Article Text

Abstract
Aims: To ascertain the prevalence of premedication before intubation and the choice of drugs used in UK neonatal units in 2007 and assess changes in practice since 1998.
Methods: A structured telephone survey of 221 eligible units was performed. 214 of the units surveyed completed the telephone questionnaire. The units were subdivided into those that routinely intubated and ventilated neonates (routine group) and those that intubated neonates prior to transfer to a regional unit (transfer group). A similar study was performed by one of the authors in 1998. The same telephone methodology was used in both studies.
Results: Premedication for newborn intubations was provided by 93% (198/214) of all UK units and 76% (162/214) had a written policy or guideline concerning premedication prior to elective intubation. Of those 198 units which premedicate, morphine was the most widely used sedative for newborn intubations with 80% (158/198) using either morphine alone or in combination with other drugs. The most widely used combination was morphine and suxamethonium±atropine, which was used by 21% (41/198) of all units. 78% (154/198) of all units administered a paralytic agent.
Conclusions: There has been substantial growth over the last decade in the number of UK neonatal units that provide some premedication for non-emergent newborn intubation, increasing from 37% in 1998 to 93% in 2007. This includes a concomitant increase in the use of paralytic drugs from 22% to 78%. However, the variety of drugs used merits further research.
Statistics from Altmetric.com
Endotracheal intubation in newborns and infants is a process often associated with adverse physiological events such as elevated intracranial pressure,1 hypoxaemia and cardiovascular instability.2 3 Randomised controlled trials (RCTs), case–control studies and cohort studies have established that premedication for non-emergent neonatal intubations results in fewer attempts, shorter procedural times, and greater physiological stability.4 Nevertheless, there is debate about the most appropriate premedication sedatives and paralytic agents for newborns undergoing non-emergent intubation.5
What this study adds
In 2007 the majority of UK neonatal units (93%) provided for some premedication prior to non-emergent endotracheal intubation in newborns.
Most UK neonatal units (78%) administered a paralytic agent with a sedative as part of this premedication.
The most widely used premedication combination (used by 21% of all UK neonatal units) was morphine and suxamethonium±atropine.
Previous studies have shown low rates of premedication for endotracheal intubation especially in small and preterm newborns.6 7 There are international differences regarding the extent of usage and the variety of drugs used as neonatal premedication.8 In 1998 Whyte et al7 performed a telephone survey of all UK neonatal intensive care units (NICUs) in order to ascertain the extent and variety of premedication used for newborn intubations in the UK. This survey had a response rate of 99%. The results indicated that at that time only 37% of units administered any sedation prior to intubation and only 14% had a written policy concerning this. Of the 88 units providing some type of premedication, the most widely used sedative was morphine (66%). Only 19 units administered a paralytic premedication (22% of the 88 sedating units). Suxamethonium was the most widely used paralytic agent in 10 of 19 units (53%), while only half of these combined it with atropine.
The aim was to assess current practice in the UK and changes over a 10-year period.
Methods
A total of 224 neonatal units in the UK were identified from the national directory obtained from CMA Medical Data Ltd (Cambridge Research Laboratories). All of these units were contacted by telephone over a 4-week period during November 2007. In each case contact was made with the neonatal sister or nurse in charge of the unit at the time. This maintained a consistent approach and ensured that reliable data pertaining to intubation guidelines and practices were obtained from the interviewee. On each occasion the investigator (PM or JK) explained the purpose of the survey. The investigator then obtained verbal permission to inquire about specific unit practices and following this a questionnaire was completed over the telephone. The questionnaire was the same as that used in the previous study by Whyte et al7 in 1998 in order to allow direct comparison.
Three units were excluded from the survey following telephone contact as they no longer functioned as neonatal units although still listed in the directory. A further seven units declined to participate in the telephone survey, but in each case the neonatal sister/nurse expressed a wish to participate in a written survey. The researchers therefore made written contact with all seven units and requested them to complete the same telephone survey but in a written form. For the purpose of our study we have excluded these seven units, confining the remit of our survey to those units which completed the telephone survey. A total of 214 units were therefore surveyed successfully by telephone. This represents a successful follow-up of 97% (n = 221).
Units were subdivided into those which routinely intubated and ventilated neonates (routine group) and those which intubated and ventilated solely for stabilisation prior to transfer of the newborn to another local tertiary level neonatal unit (transfer group). A further subgroup analysis was performed using the national neonatal cot locator service to identify those units providing level 3 neonatal intensive care (level 3 group) as defined by British Association of Perinatal Medicine (BAPM). In certain cases consultant neonatologists were contacted in order to ascertain the status of specific units. The results of this study have been analysed for the whole population of neonatal units and for the three subgroups.
Results
A total of 214 units completed the telephone survey. There were 166 units within the routine group and 48 in the transfer group. A total of 61 units were defined as level 3 NICUs.
Sedation practices and guidelines
Table 1 lists the questions asked of each unit by telephone and summarises the details regarding unit sedation practices and guidelines. Premedication for newborn intubations was provided by 93% (198/214) of all UK units. Only 7% (16/214) of units provided no premedication. Of the 16 units providing no sedation or premedication, 10 were of the transfer type and six were units which regularly intubated newborns. A total of 76% (162/214) of all units had a written policy or guideline concerning premedication prior to elective intubation. A further 17% (36/214) of units regularly provided some premedication before elective intubation although they had no set guidelines or policies regarding this practice. The majority of routine units (80%, 132/166) had a policy or guideline concerning premedication for elective intubation. Overall, 17% (28/166) of the routine units provided some premedication while not possessing a guideline or policy. Within the level 3 units, 82% (50/61) had a premedication policy, while 13% (8/61) administered premedication despite having no existing policy. Only three level 3 units provided no premedication for newborn intubations. Up to 44% (95/214) of all units stated that they used premedication for emergency newborn intubations, with 46% (77/166) of routine and 38% (18/48) of transfer units following this practice.
Numbers (%) of units with policies or regular practices for elective and emergency intubation/reintubation
Sedative premedication drugs used
Table 2 summarises the various sedative drugs used for premedication prior to newborn intubation.
Sedatives used by UK neonatal units before intubation/reintubation
Paralytic premedication drugs used
The majority of units administered a paralytic agent in addition to a sedative drug, with 78% (154/198) of all premedicating units, 74% (118/160) of routine units and 95% (36/38) of transfer units doing so. Table 3 summarises the paralytic agents and the common premedication drug combinations administered by units routinely intubating newborns (n = 118). The most frequently administered paralytic agent was suxamethonium, being used by 77% (91/118) of routine units. Atracurium was used by 16% (19/118) followed by pancuronium, used by 4% (5/118) of routine units. Three routine units used vecuronium combined with morphine.
Use of muscle relaxants by the 118 UK neonatal units which routinely intubate babies and administer paralytic premedication
A comparison of premedication drugs used in 1998 versus 2007
Figures 1 and 2 illustrate some of the main differences in the use of sedatives (fig 1) and paralytic drugs (fig 2) in all neonatal units between 1998 and 2007. In 1998 morphine was widely used as a single sedative agent in 42% (37/88) of all units providing sedation, whereas in 2007 morphine monotherapy had decreased to 14% of units (27/198). In 1998 only 24% (21/88) of all premedicating units administered morphine in combination with a paralytic drug, another sedative (diazepam or midazolam) or atropine, which had increased in 2007 to 66% (131/198). There has been a relative increase in the proportion of all units using fentanyl combined with a paralytic drug, with or without atropine and/or another sedative drug, being 4.5% (4/88) in 1998 and 19% (38/198) in 2007. Use of diamorphine has decreased substantially from 14% of all units providing sedation (12/88) in 1998 to only two units in 2007.

A comparison of the main differences in sedatives used for premedication prior to intubation in all UK neonatal units in 1998 (n = 88) compared to 2007 (n = 198). #Other refers to paralytic drugs, atropine and/or additional sedatives.

{kind=link}
{kind=link}
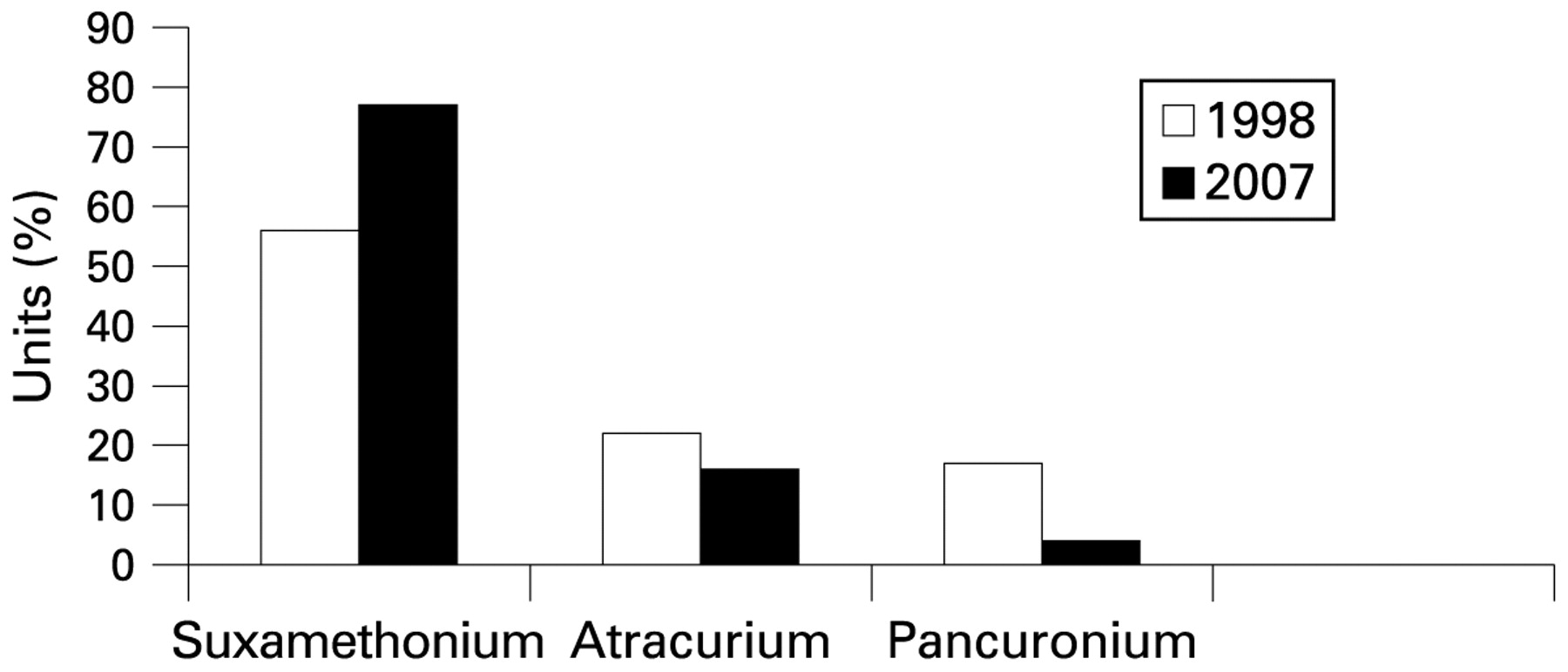
A comparison of the main differences in paralytic drugs used for premedication in UK neonatal units which routinely intubate newborns and which utilised paralytic drugs in 1998 (n = 18) versus 2007 (n = 118).
There has been a relative increase in the use of midazolam combined with other drugs between 1998 and 2007. In 1998, 6.5% (6/88) of all units providing sedation administered midazolam with or without morphine. Four of these units administered midazolam alone while two combined it with morphine. In 2007 the number of units which sedate and administer midazolam with or without morphine has increased to 11% (22/198). Five of these units use midazolam with morphine while the remaining 17 units use morphine/midazolam with a paralytic drug±atropine.
In 1998 only 19 units (22%, 19/88) of those providing premedication, administered paralytic agents. One of these was a transfer unit, while the remaining 18 units routinely intubated newborns. This number had increased to 78% (154/198) of all units which premedicated in 2007. In both 1998 and 2007, suxamethonium remained the most frequently used paralytic drug in those neonatal units routinely intubating newborns. In 1998, of the 18 routine units using paralytic drugs, 56% (10/18) used suxamethonium. In 2007 this proportion had increased to 77% (91/118) of routine units using paralytic drugs. Atracurium was used by 22% (4/18) of routine units administering paralytic drugs in 1998 versus 16% (19/118) of such units in 2007. Pancuronium was used by 17% (3/18) of routine units administering paralytic drugs in 1998 versus 4% (5/118) of such units in 2007.
Discussion
Our study has shown a significant change in the practice of providing premedication prior to elective newborn intubation between 1998 and 2007 in the UK. At the time of the original study only 37% of UK neonatal units provided some sedation prior to neonatal intubation and only 14% of units had premedication guidelines for newborn intubation.7 Neuromuscular paralytic agents were only administered by 22% (19/88) of all premedicating units. Morphine monotherapy was the main form of sedation with 42% (37/88) of all units using it. Since 1998 there has been a more than twofold increase in the number of units using premedication for non-emergent intubation, such that 93% of all UK units now follow this practice. Similarly, most units (76%) now have a guideline/protocol concerning premedication for neonatal intubation and while some units lack a formal guideline (17%), most still administer some type of premedication. As in 1998, morphine remains the most widely used sedative for newborn intubation with 80% (158/198) of all units using either morphine alone or in combination with another sedative, a paralytic and/or atropine. This must be due to familiarity as while an excellent analgesic, it is a poor sedative, especially in the timescale required for intubation.9 Since 1998 there has been a fourfold increase in the number of units using fentanyl combined with a paralytic drug, with or without atropine and/or another sedative drug. This substantial increase is perhaps attributable to recent evidence concerning fentanyl in combination with mivacurium±atropine.10 11
The single most widely administered combination of premedication drugs used for newborn intubations was morphine and suxamethonium±atropine. This combination was used by 21% (41/198) of all premedicating units. The ± status of atropine is used to denote the fact that while some units claimed that they always administered atropine in combination with sedatives and/or paralytic drugs, other units only occasionally administered atropine if clinically indicated.
There is a significant difference between the two decades in the use of paralytic drugs for newborn premedication. In 2007 the majority of units administered a paralytic agent in addition to a sedative drug, with 78% of all premedicating units, 74% of routine units and 95% of transfer units doing so. This compares to a minority (22%) of all premedicating units in 1998 which administered paralytic drugs. For over a decade suxamethonium has remained the most commonly used paralytic agent amongst units using a neuromuscular paralytic agent as a premedication drug. Nevertheless, some units in 2007 use more than one paralytic drug interchangeably. For example, of the 11 routine units combining atracurium with morphine, five also used either suxamethonium or pancuronium. The high rate of paralytic drug usage amongst the transfer group of units in 2007 (36 of 38 units surveyed) is significantly greater than in 1998. This study did not examine the specific indications for which units used particular paralytic agents.
While suxamethonium is a well established paralytic agent for emergent intubation, concerns were raised regarding its role in young children by the US Food and Drug Administration (FDA) in a drug safety alert in 1997.12 These concerns highlighted the risk of sudden cardiac arrest in children with previously undiagnosed myopathies who received suxamethonium. It is interesting that in spite of these concerns suxamethonium remains widely used in the UK. An alternative to the use of paralytic drugs for newborn intubations while still achieving effective sedation is the use of propofol. A recent study concluded that in premature neonates, propofol achieved successful intubation twice as quickly as a combination regimen of morphine, atropine and suxamethonium with less hypoxaemia whilst preserving spontaneous respiration.13
Evidence that premedication facilitates intubation, shortens the duration of laryngoscopy attempts and reduces the incidence of hypoxia during intubation attempts10 11 13 14 15 may have changed the practices of UK neonatologists since 1998. In the UK, the initial study by Whyte prompted much internet discussion (JW personal communication, 2000) and this may have encouraged an examination of the evidence. Recent research has provided some evidence for mivacurium (200 μg/kg) and fentanyl (2–5 μg/kg)10 with or without atropine (10–20 μg/kg),11 and propofol (2.5 mg/kg)13 as acceptable regimens, but despite this the most commonly used combination in the UK remains morphine, atropine and suxamethonium (MASux) for which there is little evidence.
This study used the same questionnaire as in 1998 permitting direct comparison. In addition, only neonatal nurses or unit managers were interviewed over the telephone in both studies, thus providing consistency. If neonatologists had been contacted their answers might have reflected their own professional practice rather than a neonatal unit’s approach.
It is interesting that 44% of units used premedication for emergency newborn intubation. Although some emergency intubations occurring in a neonatal unit might indeed be facilitated by the use of premedication, its use for emergency intubation within the context of the delivery room is unproven. Therefore, it is possible that there may have been variation in the way interviewees interpreted the word “emergency”. Furthermore, the interviewers did not specify the location of an emergency newborn intubation (eg, delivery suite vs neonatal unit). Therefore, this figure should be viewed cautiously.
Similar surveys of the practices of neonatologists have been performed since the study by Whyte et al7 which have shown that the practice of premedication prior to newborn intubation varies remarkably between different countries. In a recent study by Sarkar et al16 in the USA, directors of neonatology fellowship programs were contacted by e-mail and surveyed regarding the practice of premedication. Only 43.6% of the 78 fellowship programs contacted acknowledged that they provided for some premedication prior to elective newborn intubation. Only 25% of the respondents used a paralytic agent with sedation for premedication. In 2001 a prospective questionnaire survey was performed in 75 of 98 licensed neonatal and paediatric intensive care units in France concerning premedication for intubation.6 This study found that premedication for non-emergent intubations was only used in 37.1% of newborns with midazolam being the main drug used. Furthermore, premedication was more frequently used in term than preterm newborns.
It would appear that in comparison to 1998, most neonatologists in the UK in 2007 regard premedication as desirable and normal practice. However, the range and types of medications currently used demonstrate that the evidence is insufficient to define which single premedication drug or combination of premedication drugs has maximal speed of onset and the best side effect profile for intubation in the neonatal period.
Acknowledgments
We gratefully acknowledge Drs Simon Whyte and Ginny Birrell for their support. Permission was obtained from Dr Whyte to use the questionnaire.
REFERENCES
Footnotes
Competing interests None.
Linked Articles
- Fantoms