Article Text

Abstract
Objective: To document perinatal events, brain imaging, neurophysiology and clinical outcome in term infants with early postnatal collapse (PNC).
Design: Tertiary referral centre, retrospective case review (1993–2006).
Patients: Infants born at ⩾36 weeks’ gestation with early (<72 h) PNC. Peri-partum and post-collapse data were collated with clinical, electrophysiological, neuroimaging and autopsy data and neurodevelopmental outcome.
Results: Twelve infants were studied; median gestation 39 weeks (36–41), birth weight 3150 g (1930–4010). Ten were born vaginally (including occipitoposterior (1), breech (2), water birth (2), ventouse/forceps (3)), and two by emergency caesarean section. Median Apgar scores were 9 (3–9) and 10 (8–10) at 1 and 5 min; median cord pH was 7.29 (7.18–7.34). All were thought to be well after birth. The median age at PNC was 75 min (10 min to 55 h). All infants required extensive resuscitation. The median pH after PNC was 6.75 (6.39–7.05). Seven infants became severely encephalopathic, with severely abnormal EEG/aEEG recorded within 12 h. MRI showed acute severe hypoxic–ischaemic injury. All died. One infant showed rapid recovery, had mild encephalopathy, and good outcome. Four infants had severe respiratory illness, normal background EEG, and MRI showing slight white matter change (n = 3) or a small infarction (n = 1). All had a good 2-year outcome.
Conclusions: In this term cohort, early PNC was generally followed by severe encephalopathy, acute central grey matter injury and poor outcome, or severe respiratory illness, slight white matter change and good outcome. Early EEG and MRI predicted outcome accurately. However, no antepartum, intrapartum or other aetiological factors were identified. Further investigation is needed in larger PNC cohorts.
Statistics from Altmetric.com
A sudden early postnatal collapse (PNC) in a previously apparently healthy term infant is rare, but has been described and reviewed.1–5 The incidence of such events appears to be 0.03–0.5/1000 live births with a high mortality.4 5 Current literature provides only a limited description of the clinical events around the time of collapse and minimal data on electrophysiological or neuroimaging findings.
What is already known on this topic
A small subset of term infants die from postnatal collapse similar to sudden infant death syndrome and often when prone and unsupervised with first-time mothers.
There is little literature detailing the neuroimaging and electrophysiology findings in these infants.
What this study adds
Apparently well term neonates presenting with early postnatal collapse appear to divide into two apparently distinct clinical groups.
Those without respiratory disease have severe encephalopathy, brain MRI findings that show severe basal ganglia and thalami injury, and a poor outcome, whereas those with a severe respiratory course have mild to moderate white matter abnormality and a good outcome.
Further study into postnatal collapse is warranted.
The advent of bedside electrophysiological monitoring and the increased availability of MRI allow more detailed study of the aetiology of PNC. After perinatal brain injury, electrophysiological data6–9 enable global prognostication, and MRI provides detailed information on the pattern of lesions10 11 and is an excellent predictor of outcome after hypoxic–ischaemic insults and stroke.12–17 Specific patterns of abnormality are also seen in hypoglycaemia18 19 and metabolic20 and infective disorders.21
The aim of this study was to document the clinical, electrophysiological (EEG or amplitude integrated aEEG), cranial ultrasound (US), MRI and autopsy findings in a cohort of such infants to try to understand the aetiology of collapse and document outcome.
PATIENTS AND METHODS
Infants ⩾36 weeks’ gestation, inborn or referred to the Hammersmith and Queen Charlotte’s Hospitals (1993–2006) for specialist opinion, who appeared healthy at birth but suffered acute PNC (<72 h after delivery) requiring extensive resuscitation, were included in the study.
Data were extracted from case notes, referral letters and information obtained from parents at the time of admission. Perinatal data included onset and progress of labour, fetal distress, analgesia, acute antepartum or intrapartum events, delivery, gestational age, sex, birth weight, head circumference, Apgar score and cord pH. Postnatal data included presentation, time of collapse, relation to feeding, resuscitation required, post-collapse pH and subsequent clinical course. Cerebral function monitor (aEEG), EEG, US and MRI findings, along with results of infective and metabolic investigations and autopsy, were assessed.
Imaging
Cranial US scans
From 1993 to 2002, US scans were obtained using an Advanced Technology Laboratory (ATL) Ultramark-4 mechanical sector scanner with 5.0 and 7.5 MHz probes (Philips Medical Systems, Best, The Netherlands). Subsequently a Siemens Antares scanner with a multifrequency transducer (Siemens Medical Solutions, Bracknell, UK) was used. Scans were printed on high-quality paper (ATL) or stored on disc (Antares). All images were assessed by an experienced ultrasonographer (FMC).
MRI scans
Most infants had a brain MRI scan in the neonatal period. Infants were examined during natural sleep after a feed or were sedated with oral chloral hydrate (30–50 mg/kg). They wore ear protection and were monitored with pulse oximetry and electrocardiography. A neonatologist experienced in MRI was present throughout the scan.
Imaging parameters
MRI was performed using a 1.0 T dedicated neonatal magnet (Oxford Magnet Technology/Marconi Medical Systems, Cleveland, Ohio, USA), a 1.5 T Philips Eclipse Scanner or a 3.0 T Philips scanner. T1-weighted and T2-weighted sequences were acquired in the transverse plane, and T1-weighted sequences in the sagittal plane. Diffusion-weighted imaging (DWI) was not performed for all infants; when available and of adequate quality, apparent diffusion coefficient maps were analysed visually and results recorded. All images were assessed by experienced neuroradiologists (CC and MAR).
Image analysis
All images were assessed for
normal anatomy and structural development;
acute injury, ie, abnormal signal intensity (SI) within basal ganglia and thalami (BGT), posterior limb of the internal capsule (PLIC), brainstem or cortex;
evidence of more prolonged/sub-acute problems, ie, white matter (WM) abnormality/extensive cortical abnormality;
haemorrhage, intraparenchymal or extracerebral;
evidence of long-standing established injury;
unusual patterns of injury or SI suggestive of metabolic or infective disorders.
Outcome
At a minimum age of 24 months, surviving infants had a standardised neurological examination,22 23 Griffith neurodevelopmental assessment24 and head circumference measurement.25 26 Normal outcome was defined as a developmental quotient (DQ) >85 with normal neurological examination.
Ethics approval for the brain MRI studies from the Hammersmith Hospital ethics committee and parental permission were obtained in all cases.
RESULTS
Infants
Twelve infants fulfilled the study criteria. All but one were white, five were male, one was a twin, and nine were first born. Five were outborn. Table 1 gives details of these infants, along with descriptions of perinatal and postnatal events.
Only one infant, a twin, was <3rd centile for weight, and two were ⩽9th centile. No infant had a head circumference ⩽9th centile. No infant had an abnormally low cord pH or persistently low Apgar scores, or required major resuscitation at birth. All infants were considered healthy, initially stayed with their mother, and were fed. One infant (case 7) born at 36 weeks weighing 1930 g was admitted at 2 h for grunting. He rapidly improved and was tolerating full feeds and ready for discharge to the postnatal ward at the time of unexpected collapse at 55 h.
Maternal and prelabour data
Median maternal age was 31 years (range 23–38). Two mothers had documented prior medical problems: one hypothyroidism and one a right-sided hemiplegia first noticed at 16 months of age and attributed to perinatal problems. Three mothers developed hypertension in the third trimester (33–35 weeks): in two this prompted induction of labour; the third mother did not require treatment and was normotensive at delivery. Three mothers mentioned concerns about fetal movements but >10 kicks were always noted in a 12 h period. One mother (case 5) was involved in a car accident 6 days before delivery; she was unharmed, and a cardiotocogram (CTG) was reported normal. No other intercurrent illnesses or acute events were noted antenatally.
Labour and delivery-related data
Labour started spontaneously in eight mothers and was induced in four (table 1); four labours were augmented with syntocinin. Three mothers had epidurals; no mother had a general anaesthetic.
Three fetuses had documented CTG abnormalities: one had fetal tachycardia thought to be secondary to maternal fever and two had early decelerations. In the other 10 mothers, CTG monitoring was continuous in seven and intermittent in two (in the water bath) and reported normal. Information was not available for one mother.
No infant was exposed to a sentinel event. Two mothers, one of whom had an epidural and one of whom laboured in a water bath, developed a fever ⩾37.5°C during labour (cases 1 and 10); neither had proven infection. The maximum length of membrane rupture was 24 h. The length of the second stage, available for 8/10 infants, was >2 h in four, maximally 170 min. The two mothers delivered by caesarean section for breech presentation were not in 2nd stage.
Seven infants were born by spontaneous vaginal delivery (including one occipitoposterior presentation, two water births), three were born vaginally by forceps, and two by semi-emergency caesarean section; none was born by elective caesarean section.
Placental information was available for only three infants. The histopathology was normal for one of the infants who had a post-mortem examination, and the placenta was reported to look normal for two other infants, both of whom also died.
PNC-related data
The median age at collapse was 75 min (range 10 min to 55 h). All infants required extensive resuscitation including cardiopulmonary resuscitation and intubation. The median pH after PNC was 6.75 (range 6.39–7.05) and base deficit 21.7 mmol/l (range 11.3–29.6).
Six infants appeared to collapse while feeding at their mother’s breast or within minutes of the first breast feed. Two infants were found collapsed having been sleeping with their mother. In 10 infants, colour change, pallor or collapse was noted acutely, and resuscitation was started immediately after concerns were raised. One infant (case 2) was found in her mother’s arms while she slept; this infant had no heart rate when found, and the time of collapse is unknown but thought to be within 1 h. One infant (case 8) was confirmed collapsed 20 min after birth and had a slow heart rate at that time; however, the father had been concerned that the infant was quiet for 10 min before this.
The infants had early electrophysiological monitoring and brain imaging as part of their clinical assessment. They underwent neurometabolic work-up as individually indicated, the range of investigations including amino acids, organic acids, ammonia, uric acid, urinary sulphite oxidase and blood and cerebrospinal fluid glucose, lactate, pyruvate, amino acids, very long chain fatty acids and carnitine profile. No result was diagnostically positive, although lactate concentrations were high in some infants initially but settled. C-reactive protein concentrations, blood cultures, virus isolation and PCR, and congenital infection screens were all normal/negative. No infant had clinical evidence of congenital malformations including congenital heart disease. All echocardiograms obtained (cases 2–4, 6, 8, 9, 12) showed normal heart structure. No infant had evidence of hypoglycaemia, anaemia, clotting or thrombophilic abnormality (full testing carried out in four infants, cases 1, 4, 6 and 8).
The subsequent postnatal course appeared to be most easily distinguished by the presence or absence of ongoing major respiratory disease.
Infants without respiratory disease (cases 1–8)
Seven infants (cases 1–7) required ongoing mechanical ventilation because of lack of respiratory drive after the collapse. However, all seven required minimal support (maximum positive inspiratory pressure 18 cm H2O, maximum fractional inspiratory oxygen 0.30). These seven infants were severely encephalopathic, and all had an abnormal aEEG or EEG with a burst suppression pattern (n = 3), isoelectric pattern (n = 3) or sustained seizure activity (n = 1) within 24 h of the collapse. Six of these seven were found breast feeding in their mother’s arms at the time of collapse. Their clinical state was consistent with hypoxic–ischaemic encephalopathy (HIE) stage 3.27 One infant (case 8) made a very rapid recovery after PNC, was self-ventilating in air within 10 min, and had no further respiratory difficulties. She was initially irritable, with high-pitched cry, hypertonic and hyper-reflexic and had one clinical seizure. An EEG recorded on day 4 had a normal background with no electrical seizures seen.
US scans
Six of the seven severely encephalopathic infants (cases 1–6) had cranial US scans on day 1: three were available for review (cases 2–4); two showed mild WM trigonal (cases 1 and 3) and one mild BGT (case 4) echogenicity 2 h after the collapse. The others were reported to be normal. Limited sequential scans were available for the group, but the pattern appeared to be of a swollen appearance to the WM on days 2–4 which settled, with BGT abnormality becoming increasingly obvious and persisting after day 2. The infant who survived to day 36 (case 3) developed small caudothalamic cysts. A US scan in case 8 was reported to be normal.
MRI scans
MRI scans were performed at median 4 days (range 1–9) after collapse in this group. All seven severely encephalopathic infants had findings typical of acute severe perinatal hypoxia–ischaemia (fig 1) with swollen featureless appearances and/or abnormal SI in the BGT and loss of the normal signal from PLIC.17 All also had brainstem injury evidenced by swelling and/or loss of the normal SI from myelination (fig 1). Four had additional cortical highlighting often seen with an acute recent hypoxic–ischaemic insult in term infants. Only two infants had “slit-like” ventricles as a marker of more generalised brain swelling; in three infants the ventricles were of normal size and in two they were mildly dilated.

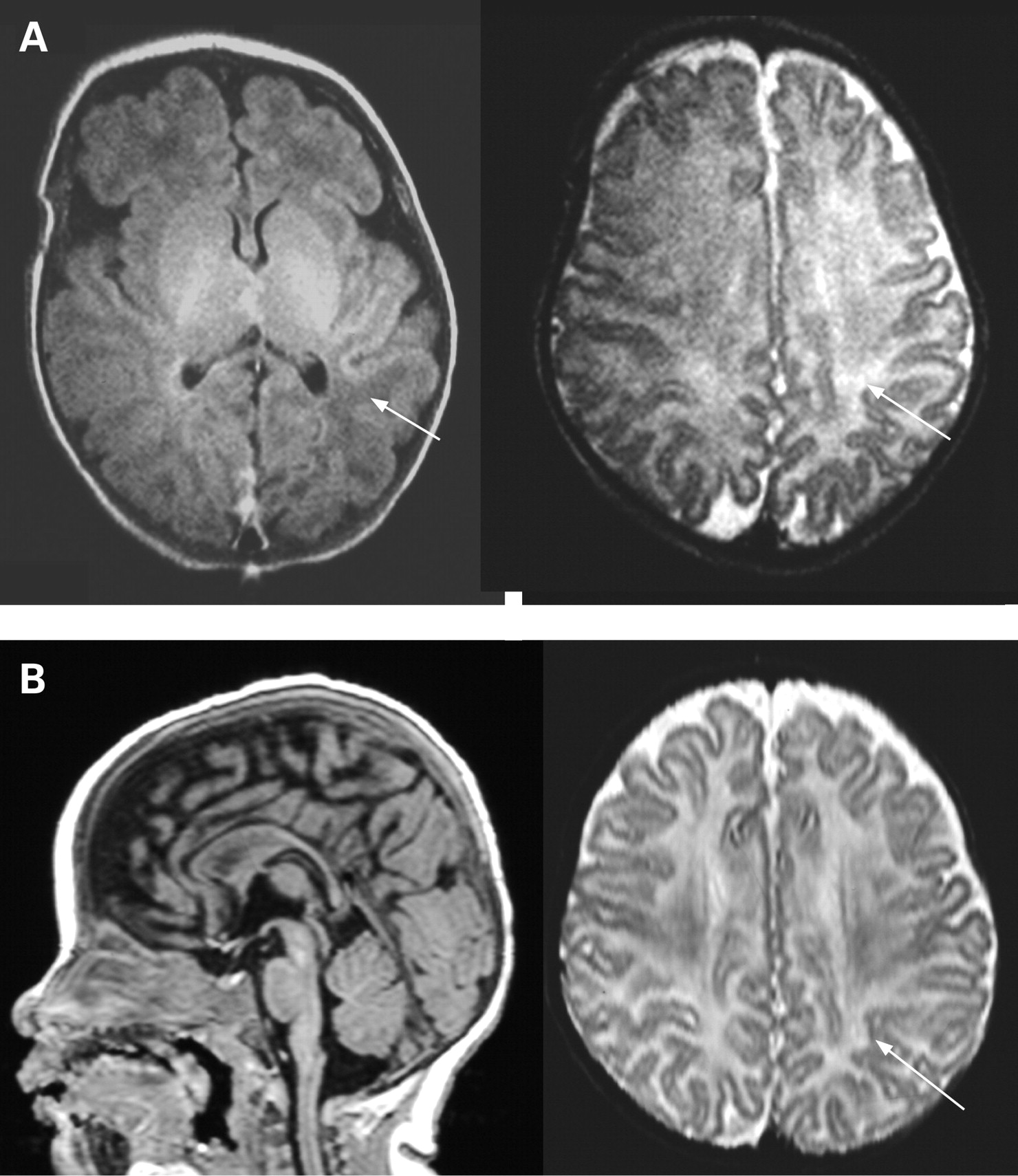
Case 5 imaged on day 9. Top row: axial T1-weighted images showing abnormally increased signal intensity (SI) in the basal ganglia and thalami (BGT) (A) with abnormally low SI in the posterior limb of the internal capsule (arrow). There is abnormally increased SI in the mesencephalon (B) and in the cortex along the central sulcus and the interhemispheric fissure (C). There is abnormally low SI in the white matter adjacent to the abnormal cortex (C). Middle row: axial T2-weighted images. The normal anatomical details in the BGT are lost (A). There is abnormally low SI in the thalami (A) and the mesencephalon (B). There is also increased SI in the thalami and to a lesser extent the putamen (A). There is some low SI in the cortex of the central sulcus (C) and multiple foci of abnormally high SI in the subcortical white matter (C), corresponding to the regions of low SI seen on the T1-weighted images. Bottom row: axial diffusion-weighted imaging. There is restricted diffusion, seen as low SI on the apparent diffusion coefficient maps in the brainstem (A), the internal capsule (B) and along the central sulcus in the region of the corticospinal tracts (C), marked with arrows.
All infants showed an abnormal appearance to the WM typically seen with hypoxia–ischaemia with low SI on T1-weighted images and high SI on T2-weighted images. In two infants, there were regions of more widespread loss of grey matter (GM)/WM differentiation. One infant had a small punctate WM lesion (case 4, fig 2). Six infants had evidence of extracerebral haemorrhage in the subdural space, three of whom also had small subdural haemorrhages around the cerebral hemispheres. A small punctate haemorrhagic lesion in the cerebellum was seen in case 3 on day 5 and mild vermis atrophy on day 13. The MRI scan of the mildly encephalopathic infant (case 8) showed a slight but similar WM change to the other infants but normal BGT and cortex, but had some extracerebral haemorrhage in the posterior fossa.

Case 4 imaged on day 3. Axial T1-weighted images (A), T2-weighted images (B) and apparent diffusion coefficient maps derived from diffusion-weighted images (C) at the level of the basal ganglia (left) and mid-ventricular level (right). There is loss of detail in the basal ganglia and thalami and no signal from myelin in the posterior limb of the internal capsule. There is a small punctate lesion, high signal on T1 and low signal on T2, in the posterior periventricular white matter on the right (arrow). It shows restricted diffusion (arrow in (C)).
DWI was available for five severely encephalopathic infants. All showed restricted diffusion in the BGT, indicating recent injury, and, in the three where DWI was acquired at the level of the brainstem, there was additional focal restriction within the corticospinal tracts. In one infant (case 5) imaged on day 9, the restriction was still very marked (fig 1). In a further infant (case 1), there was more widespread restricted diffusion involving the cortex and WM.
The imaging appearance in all seven severely encephalopathic infants was consistent with recent injury around the time of birth (figs 1 and 2). None showed changes consistent with injury established before delivery.
Gadolinium was used for case 1, which enhanced the cortical highlighting and the abnormal SI in the BGT. Case 2 had proton and phosphorus magnetic resonance spectroscopy, which showed a very high lactate peak, a normal N-acetylaspartate/creatine ratio, and a very low inorganic phosphorus/phosphocreatine ratio consistent with a recent acute severe hypoxic insult.
Outcome (table 2)
All seven severely encephalopathic infants died, six within 10 days of birth and one at 36 days. After discussion with their parents, all had intensive care discontinued because of the severe clinical, electrophysiological and neuroimaging findings. Three infants had a full autopsy examination, and the findings were consistent with the MRI appearances. These were selective neuronal cell death of the basal ganglia, thalamus, hippocampus region and ventral pons (pontosubicular necrosis), dentate and olivary nuclei, and cerebellar cortex with focal necrosis of the brainstem. No additional information about the cause of death was obtained from the autopsy. The infant with mild encephalopathy and mild MRI findings had a normal DQ, neurological examination and head growth at 2 years.
Infants with respiratory disease (cases 9–12)
Four infants had ongoing primary respiratory compromise after the collapse. All four showed a significant respiratory component to the acidosis (Pco2 11–20 kPa, base deficit 19–24 mmol/l). Three infants met diagnostic criteria for persistent pulmonary hypertension of the newborn (PPHN) with Pao2 6 kPa when ventilated in 100% oxygen, near-normal lung fields, normal cardiac structures and evidence of pulmonary to systemic shunting.28 All three infants required prolonged (>72 h) ventilatory support and treatment with inotropes and nitric oxide. Two infants were referred for, but did not receive, extracorporeal membrane oxygenation (ECMO). One infant (case 12) collapsed at 30 min after birth with evidence of respiratory distress syndrome but not PPHN; this infant required ventilatory support for 72 h and treatment with surfactant. No infant had positive cultures or other evidence of infection.
All four had a normal background cerebral function monitor/EEG, but two (cases 9 and 11) had one documented clinical seizure, and one (case 9) was irritable and hyperalert in the first 1–2 days consistent with HIE stage 127 and one (case 10) was thought to be floppy.
US scans
US scans were obtained for all four infants on day 1 and sequentially for three; three were available for review. On day 1, one showed diffuse swelling (case 10), one mildly echogenic WM and marked GM/WM contrast (case 11), and one slightly echogenic cortex adjacent to the interhemispheric fissure, but normal WM and BGT (case 12). The one that was not reviewed was reported to be normal. Of the three with early sequential scans, the WM became more swollen in appearance in two and the BGT in one; these findings settled in all three. In one (case 11), left anterior focal echogenicity was seen on day 6, becoming more marked on day 7; this infant had an infarct in this region on MRI. Two infants had later US scans, case 9 on day 17 and case 10 at 2 months; both showed a slightly increased extracerebral space, one with mildly echogenic WM and the later one with deep sulci and mild ventriculomegaly suggestive of a slight reduction in WM volume. This child also developed deep caudothalamic notches. One infant (case 12) developed small cysts in the caudothalamic notch by day 12.
MRI scans
One infant had an MRI scan on day 18 and at 4 months. Two infants had a single MR scan, one each at 2 and 7 months. One infant (case 10) did not have an MR scan but had serial US scans.
The infant with early MRI had some slight WM change with low SI on T1-weighted images and high SI on T2-weighted images (fig 3) but normal BGT and PLIC. On a later scan, this child showed a reduction in WM volume, as did the infant scanned at 7 months. The infant scanned at 2 months had an established small frontoparietal infarct in the territory of the left middle cerebral artery (fig 4), consistent with earlier US findings. This infant was referred for ECMO; he had two early normal US scans, with echogenicity becoming apparent on day 6, suggesting a postnatal timing of onset for this lesion. No haemorrhage was seen in this group.
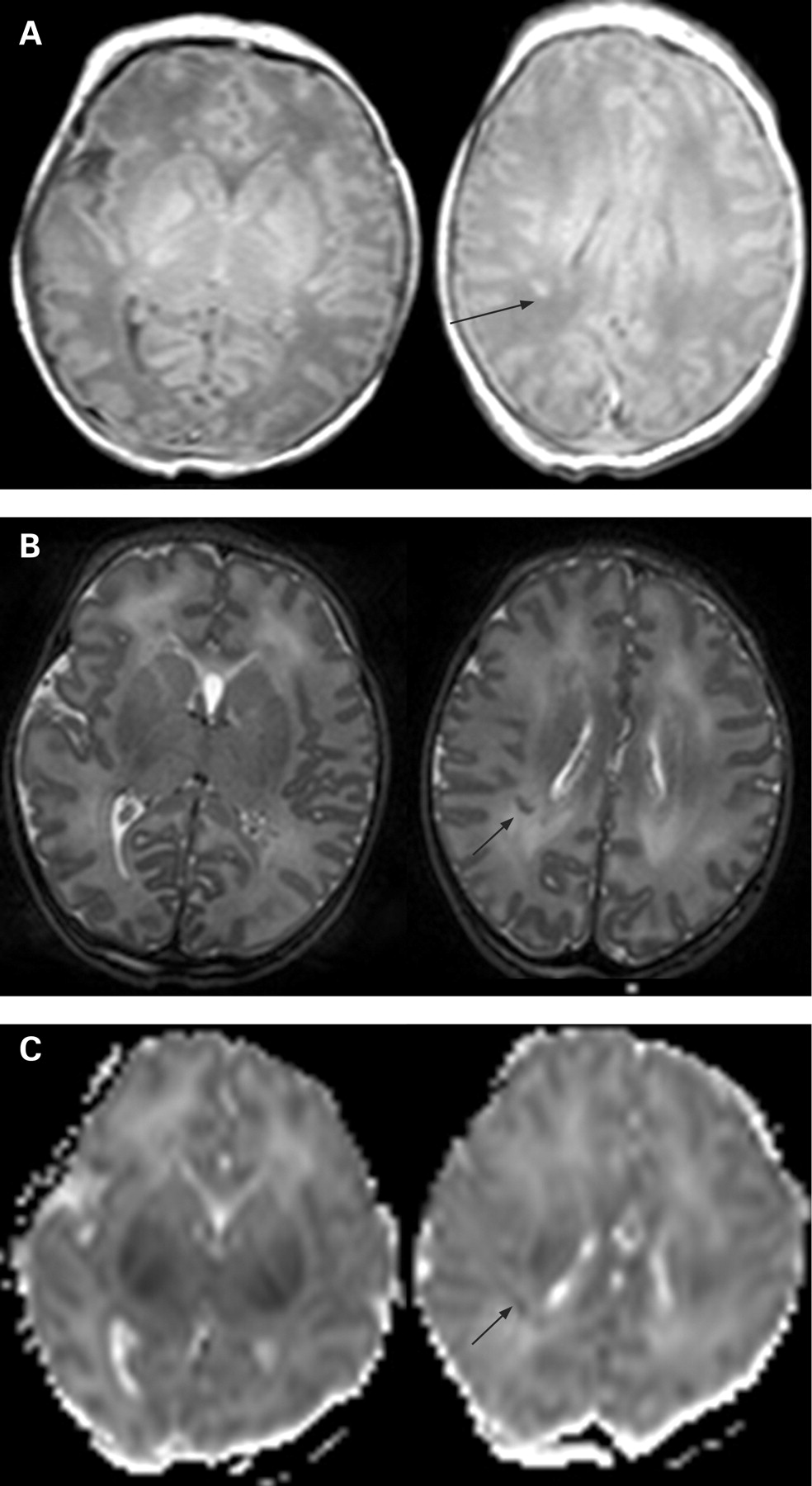
Case 9 imaged on day 18 (A) and at 4 months (B). (A) Axial T1-weighted (left) and T2-weighted (right) spin-echo images showing low signal intensity (SI) on the former and patchy high SI on the latter in the white matter (arrows) in the neonatal period. (B) The later T1-weighted sagittal (left) and T2-weighted (right) axial images show a slightly thin corpus callosum, an increased extracerebral space, and still some patchy long T2 in the white matter (arrows).
{kind=link}
{kind=link}
{kind=link}
{kind=link}
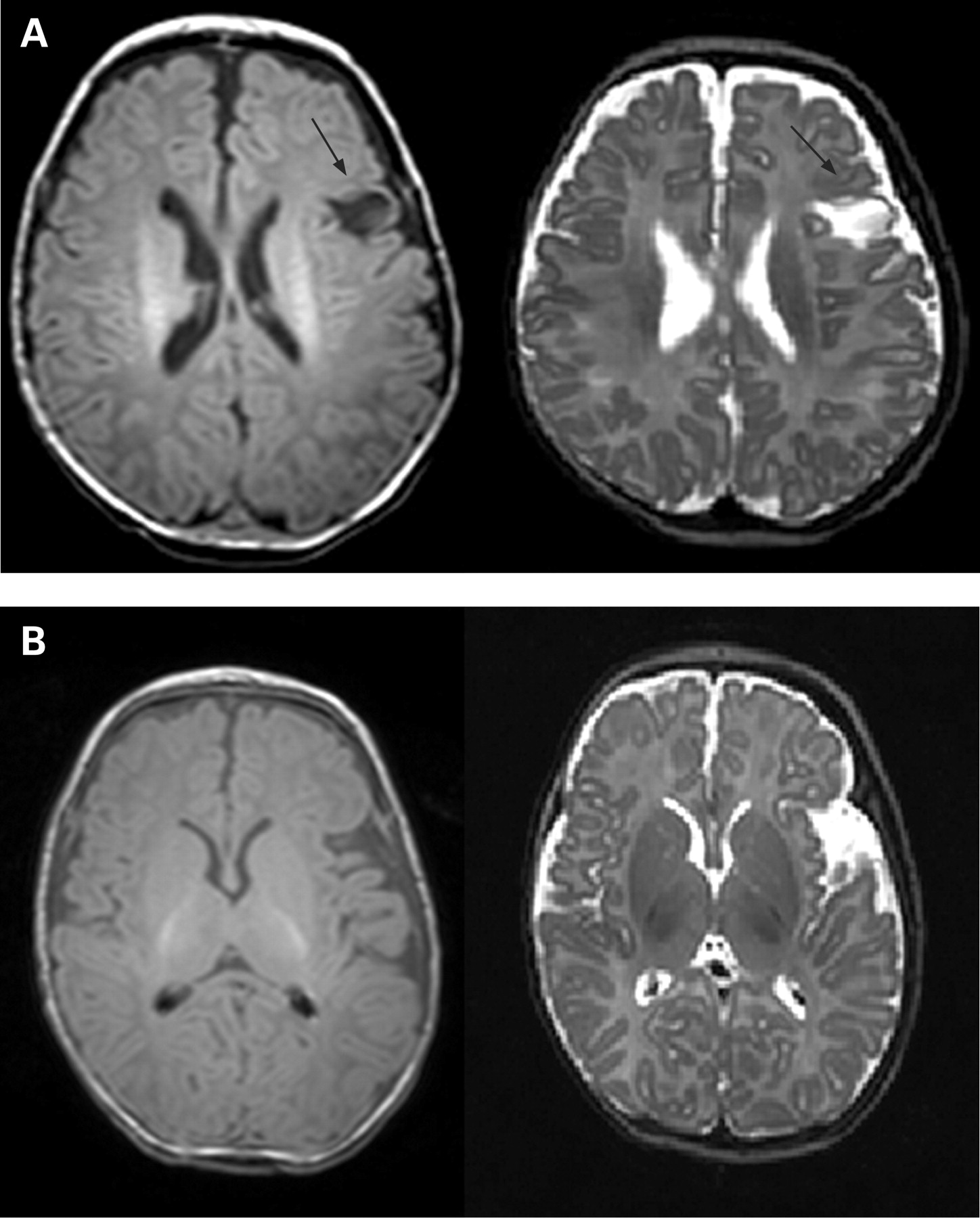
Case 11 imaged at 2 months. Axial T1-weighted (left) and T2-weighted (right) images. (A) There is a small infarct in the left parietal lobe (arrows). There is mild ventricular dilatation superiorly. (B) The appearances of the basal ganglia and thalami and posterior limb of the internal capsule are symmetrical and appropriate for age.
Outcome (table 2)
All infants in this group had DQs in the normal range (median 104, range 90–122). All children were able to walk independently and had a normal neurological examination; none had cerebral palsy. Two of the three children with WM change had a fall in occipitofrontal circumference centile at follow-up, in keeping with their US and MRI scans (table 2). The infant with middle cerebral artery infarct shows normal development at 2 years with no signs of hemiplegia and good head growth.
DISCUSSION
We report findings on presentation, clinical course, imaging, EEG and outcome of 12 near-term infants with acute severe PNC. These infants could be divided into two groups:
Group 1, with a primarily neurological abnormality. All but one were severely encephalopathic and had severe EEG abnormality and severe damage to the central GM and brainstem. All these infants died. One infant in this group had a mild encephalopathy, and probably represents a spectrum of encephalopathy occurring after collapse, as has been described previously.4
Group 2, with a primarily respiratory abnormality. These infants had near-normal brain imaging and EEG and a normal outcome.
Extensive metabolic and bacteriological investigation for both groups did not reveal any positive results. For both groups, findings from early neonatal electrophysiology and brain imaging aided early prognostication and guided management.
Infants in group 1 showed MRI evidence of recent hypoxic–ischaemic damage affecting the basal ganglia, PLIC and brainstem, consistent with injury around the time of birth. Information from autopsy was only available in three cases. This is disappointing given the difficulty in defining aetiology, but similar rates have been reported previously,1 where available autopsy supported the MRI findings. The marked abnormalities in the brainstem may represent the severity of the injury occurring at collapse or potentially the aetiology of the collapse. Two infants in group 1 had evidence of white matter change on US scan performed on day 1, suggesting distress before delivery. WM change tended to become more obvious in the first 3 days and then lessen, whereas, in those with central GM damage, this became more evident over the first few days after the PNC. Only one infant who had collapsed 10 min after birth had mild BGT echogenicity apparent within 2 h of collapse, suggesting an insult to this tissue a day or so before delivery.
This study was conducted over a long time period. Whereas imaging techniques have advanced, conventional MRI sequences and image interpretation in our experience have remained consistent, even at different field strengths. Although the advent of DWI has facilitated the early detection of injury, the severity of damage in group 1 was readily demonstrated using conventional MRI scans and was consistent with the clinical and pathological findings and outcome. Where we had DWI findings, they supported the acute and recent timing of the insult.
All but one infant in the non-respiratory group had posterior fossa and subdural haemorrhage over the hemispheres (table 2). Most were small, and subdural haemorrhage is reported in infants born by normal delivery29 and not necessarily attributable to excessive birth trauma. No infant had clinical evidence of clotting problems or disseminated intravascular coagulation, and extensive thrombophilic investigation in four infants produced results that were within normal limits. Although this observation is of interest, it is not possible to comment further on its significance in this small cohort.
The exact timing of injury in these infants is extremely difficult to ascertain. The possibilities are of late antenatal or intrapartum brainstem injury affecting the baby’s ability to maintain respiration or a primary airway compromise postnatally. The clinical, EEG, US and MRI changes for all infants were all consistent with a perinatal origin. The time from collapse to resuscitation was apparently very short, except for one infant for whom it could have been as long as 1 h. From this, it seems unlikely that, in the remaining infants, the injury happened as a result of the collapse unless perhaps it was accompanied by a complete cessation of the circulation; however, a heartbeat could be heard at the beginning of resuscitation in six infants.
We acknowledge that none of the infants showed convincing signs of perinatal asphyxia from the Apgar scores, which were normal, or from the cord pH values when available. Three infants had some fetal CTG concerns, but these were relatively minor. Of note, however, and in common with infants who develop focal arterial ischaemic infarction, few of the group had a simple normal vaginal delivery, and none was delivered by elective caesarean section.30 31
A possible explanation for the PNC was that interference with brainstem blood flow in the course of labour and delivery gave rise to brainstem injury. Infants with focal hemispheric lesions usually present with seizures some hours after birth and presumably some hours after the insult. It is possible therefore that infants with brainstem injury may also have a time lag between injury and presentation, but in these infants the presentation may be one of collapse rather than focal seizures because of the site of lesion and the period of hypoxia leading to further injury in the brainstem and basal ganglia. None of the infants who sustained brainstem injury regained self-ventilation.
Given that most of the infants collapsed within a few hours of birth, it would be very difficult to discriminate between damage occurring intrapartum and at the time of collapse, using either imaging or histopathological methods. The presentation in the group with severe neuronal injury seemed often to have a time relation to feeding—six of these infants were noted to have collapsed while feeding at their mother’s breast or within minutes of their first breast feed. This may be due to either the infants having suffered a mild generalised asphyxia or basal ganglia and brainstem injury impairing ability to coordinate feeding and respiration. Previous literature has suggested a primary mechanism of inadvertent suffocation in infants with early PNC, which is supported by risk appearing to be higher in first-time parents (nine of our 12 infants were born to primiparous mothers) and with early skin-to-skin contact.1 Although the benefits of skin-to-skin contact are not disputed,32 some authors have recommended close monitoring of parents and infants in the first postnatal hours.1 4 As this was a retrospective study, we do not have clear documentation of the infants’ position at the time of collapse; however, in our study only two were found sleeping with their mothers. The majority with poor outcome were found collapsed during or immediately after feeding.
Both gestational age and the nature of the asphyxial insult have a profound effect on the ultimate pattern of injury. It is interesting that the gestation of these infants was a little less than term, median 38 weeks (range 36–41); it has been found that acute severe hypoxic–ischaemic injury in more preterm infants tends to affect the lower basal ganglia and brainstem more than in more mature infants (P Logitharajah, M Rutherford, F Cowan, unpublished work).33
Four infants presented with a severe respiratory illness, requiring ventilation in 100% oxygen, with no evidence of sepsis, metabolic disease or congenital heart disease. These infants did not generally present in relation to feeding. Two of these four infants were delivered in a water bath and an association between water birth and respiratory distress, although controversial, has previously been reported.34–36 Two of the four infants had one clinical seizure (without EEG corroboration) and one had symptoms of stage 1 HIE, but none had evidence of severe injury on MRI and all had normal background EEG. They did, however, have some mild WM change and reduction in WM volume on follow-up; one infant had a small branch middle cerebral artery territory infarct, which was not evident until day 6 on US.37 It may be that this was a postnatal event associated with severe PPHN. All these children have a good outcome at 2 years, although longer-term surveillance is warranted. Head growth, although in the normal range, was on a lower centile than at birth in two infants, supporting the imaging evidence of mild WM injury,26 and three of the children also had an increased extracerebral space. The children may be at risk of attention and behavioural problems, as has been reported in children with milder WM injury,38 39 HIE40 or after ECMO.41–43
CONCLUSIONS
This series of infants present a rare but interesting entity, and, although no infant in this cohort was found to have an underlying metabolic or infective aetiology, investigation for these disorders is clearly warranted. As with more typical intrapartum asphyxial presentations, early electrophysiological monitoring and brain imaging (both US and MRI) are useful to guide prognosis and treatment. The outcome for those infants with early severe neurological problems was uniformly severe. Infants with severe respiratory disease but only mild or no encephalopathy had little evidence of brain injury and a normal developmental outcome. A multicentre study of all infants presenting with PNC is likely to increase our understanding of this rare but important condition.
REFERENCES
Footnotes
Funding: This work was supported by Philips Medical Systems (Best, The Netherlands), the Medical Research Council, the Academy of Medical Sciences, the NIHR Biomedical Research Centre Funding Scheme and the Health Foundation.
Competing interests: None.
Ethics approval: Obtained.
Patient consent: Parental consent obtained.
Linked Articles
- Fantoms