioeconomic status, and thus the data may not represent neonatal sepsis at the community level. However, the data provide valuable information on various aspects of neonatal sepsis in Asia including antimicrobial resistance. The data may help to build a platform of knowledge for preventive interventions to reduce neonatal mortality hence improve child survival.
In conclusion, despite the unit in CHHP-China, the data we obtained showed similar pattern of EOS in Asian units to that in developed countries. The incidence of GBS sepsis was low but remained a major contributor to EOS suggesting the need to strengthen IPAP. The spectrum of organisms causing EOS and LOS highlights the importance of Klebsiella as the most common Gram-negative infection, responsible for one third of deaths due to sepsis. Initial management of infants with suspected infection should take into account the sensitivity of Klebsiella in local settings. The emergence of non-fermenting Gram-negative bacteria like Pseudomonas and Acinetobacter as important pathogens, in addition to higher rates of MRSA infection in Asian units, is of great concern and requires longitudinal surveillance to monitor the varied pathogens and their changing antibiotic susceptibility patterns.
References
Supplementary materials
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Files in this Data Supplement:
- Data supplement 1 - Online tables
Footnotes
-
Contributors AT drafted the paper, analysed the data, contributed to all aspects of the study. MH contributed in the study design and data analysis and revised the paper for important intellectual content. LC contributed to the study design and data collection and revised the paper for important intellectual content. JL contributed to the study design and data collection and revised the paper for important intellectual content. KL contributed to the study design and data collection and revised the paper for important intellectual content. NN contributed to the study design and data collection and revised the paper for important intellectual content. DI study design, data interpretation and revision of the paper for important intellectual content.
-
Competing interests None.
-
Provenance and peer review Not commissioned; externally peer reviewed.