Article Text

Abstract
Objective We aimed to study the determinants of neonatal weight loss measured on the third day of life in term-infants.
Design The EDEN mother–child cohort is a prospective study that recruited 2002 pregnant women before 24 weeks of gestation in two French university hospitals. Neonates were weighed every day until discharge that occurred on average 4.5 days after birth. Altogether, 1557 healthy term neonates with data on weight at day 3 and feeding mode available were included. The outcome variable was weight loss at day 3 (D3WL), expressed as a percentage of birth weight lost in the first 3 days of life. Our main explanatory variables were maternal pre-pregnancy body mass index (BMI), gestational weight gain, gestational diabetes, birth weight, gestational age and feeding mode.
Results Factors associated with greater D3WL, whatever the feeding mode, were: higher birth weight, gestational diabetes and caesarean section; higher gestational age was associated with a reduced D3WL. The association between maternal pre-pregnancy BMI and D3WL differed by feeding mode (interaction p value=0.0002). In breastfed babies, mean D3WL ranged from 4.9% for neonates of underweight mothers to 5.8% for neonates of obese mothers (p trend=0.0005). In formula-fed babies, D3WL was highest for neonates of underweight mothers (4.1%) and lowest for those of obese mothers (2.6%) (p trend=0.01).
Conclusions The lower D3WL in formula-fed neonates, especially in neonates of obese mothers, suggests a relative overfeeding in the early days compared with breastfed neonates, which may potentially have consequences on later health. Overweight and obese mothers may need extra support to prevent early breastfeeding discontinuation.
Statistics from Altmetric.com
In most babies, the first postnatal days are characterised by an initial weight loss. This period constitutes a transition from the intra- to the extra-uterine life. For the first time, neonates must adapt their energy expenditure to more variable external conditions than those experienced in-utero, and learn to regulate their own energy intake. This period may be critical for the postnatal programming of appetite and energy metabolism, setting the lifetime regulation of weight control, as shown in animal studies.1 2
What is already known on this topic
▶ Breastfed babies lose more weight than formula-fed babies in the first days of life.
▶ Neonatal weight loss has been shown to increase with birth weight and female sex, and to decrease with gestational age.
▶ The effects of this initial weight loss on later growth and decision to supplement breast feeds are unclear.
What this study adds
▶ Maternal obesity exacerbates neonatal weight loss in breastfed infants.
▶ Obese mothers may require additional support in order to effectively establish breast feeding and prevent early discontinuation.
▶ Maternal obesity is associated with lower weight loss in formula-fed neonates.
Whether a larger weight loss is beneficial or detrimental for later health remains unclear as to our knowledge there are no data on the long-term consequences of this initial loss. Only one study found that a larger weight gain in the first week of life was associated with overweight in adulthood in formula-fed infants, independently of their birth weight.3 Therefore, a higher initial weight loss would rather be protective against later overweight. On the other hand, degree of weight loss is critical in the decision to supplement breastfed infants4 and introduction of supplements is a risk factor for breastfeeding discontinuation.5 As a consequence, these infants may not benefit from a feeding mode that has been shown on average to reduce the risk of childhood obesity by 22%,6 although this effect is still discussed.7 8 Therefore, a better understanding of the determinants of neonatal weight loss is needed.
MacDonald et al showed that neonatal weight loss varied with the feeding mode: median neonatal weight loss was 3.5% of the initial birth weight in exclusively formula-fed infants, versus 6.6% in exclusively breastfed babies.9 Factors significantly associated with greater neonatal weight loss included higher birth weight, female sex, epidural use and longer hospital stay. Lower neonatal weight loss was associated with greater gestational age and exclusive formula feeding.4 Dewey et al showed that excessive neonatal weight loss (>10% of birth weight) was more frequent among neonates of women with a body mass index (BMI) >27 kg/m2, but this relationship disappeared after adjustment.10 Another study found that babies of obese breastfeeding mothers lost more weight in the maternity ward compared with neonates of reference-weight breastfeeding mothers.11 Other maternal characteristics that have previously been associated with intrauterine growth and later obesity in the child, such as maternal gestational weight gain12 or gestational diabetes,13 have not been investigated in relation to neonatal weight loss.
Our objective was to study the determinants of neonatal weight loss measured on the third day of life in term-infants.
Methods
Subjects
The EDEN study is an ongoing birth-cohort study that aims to analyse the influence of pre- and postnatal determinants of child growth, development and health. Pregnant women were recruited in two French university hospitals before 24 weeks of gestation. Exclusion criteria were multiple pregnancies, known diabetes prior to pregnancy, illiteracy, moving outside the region planned in the next 3 years. Of the 2002 women recruited, data were available on the child's birth characteristics for 1893 newborns (figure 1). The EDEN study received approval from the ethics committee (CCPPRB).
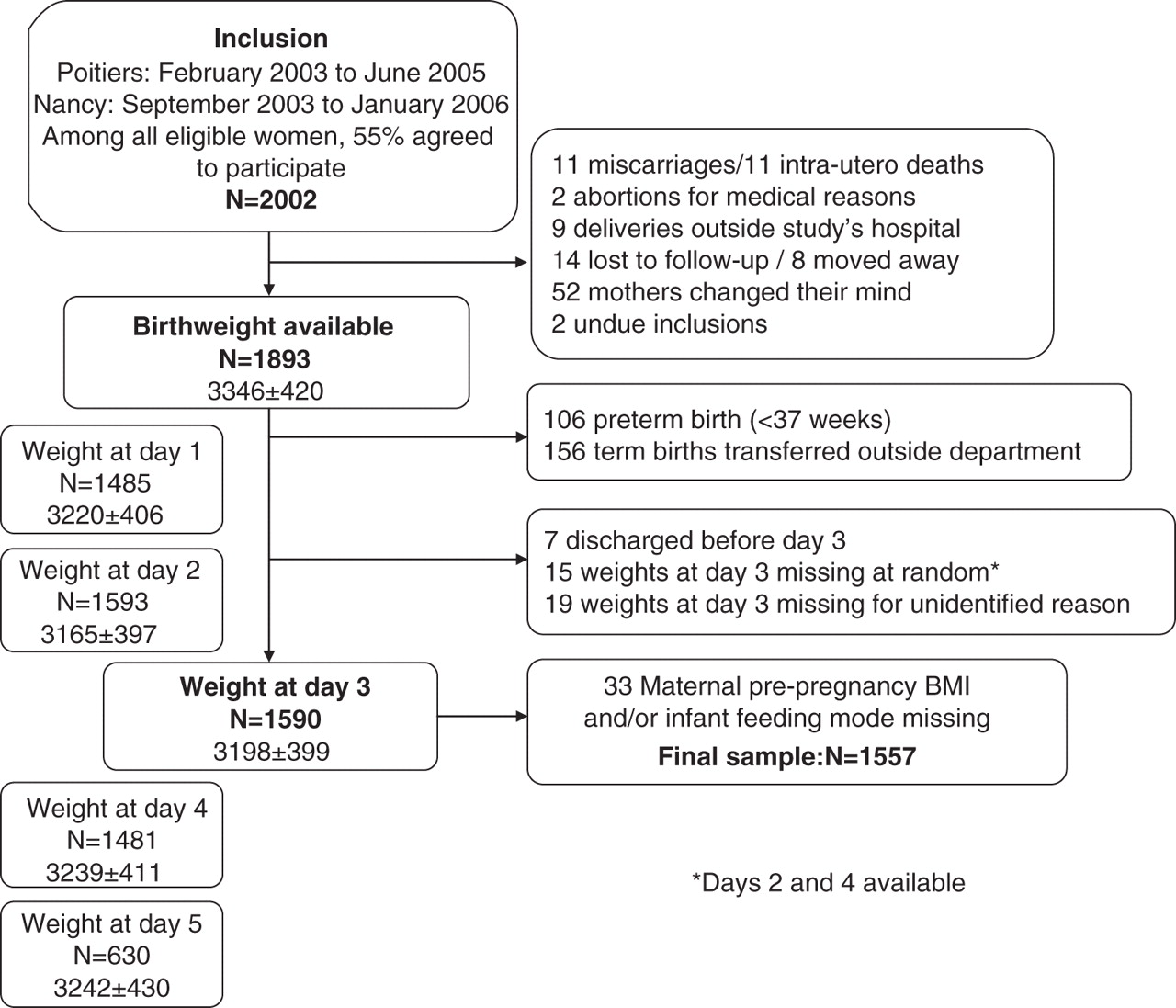
Study flow chart (mean±SD).
Parental, obstetric and neonate's characteristics
Between 24 and 28 weeks of gestation, mothers and fathers completed a self-administered questionnaire and had a clinical examination performed by research midwives. Maternal education, maternal tobacco use before pregnancy and in the first and second trimester (third trimester use was collected at birth) and self-reported maternal weight before pregnancy were obtained in the questionnaire. During the clinical examinations, parental weights were measured using electronic Terraillon SL-351 scales (Hanson, Hemel Hempstead, UK)to the nearest 0.1 kg. Parental heights were measured with a wall Seca-206 stadiometer (Hamburg, Germany) to the nearest 0.2 cm. Mothers were also weighed on average 2 days after birth by the same research midwives. Maternal gestational weight gain was calculated as measured weight after delivery minus self-reported weight before pregnancy. Parental BMIs were computed as weight (kg) divided by square of measured height (m) and classified according to the usual categories.14
From obstetric and paediatric records, we extracted data on parity, gestational diabetes, type of labour, anaesthesia, delivery mode, offspring's sex and gestational age. Birth weight was measured with electronic Seca scales (Hamburg, Germany: Seca 737 in Nancy and Seca 335 in Poitiers with a 10 g precision). Afterwards, neonates were weighed every day until discharge that occurred on average 4.5 days after birth, which is current practice in France. Our data, in accordance with MacDonald et al, suggest that the nadir occurred on average between the second and third day. Our outcome variable was the weight loss measured at day 3 and was expressed as a percentage of birth weight lost in the first 3 days: D3WL=(birth weight−weight at day 3)×100/birth weight.
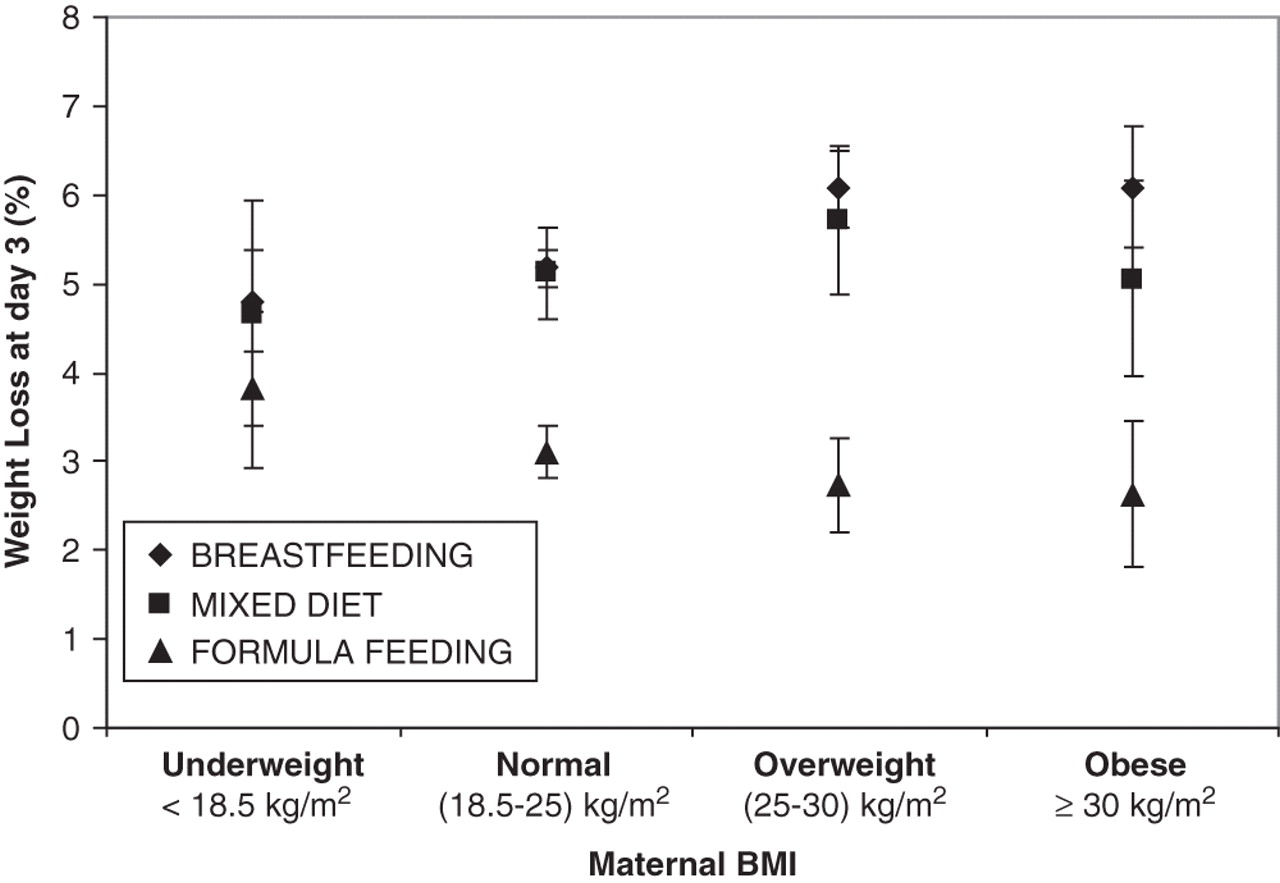
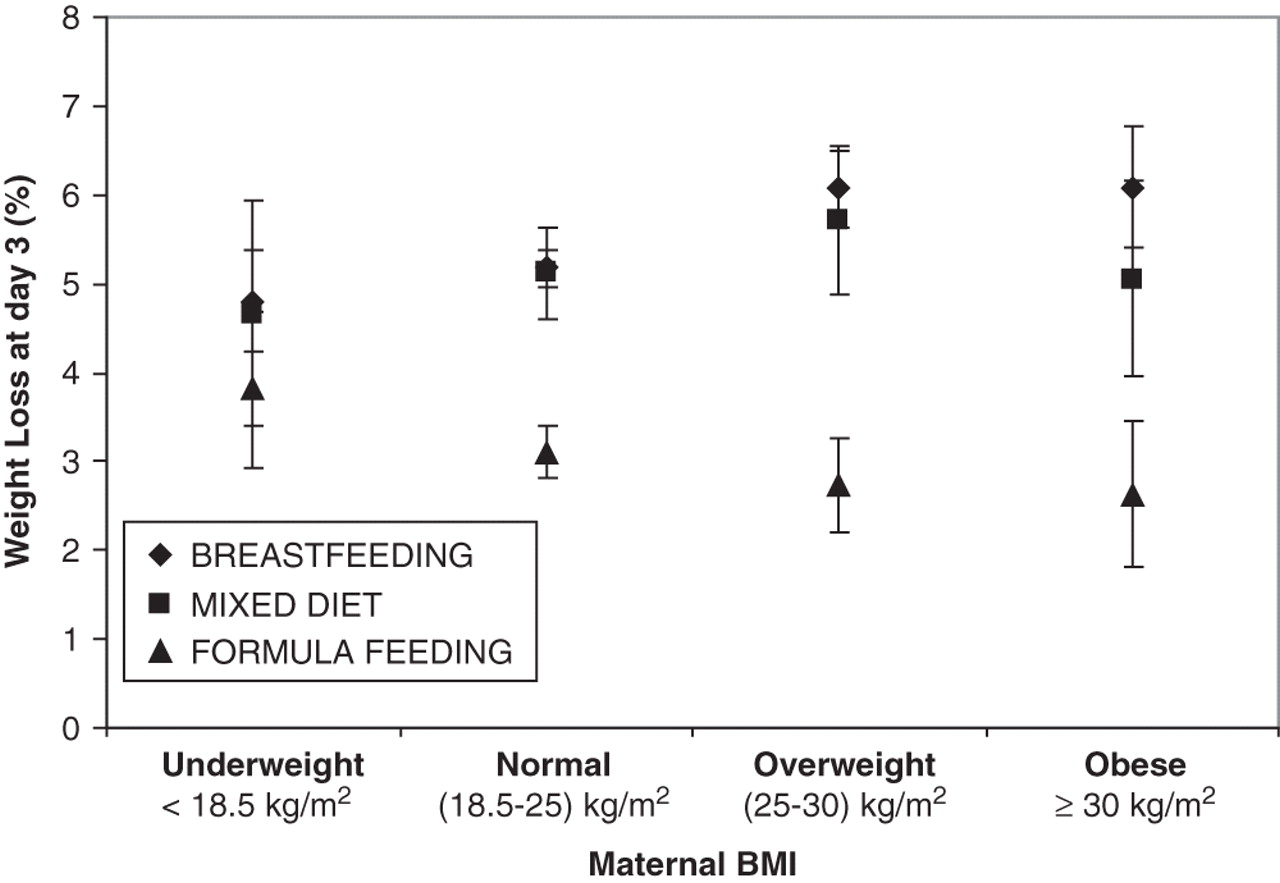
The infant's feeding method was initially used as a 3-class variable: exclusive breast feeding from birth to discharge, exclusive formula-feeding and mixed-feeding (when supplementary feedings that had been given). The similarity of the patterns of D3WL seen in breastfed and mixed-fed neonates (figure 2) led us to combine them in a single ‘breast feeding’ class as opposed to ‘exclusive formula’.
{kind=link}
{kind=link}
Weight loss % (mean and 95% CI) at day 3 according to maternal BMI and feeding method: model adjusted for birth weight and gestational age.
Statistical analysis
Student t tests and analyses of variance were used to test for crude associations between D3WL and potential determinants. Subsequently, we performed multivariate analyses, using general linear models, with D3WL as the dependent variable. The explanatory variables in our final model included all the variables that were significantly associated (p≤0.05) with D3WL in crude analyses (table 1), but start of labour, due to its high collinearity with delivery mode. Recruitment centre and the infant's sex were also included in the model. We tested the potential interactions between all the explanatory variables and feeding mode, using a p≤0.15 threshold for significance (table 2: ‘tests for interactions’).
Description of the 1557 included trios and crude associations between weight loss at day 3 and parental, obstetric and infant characteristics
Linear regression coefficients from a multivariate regression analysis showing the association between weight loss at day 3 as dependent variable, and maternal, obstetric and neonate's characteristics with a stratification by feeding mode
When the interaction was not significant (ie, the effect of the explanatory variable on D3WL was the same whatever the feeding mode), we refer to the results shown in table 2: model 1.
When the interaction was significant (ie, the effect of the explanatory variable on D3WL differed according to the feeding mode), we refer to the regression models stratified by feeding mode (table 2: models 2 and 3). Analyses were carried out with SAS (version 9.1; SAS Institute, Cary, North Carolina, USA).
Results
As described in figure 1, our final sample included 1557 neonates and their parents. The term babies excluded for missing data did not differ significantly from their peers regarding all the characteristics listed in table 1. In the 1557 included mother–child pairs, infant weight change between birth and day 3 was normally distributed and ranged from a large loss (−14.2% of birth weight) to a weight gain (+8.2%). A larger D3WL was observed among exclusively breastfed babies (5.3%) and mixed-fed babies (5.2%) as compared to formula-fed newborns (3.1%). Altogether, 61 neonates (4%) lost more than 10% of their birth weight: 85.2% of them were exclusively breastfed and none were exclusively formula-fed, 38% had an overweight or obese mother compared to 26% in the whole sample.
In unadjusted analyses, infants of older women, of mothers diagnosed with gestational diabetes, had a significantly larger D3WL (table 1). Start of labour and delivery mode was significantly associated with D3WL, but there were no associations of D3WL with epidural and/or spinal anaesthesia, paternal BMI, or with the infant's sex. D3WL decreased with gestational age while it increased with birth weight. D3WL was higher in babies of non-smokers and in babies of women with a higher education, due to higher breastfeeding rates in these groups: differences were not significant anymore in multivariate analyses.
Figure 2 illustrates the interaction between maternal pre-pregnancy BMI and feeding mode on D3WL in a multivariate model adjusted only for birth weight and gestational age (p for interaction=0.0006). D3WL was larger in breastfed than in formula-fed babies, for any maternal BMI. D3WL increased with increasing maternal BMI in babies exclusively breast fed (p for trend <0.0001). It decreased with increasing maternal BMI in formula-fed babies (p for trend=0.03). In a multivariate model adjusted for all the selected explanatory variables and maternal pre-pregnancy BMI used as a four-class variable (model not shown), breastfed babies born to underweight mothers lost 4.9% of their birth weight, while they lost 5.8% if born to obese mothers (p for trend across BMI categories=0.0005). Formula-fed babies born to underweight mothers lost 4.1% of their birth weight, while they lost 2.6% if born to obese mothers (p for trend=0.01). In contrast, there was no interaction between paternal BMI and feeding mode on D3WL (p for interaction=0.36) and paternal BMI was not significantly associated with D3WL in a multivariate analysis.
Interactions were also found between the feeding mode and centre, parity, gestational weight gain and the neonate's sex (table 2: interaction p value). Table 2 (models 2 and 3) shows the stratified results. D3WL was significantly different in the two centres in the breast fed but not in the formula-fed group. D3WL was significantly lower among multipara than primipara in the breastfed category (−0.81%, p<0.0001). The positive association between gestational weight gain and D3WL was only significant in the breastfed group (+0.45% of D3WL for a 10 kg increase, p=0.01). When formula-fed, male neonates seemed to lose significantly less weight than females (−0.57%, p=0.02). The difference was not significant in breastfed babies.
Neonates of mothers diagnosed with gestational diabetes lost more weight than other babies: the adjusted mean difference in D3WL was 0.64%. D3WL was also higher after an emergency caesarean section, as compared to vaginal delivery (p=0.004), and babies born after a planned caesarean section lost even more weight. D3WL decreased with each additional week of gestation and increased with birth weight. There was a 2% difference in D3WL between infants born at 37 weeks and infants born at 42 weeks and a 1% difference in D3WL for a 1 kg higher birth weight. A 10-year increase in maternal age was associated with 0.46% higher D3WL (table 2).
Discussion
To our knowledge, the search for contributors to weight loss has never been carried out after stratification by feeding mode, hence missing the opportunity to discriminate between factors that modulate D3WL via their role in breast feeding and others that have an effect on their own. Our prospective cohort allowed us to study a number of maternal characteristics that have not been studied before in relation to D3WL.
A comparison with a representative survey carried out on about 15 000 pregnant French women in 200315 indicated that women in the EDEN study were more educated and more often employed, showed healthier life-styles and were more likely to exclusively breast feed when in the maternity hospital, than the general French population. In addition, our results apply only to the healthier term-newborns as all premature and transferred babies have been excluded from the analysis.
We did not intend to use the maximum weight loss for all the neonates as our outcome. It has been shown to be between the second and third day which was confirmed in our data.9 Even with daily weighings as we did, we might have missed the real nadir. However, we repeated all the analyses with weight at day 2 as dependent variable and also with the lowest weight recorded for each neonate whatever the day of measurement. The results were not materially changed which suggests that the factors we identified are associated with both weight loss at day 2 and 3.
D3WL may be partly explained by a loss of fluids, mainly through urine, as well as a loss of solids, such as meconium. Part of the D3WL may also be attributed to the mobilisation of the neonate energy stores to face new needs of the extra-uterine environment, such as thermoregulation. The relative contribution of the two mechanisms is still uncertain. In adequate-for-gestational-age term neonates, D3WL was associated with a decrease in total body water with a probable role of body energy stores.16
In our study, a number of prenatal factors appeared as predictors of D3WL, independently of the neonates's feeding mode. The abandonment of a very rich and hyperglycaemic environment may result in an increased postnatal weight loss, as shown by the positive associations between D3WL and gestational diabetes or birth weight; while the negative association with gestational age may reflect a difference in the maturation of the feeding capabilities or behaviour. As shown in pre-term babies,17 the more mature they are, the more efficiently they suckle and swallow.
Formula-fed neonates lost less weight in the first 3 days than breastfed neonates whatever their mother's BMI. Within the formula-fed group, neonates born to overweight or obese mothers, who may have a greater risk of later overweight, are those who lost the least weight. This is of particular interest in the context of the current obesity epidemic. Some have suggested that formula-fed neonates may be at risk of ‘overfeeding’ in the early days.4 During this period, breastfed babies receive a dramatically smaller quantity of milk than formula-fed babies and go through a period of relatively reduced intake until lactation is fully established, around the third day after birth.18 By contrast, the formula is readily available from birth onwards and newborns offered formula ad libitum, seem to consume much larger amounts than breastfed babies.19 Differences in D3WL between breastfed and formula-fed may also arise from the composition of the milk. As an example, it has been suggested that the maternal leptin ingested by the breastfed baby may add to the baby's own leptin.20
In the breastfed group, neonates born to overweight and obese mothers lost significantly more weight than those born to mothers with a normal BMI. This might be disadvantageous if the higher weight loss results in early breastfeeding discontinuation, especially as neonates of overweight and obese mothers may particularly benefit from the potential protective effect of breast feeding.21 This is consistent with the literature that shows that these women have more difficulties in initiating and sustaining breast feeding adequately.22 23 They experience greater difficulties in positioning the baby, have a delayed onset of lactation24 or smaller amounts of milk due to abnormal prolactine response to suckling.25 Extra support may be needed for overweight and obese mothers who intend to breast feed. Higher gestational weight gain has also been negatively associated with lactational performance26 and is associated with greater D3WL in our data.
Our results also point out that a number of factors may increase D3WL in breastfed babies only, by undermining breastfeeding success. The association between parity and D3WL may be explained by greater difficulties to initiate breast feeding in primipara.23 The significant difference in D3WL observed between the two study centres in breastfed babies may reflect differences in the characteristics of the population, but also reveal differences in the support offered to breastfeeding mothers.27 28 Indeed, hospital policies and clinical practices contribute greatly to breastfeeding initiation and duration.5 Additional qualitative studies are warranted to understand how practices impact neonatal weight loss.
Conclusion
This study confirms previous reports that formula-fed neonates lose less weight in the neonatal period than their breastfed counterparts and may suggest a relative overfeeding of formula-fed babies in the first days of life. Maternal obesity exacerbates neonatal weight loss in breastfed neonates suggesting that obese mothers may require additional support in order to effectively establish breast feeding. On the contrary, maternal obesity is associated with lower weight loss in formula-fed neonates. This reduced neonatal weight loss in the formula-fed neonates, who are at higher risk of later overweight because of maternal obesity, might have adverse long-term consequences.
Acknowledgments
We are indebted to the participating families, to the midwife research assistants (L Douhaud, S Bedel, B Lortholary, S Gabriel, M Rogeon, M Malinbaum) for data collection and to P Lavoine, J Sahuquillo and G Debotte for checking, coding and data entry.
References
Footnotes
-
EDEN mother–child cohort study group MA Charles, M de Agostini, A Forhan, B Heude, P Ducimetière (INSERM, U780), M Kaminski, MJ Saurel-Cubizolles, P Dargent, X Fritel, B Larroque, N Lelong, L Marchand, C Nabet (INSERM U953), I Annesi-Maesano (INSERM U707), R Slama (INSERM U823), V Goua, G Magnin, R Hankard, (Poitiers University Hospital), O Thiebaugeorges, M Schweitzer, B Foliguet (Nancy University Hospital), N Job-Spira (ANRS).
-
Funding We acknowledge all funding sources for the EDEN study: Fondation pour la Recherche Médicale (FRM), French Ministry of Research: IFR program, INSERM Human Nutrition National Research Program, and Diabetes National Research Program (through a collaboration with the French Association for Diabetes Research (ARD)), French Ministry of Health, French Agency for Environment Security (AFFSET), French National Institute for Population Health Surveillance (INVS), Paris–Sud University, French National Institute for Health Education (INPES), Nestlé, Mutuelle Générale de l'Education Nationale (MGEN), French speaking association for the study of diabetes and metabolism (ALFEDIAM), National Agency for Research (ANR non-thematic programme), National Institute for Research in Public health (IRESP: TGIR cohorte santé 2008 program). Statistical analyses were carried out in complete independence of funders.
-
Competing interests NR received a grant from Nestlé to subsidize, in part, her PhD.
-
Patient consent Written consent was obtained from the mother for herself at the beginning of the study and from both parents for the newborn child after delivery.
-
Ethics approval The EDEN study received approval from the ethics committee (CCPPRB) of Kremlin Bicêtre on 12 December 2002. Files have been declared to the ‘National Committee for Processed Data and Freedom’ (CNIL).
-
Provenance and peer review Not commissioned; externally peer reviewed.