Article Text

Abstract
Objective To measure nursing workload and timely completion of essential tasks in relation to the staffing levels recommended by the British Association of Perinatal Medicine (BAPM) in Staffordshire, Shropshire and Black CountryNewborn Network.
Methods A prospective observational study was conducted measuring the time taken by selected nurses to undertake the necessary tasks for babies receiving different levels of care in the Network's six constituent neonatal units. An independent observer was used. The unit and individual's workload was evaluated against BAPM standards. Delays in essential predetermined tasks were recorded. The impact on quantity of care given and on the number of delayed tasks were compared between those with the recommended workload or less and those overstretched.
Results Between October 2008 and February 2009, 89 nurses were observed caring for 244 neonates over 534 h. 54% of nursing shifts failed to meet BAPM standards. Nurses with workload greater than the BAPM-recommended levels demonstrated a 28% decrease in median time spent on clinical care per baby. 92 (17%) essential tasks were delayed >1 h or not done. Delays/omissions were more likely when BAPM standards were not met (53% vs 40%, p=0.049). In nursing observations without delays/omissions, accommodating for adequate nursing breaks and working in the same area, nurses could cater for no more than 1.2, 1.5 and 2.7 babies in intensive care, high dependency care and special care, respectively.
Conclusion Understaffing leads to measurable problems including delays to essential treatment and reduced clinical care. BAPM standards are not aspirational and should be regarded as a minimum. Further research on optimising nursing care efficiency with limited nursing resources is necessary.
Statistics from Altmetric.com
Introduction
Reductions to the threshold of viability and increasing survival of extremely premature newborns contribute to increasing neonatal workload in the UK.1 These gains have been achieved despite ongoing neonatal nursing shortages in the National Health Service,2 which have been assessed against defined standards for neonatal nursing care provision.3 Despite these standards being outlined by the British Association of Perinatal Medicine (BAPM) and adopted by the Department of Health (DOH),4 most UK neonatal units do not achieve them consistently. This raises the issue whether the standards are an unrealistic expectation or necessary to provide safe, high-quality care.
What is already known on this topic
▶ British Association of Perinatal Medicine (BAPM) and Department of Health recommendations for neonate:nurse ratios for providing care in intensive care (IC), high dependency care (HDC) and special care (SC) in England are currently 1:1, 2:1 and 4:1, respectively.
▶ Neonatal units are generally understaffed and do not meet the standards set.
What this study adds
▶ The SSBC Newborn Network bears a significant burden of staff shortages in IC and SC especially.
▶ These shortages compromise time spent on clinical care, especially in the IC unit. When these shortages occur, significantly more delays and omissions in essential nursing care occur.
▶ Optimal neonate:nurse ratios for the Staffordshire, Shropshire and Black Country Newborn Network are 1.2:1 in IC, 1.5:1 in HDC and 2.7:1 in SC. BAPM standards are not aspirational, but a minimum requirement.
In 2007, the neonatal nursing teams from the Staffordshire, Shropshire and Black Country Newborn Network (SSBCNN) raised an awareness that the neonate-to-nurse ratios were failing to achieve BAPM recommendations and were placing increasing pressure on nursing work. They argued that neonatal workload tool assessments, illness scores, neonatal outcomes5 and quantification of nurse:neonate ratios indirectly reflect the workload of the individual nurse, but fail to quantify the burden placed on the individual nurse. This burden is influenced by many factors including level of experience, critical thinking and overall ward/administrative responsibilities. We therefore attempted to objectively evaluate nursing workload in the context of current staffing. We attempted to understand the actual workload per nurse during a 6-h period of observation and to assess whether staffing ratios currently in existence allowed for adequate nursing care provision. For the purposes of the study, this was defined by whether essential nursing tasks were delayed or omitted due to excessive workload. A secondary aim was to gain some understanding of what nurses ought to be able to achieve in a given period of time, under normal circumstances.
Method
A prospective observational study was conducted between 8 October 2008 and 6 February 2009 at the six neonatal units in the SSBCNN. An independent senior neonatal nurse conducted nurse observations for three non-consecutive weeks per unit. Each observation lasted 6 h and commenced at 07:00–08:00, 12:00–14:00 or 18:00–21:00. By sampling shifts at different times of the day, we hoped to limit bias due to variations in unit activity and staffing ratios. As a single observer was used, we considered 6 h to be a reasonable time for the continuous nurse observations.
Selection of nurses for observation
As the qualified in specialty (QIS) trained and non-trained nurses on duty varied each day, on the first day, the first named nurse on the duty roster was selected (in the category of QIS trained or non-trained); on the second day, the second named nurse on duty was selected, and so on, going back to the beginning if there were more days than named nurses on duty to select from. With this, we hoped to eliminate oversampling of individual nurses. For the level 3 units, QIS-trained nurses were observed for 2 of the 3 weeks and a non-trained nurse for 1 of the 3 weeks; this was the opposite for level 1 and level 2 units.
Comparison of workload with BAPM recommendations
Workload in the observed units
Neonatal unit team leader interview provided information on unit staffing and level of care required, based on BAPM-defined criteria,3 for intensive care (IC), high dependency care (HDC) and special care (SC).
Nursing workload
Nursing staff and neonatal caseload were compared with BAPM/DOH3 4 recommended standards for staffing (one neonate per nurse for babies requiring IC, two per nurse for HDC and four per nurse for SC). Nursing workload was calculated as:

Shifts that exceeded 100% were considered to have excess nursing workload.
Workload of observed nurse
The number of neonates cared for by the nurse at each level of care and the time taken for nursing activities were recorded. This was done using a published taxonomy of nursing tasks6 and included direct and indirect clinical care, administration and staff breaks. Direct clinical care referred to essential care such as observations, administering drugs and feeds. Indirect nursing care referred to supporting activities such as parent craft. All tasks were recorded to the nearest next minute by reference to a wall clock; a stopwatch was not used as it was thought to be too intrusive and impossible to record overlapping tasks.
Comparison with BAPM standards
Nursing workload was analysed as (1) nurses who had ≤BAPM-recommended number of neonates to care for (adequately staffed) and (2) those who had more neonates to care for than that recommended by BAPM (underresourced).
Quality of nursing care provided
Delays/omissions in scheduled tasks were recorded as an indicator of the quality of care provided. At the start of each shift, the handover between the nurse completing and the ‘observed nurse’ starting the shift was observed. The observer highlighted essential tasks that were scheduled for the baby for the next 6 h: (1) respiratory rate, heart rate, temperature and blood glucose monitoring, (2) neonatal body cleansing/'all cares', (3) preparation/administration of feed, (4) medications and (5) intravenous cannulation sites observations. The observer then recorded whether these scheduled tasks were (1) completed within the hour of being scheduled, (2) delayed for more than an hour but completed or (3) omitted during period of observation. Delays >1 h and omissions were correlated with caseload and nursing breaks.
What can a nurse achieve in a given period of time?
We used data from nurses without delays >1 h/omissions in scheduled tasks, nursing neonates in a single area of care as the standardon which the achievable caseload per nurse could be defined.
Analysis
Data were analysed using Excel and SPSS version 13.0 packages. Pearson χ2 and Mann–Whitney tests were used as appropriate. The level of statistical significance was set at p<0.05 using two-tailed comparisons.
Study approval
Approval was obtained through each of the participating hospital's Audit Department.
Results
Neonatal workload
Workload in the observed units
A total of 1155 neonates were attended to by 430 nurses in 89 shifts, during the 18 weeks of observation. Of all nurses working, 64.4% (277.5) were trained in QIS. During the study period, there were 21 new admissions to IC/HDC, 12 transfers and 23 (25.8%) staff on overtime duty.
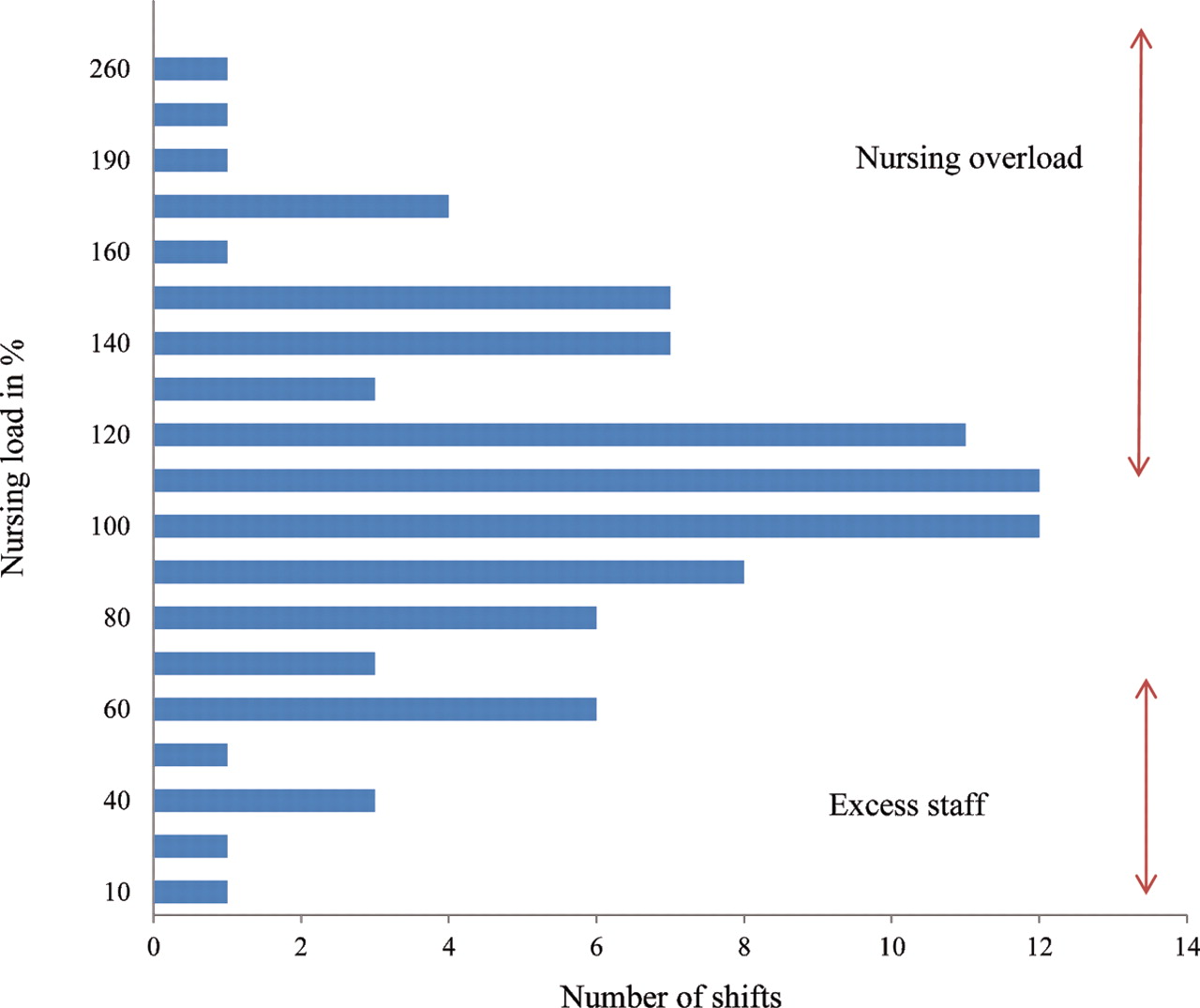
Variation in neonate:nurse ratio was observed across all grades of care, including up to 3:1 in IC and 13:1 in SC (figure 1). In IC and SC, median neonate:nurse ratios exceeded BAPM requirements. Better distribution of nursing support was observed in HDC and was due to more non-QIS staff being allocated to HD shifts than to IC (n=46/149 (31%) vs n=14/107 (13%), p≤0.001). In 54% (48/89) of shifts observed, nursing workload exceeded BAPM recommendations; in 13.5% (12/89), the Network had more nurses than recommended for its caseload (figure 2). There was no statistically significant difference between the proportion of night versus day shifts with excessive nursing workload.

Neonate:nurse ratio in special care (SC), high dependency care (HDC) and intensive care (IC) in the SSBC Newborn Network. X-axis denotes shift observed (n=89); Y-axis denotes number of neonates looked after per nurse in the designated area. The horizontal line represents the BAPM-recommended neonate:nurse ratio for the area. This was 4:1 for SC, 2:1 for HDC and 1:1 for IC. The area above the horizontal line represents shifts in which BAPM/DOH-recommended standards of nursing ratios were exceeded. BAPM, British Association of Perinatal Medicine; DOH, Department of Health.

Nursing load in SSBC Newborn Network: Definition of nursing load is given in the methods. Nursing workload >100% indicates shifts that had more babies to cater for based on the number of nurses present (QIS trained and non-trained) rather than the number recommended by BAPM/DOH; <70% indicates shifts that were staffed in excess of BAPM recommendations. BAPM, British Association of Perinatal Medicine; DOH, Department of Health; QIS, Qualified in Specialty.
Workload of observed nurse
From this cohort, 89 nurses caring for 244 neonates were observed over 534 h. One hundred and seventy neonates receiving SC, 41 receiving HDC and 33 receiving IC were cared for. Four nurses provided cover across two areas (two between IC/HDC, one between IC/SC and one between HD/SC). Excluding these cases, the median neonate:nurse ratio for the observed nurses in IC was 2:1 (range 1.3:1–3:1), HDC 2:1 (range 1.3:1–4:1) and SC 3: 1 (range 1.5:1–6:1); 42/55 nurses in SC, 10/15 in HDC and 5/19 in IC worked in areas that were adequately staffed, and the remainder, worked in areas that were underresourced for the shift.
Quality of care
Time spent on nursing activity
The median time spent per category of care was highest in IC and least in SC (table 1) and decreased proportionately as the number of neonates cared for by the nurse increased across all levels of care (figure 3). Time spent on staff breaks was significantly underachieved. In a 6-h cycle, 40 min were allocated to staff breaks, resulting in a total of 3560 min in 89 nurses observed. Of this, only 1789 min were taken as break, representing 50.3% less time than allocated. It was found that 76/89 (85%) nurses did not achieve the standard of 40-min break per cycle of observation. In this group, the median time taken for breaks was 12 min. No significant difference was found between nurses not taking breaks while working in SC, HDC or IC, or QIS status.

{kind=link}
{kind=link}
{kind=link}
Relationship between time taken on direct and indirect clinical care and number of babies cared for by nurse. Total time spent on each baby was highest in intensive care, then high dependency care and least in special care. When normalised to the nearest whole number of babies a nurse cared for, the total time on direct and indirect clinical care decreased as the number of babies per nurse increased; this occurred across all levels of care.
Proportion of time taken for nursing activities across different levels of care in the SSBC Newborn Network
The median time spent on clinical care per neonate in nurses working in underresourced areas (n=32) was 28% less than the time spent on care in adequately staffed areas (n=57). In IC, this was statistically significant.
When neonate:nurse ratios fell short of BAPM recommendations in IC, there was statistically significantly less time spent on tasks such as ventilator care and paying attention to alarms (table 2). Nursing activities such as cleansing, drug administration and record keeping were not affected by the caseload. Where there was adequate staffing, more time was spent teaching other staff in HDC/IC; this did not reach significance.
Median time in minutes spent on clinical care (direct and indirect care) in nurses who worked in underresourced and adequately staffed areas by British Association of Perinatal Medicine standards
Delays and omissions in scheduled activity
Ninety-two (17%) episodes of observed scheduled activities were delayed >1 h (n=50) or not done (n=42) within the observation time. These episodes occurred in 40 different nurses, representing delays/tasks not undertaken in 45% of nurses observed. The delays/omissions occurred in 43% of nurses working in SC, 29% in HDC and 71% in IC. In IC, nurses with delays in scheduled activities spent an average of 43 min longer on clinical care per baby than those who had no delays. More delays/omissions were observed in the early morning shift compared with the night shift (15/25 vs 16/45, p=0.049). Delays in individual neonates were more likely to occur when BAPM standards were not met than met (55/103 vs 57/141, p=0.045).
Of the 40 nurses who had delays/omissions, 849 of their entitled 1600 min (53%) were spent on staff breaks versus 940 min of the allocated 1960 min (48%) in the group of nurses who had no delays/omissions (p=0.519). Nurses who had delays/omissions had higher nursing ratios (0.3 neonates more to care for (p=0.189)) than nurses who did not have delays. No significant difference was found between delays/omissions in QIS and non-QIS nurses.
What should a nurse achieve in a given shift?
Of the nurses who did not have delays/omissions and nursing neonates in the same area, the average total time taken per baby was 125, 222 and 270 min, respectively in SC, HDC and IC. Staff breaks were an average of 7, 8 and 8 min, respectively. This then assumes that a nurse can cater for 2.9 in SC, 1.6 in HDC and 1.3 neonates in IC without significant delays but with suboptimal nursing breaks.
As the individual nurses cared for a variable number of neonates, but were still entitled to a 40-min break per shift observed, we adjusted for this as follows: in a 6-h shift, 320 min represented time for work on neonates, allowing 40 min for staff breaks. For SC, HDC and IC therefore, the average time spent on direct clinical care, indirect clinical care and administrative duties (excluding breaks) was 118, 214 and 262 min, respectively, per neonate. Based on this then, the optimum number of neonates that a nurse could care for without delays or omissions in tasks in a 6-h period, and taking a 40-min break, would be 2.7 (320/118) in SC, 1.5 (320/214) in HDC and 1.2 (320/262) in IC.
Discussion
This study shows that nursing staff spent less time on certain tasks predefined by us as being essential to quality of care when staffing ratios exceeded BAPM/DOH standards. More clinical work was done by the nurse; less time was available for direct patient care per baby and essential tasks were delayed or omitted when the workload and nursing ratios were higher. No significant difference was observed between delays/omissions in QIS and non-QIS trained nurses, suggesting that these cannot purely be assigned to inexperience or ability to think critically. That more than three quarters of the nursing workforce was not taking breaks adequately is of concern.7
In nurses where no delays/omissions were noted, BAPM/DOH staffing standards only just allow enough time to get all the tasks done in a shift in IC. It must be appreciated that even when BAPM/DOH standards are met on the unit, the individual nurse is likely to have to look after more babies in order to free up time for someone to manage the unit. For HDC and SC, nurses need to cater for fewer babies than defined by BAPM/DOH in order to complete all scheduled tasks set without significant delay. This finding supports recent suggestions that nurses in SC should care for two to three babies,6 and not four as recommended, and perhaps reflects the evolving nature of our neonatal clientele, with greater survival into HDC and SC of births on the threshold of viability.1 8 The practicality of this nursing ratio, in the current economic climate however, is unlikely. That our data did not find any significant difference in the care provided by QIS-trained and untrained nurses suggests that one avenue for future exploration could be increased utility of QIS-untrained nurses. These nurses could provide support either in SC or elsewhere, thus freeing up senior nurses to do more. The Gaussian distribution in figure 2 does indicate that there is room to improve nursing distribution per shift, if the Network nursing workforce functions as a single entity, with nurses moving between geographically clustered units as they are needed. Such an approach needs careful consideration, as this might not be well tolerated by nursing teams and could incur extensive travel costs if Network units are widely scattered.
In order to assess the validity of these low neonate:nurse ratios, the following questions must be considered: (1) were all the tasks undertaken necessary? (2) was the appropriate amount of time taken per task? (3) were nurses under pressure without delays actually performing better by giving less time per baby? (4) were unnecessary tasks done when not under pressure to fill time? (5) was there a cultural element to the lack of adequate breaks in nurses who can take breaks but do not, in solidarity with the harder-worked members of their teams? and (6) did the presence of the observer mean nurses were less inclined to take breaks, or bank their breaks for later in the shift? Furthermore, these ratios need contextualising against overall bed occupancy for the Network over a longer period of time. These argue the case for further study in this field, with careful re-assessment of what constitutes essential care in a busy neonatal unit and who should be undertaking these activities.
Simply based on our observations, this study implies that BAPM/DOH standards, far from being aspirational, are practically needed as the bare minimum for adequate service provision. In the absence of a burgeoning neonatal workforce, further work must focus as above on how to optimise neonatal nursing care provision in HDC and SC without compromising the patient or nurse.
Acknowledgments
The authors thank Babu Kumararatne and Sanjeev Deshpande for their helpful contribution to the discussion and all the nursing staff who contributed to this study.
Footnotes
-
Funding The independent observer was funded by the SSBC Newborn Network.
-
Competing interests None.
-
Ethics approval This study was approved by the SSBC Newborn Network contributing Hospitals Audit Departments.
-
Provenance and peer review Not commissioned; externally peer reviewed.