Article Text

Abstract
Background: Neonatal seizures are often subclinical, making accurate diagnosis difficult.
Objective: To describe the clinical manifestations of electrographic seizures recorded on continuous video-EEG, and to compare this description with the recognition of clinical seizures by experienced neonatal staff.
Methods: Term infants, at risk of seizures, were monitored by continuous 12-channel video-EEG from <6 hours of birth for up to 72 hours. All clinical seizures were recorded by experienced neonatal staff on individual seizure charts. Video-EEG recordings were subsequently analysed. The number, duration and clinical expression of electrographic seizures were calculated (in seconds), and compared with the seizures clinically suspected by the neonatal staff.
Results: Of 51 infants enrolled, nine had electrographic seizures. A further three had clinically suspected seizures, without associated electrographic abnormality. Of the total 526 electrographic seizures, 179 (34%) had clinical manifestations evident on the simultaneous video recording. The clinical seizure activity corresponded to 18.8% of the total electrographic seizure burden. Overdiagnosis also occurred frequently. Of the 177 clinically suspected seizure episodes documented by staff, 48 (27%) had corresponding electrographic evidence of seizure activity Thus, only 9% (48/526) of electrographic seizures were accompanied by clinical manifestations, which were identified and documented by neonatal staff.
Conclusion: Only one-third of neonatal EEG seizures displays clinical signs on simultaneous video recordings. Moreover, two-thirds of these clinical manifestations are unrecognised, or misinterpreted by experienced neonatal staff. In the recognition and management of neonatal seizures clinical diagnosis alone is not enough.
Statistics from Altmetric.com
Neonatal seizures are associated with a significant incidence of brain injury and long-term neurodevelopmental delay.1 2 Prompt therapeutic intervention may be important but recognition of seizures is hampered by a highly variable clinical expression and the frequent use of paralytic agents.3–5 In addition, anticonvulsant treatment often leads to electroclinical dissociation—that is, the number of clinical seizures decreases while the number of electroencephalographic (EEG) seizures continues unabated or increases.6 7 Certain neurological events previously considered to be seizures have also been thought to be either brainstem release phenomena or movement abnormalities.8 EEG confirmation is essential for the evaluation of neonatal seizures. The combination of both EEG and clinical criteria most accurately diagnose and classify all seizures in neonates.9 Because of the difficulty in deciding clinically whether a baby is seizing, clinical seizures may be overestimated, resulting in unnecessary treatment. Neonatal seizures may also be either underdiagnosed resulting in undertreatment, or incorrectly categorised resulting in potentially harmful treatment.10 11
Clinical observation of seizure semiology, unaccompanied by EEG confirmation, has severe limitations. Accordingly, the EEG plays an important part in understanding the nature of paroxysmal movements in neonates and in differentiating epileptic seizures from non-epileptic events.9 The aims of this study were to quantify the clinical manifestations of electrographic seizures in neonates precisely and to compare that with the clinical recognition of neonatal seizures by experienced neonatal personnel. We wished to determine the gap between electrographic seizure burden, video-recorded clinical manifestations of seizures, and clinical documentation of seizures in a population of term infants.
METHODS
This study took place in the neonatal intensive care units of the Unified Maternity and Neonatal Services in Cork between January 2003 and June 2005. The neonatal units (400 admissions a year) serve as tertiary regional referral centres for a population of 0.5 million (8500 births a year). Neonates were recruited into this study at birth if they fulfilled two or more of the following criteria: initial capillary or arterial pH <7.1, Apgar score <5 at 5 minutes, initial capillary or arterial lactate >7 mmol/l (normal newborn values <4 mmol/l) or abnormal neurology/clinical seizures. Infants’ neurological status was assessed by a standardised neurological method.12 In addition, neonates who did not fulfil these criteria at birth, but later developed clinical seizures, were recruited immediately after their first clinical seizure. Infants with either major congenital abnormalities or metabolic disorders were excluded from the study. The study was approved by the ethical committee of Cork University Hospital. Written informed parental consent was obtained for each participant. Clinical staff were not trained in EEG analysis and were unaware of the EEG findings. The digital EEG screen was set to non-display mode. Although staff were aware that studies on high-risk neonates were in progress, they did not know the specific study hypothesis. Anticonvulsant agents were administered for clinically suspected seizures only. Infants receiving neuromuscular blockade were excluded from the group. In addition to the initial neurological assessment, a clinical Sarnat score was assigned at 24 hours of age.
A bedside 16 channel Viasys NicOne Video-EEG system was used to record multichannel EEG using the 10–20 system of electrodes placement designed for neonates (F4, C4, T4, O2, Cz, F3, C3, T3, O1). The digital video-EEG recording was started as soon as possible after recruitment, usually at 3–6 hours after delivery, and recorded for 24–72 hours. Thoracic respiratory movements, heart rate, continuous invasive blood pressure (from radial or umbilical arterial catheter if available) and oxygen saturation, were also measured simultaneously. Only those neonates with either clinical or EEG seizures were included in the analysis.
EEG analysis
Each EEG recording was later analysed and electrographic seizures were distinguished from the continuing background activity by an experienced neonatal electrophysiologist (GBB). All seizures in each recording were counted and the duration of each seizure measured. An EEG seizure discharge was defined as a sudden repetitive stereotyped discharge lasting for at least 10 seconds on two or more EEG channels. In those infants with EEG seizures, the EEG seizure burden was calculated. This was defined as the number of electrographic seizure seconds in the total EEG recording. The time and duration of each electrographic seizure was also recorded. EEG epochs without clear simultaneous video recordings (for example if the infant was transiently obscured from view by staff, or equipment) were excluded from the analysis.
Video analysis
Clinical manifestations of seizures were determined by observation of the continuous video recordings. This was carried out at a later stage by a research paediatrician (DMM), not involved in the clinical care of the infants. The movements of the infants observed before, during and after each electrographic seizure episode were analysed. Clinical manifestations of the EEG seizures were classified as previously described by Volpe: subtle, clonic, tonic or myoclonic.13 Clinical seizure manifestations were defined as movements consistently associated with simultaneous abnormal electrographic discharges. The number and duration (in seconds) of clinical seizures were calculated for each infant.
Staff recognition of seizures
In the neonatal intensive care unit setting, experienced nursing and medical staff generally identify, and record, what they believe to be seizure activity. Nurses document the number and duration of each clinical seizure event on a seizure chart in the bedside medical notes. They are trained to use certain clinical strategies to differentiate clinically between epileptic and non-epileptic movements. These include stimulus response, response to soothing and response to gentle restraint. In addition, they are careful to recognise subtle movements as possible seizures. In our unit, specific seizure nursing sheets are maintained as a standard of care at the bedside of all infants. All recognised clinical seizure events and their time, type and duration are recorded on these seizure sheets.
RESULTS
Fifty-one infants were recruited to the study and had continuous EEG monitoring. Of these, 11 had clinically suspected seizures documented in the nursing/medical notes. One further infant had electrographic evidence of seizures which were unrecognised clinically. Our study focused on these 12 infants; table 1 gives their details.
In this study, the nursing seizure sheet, nursing notes and medical notes of each infant were examined retrospectively by a neonatologist (IA) following discharge of the infant from the neonatal unit. The number, time and description of the clinically suspected seizure events were noted. These were then compared with the video and EEG manifestations of seizures by a research paediatrician (DMM). A clinically suspected seizure was confirmed electrographically if there were electrographic seizure discharges at the time (within 5 minutes before or after the recorded time) of the clinically suspected seizure. This gap of 5 minutes before or after the documented time of onset was necessary to allow for minor discrepancies between staff recognition and documentation. Clinical seizures recognised by staff were recorded in minutes of seizure activity.
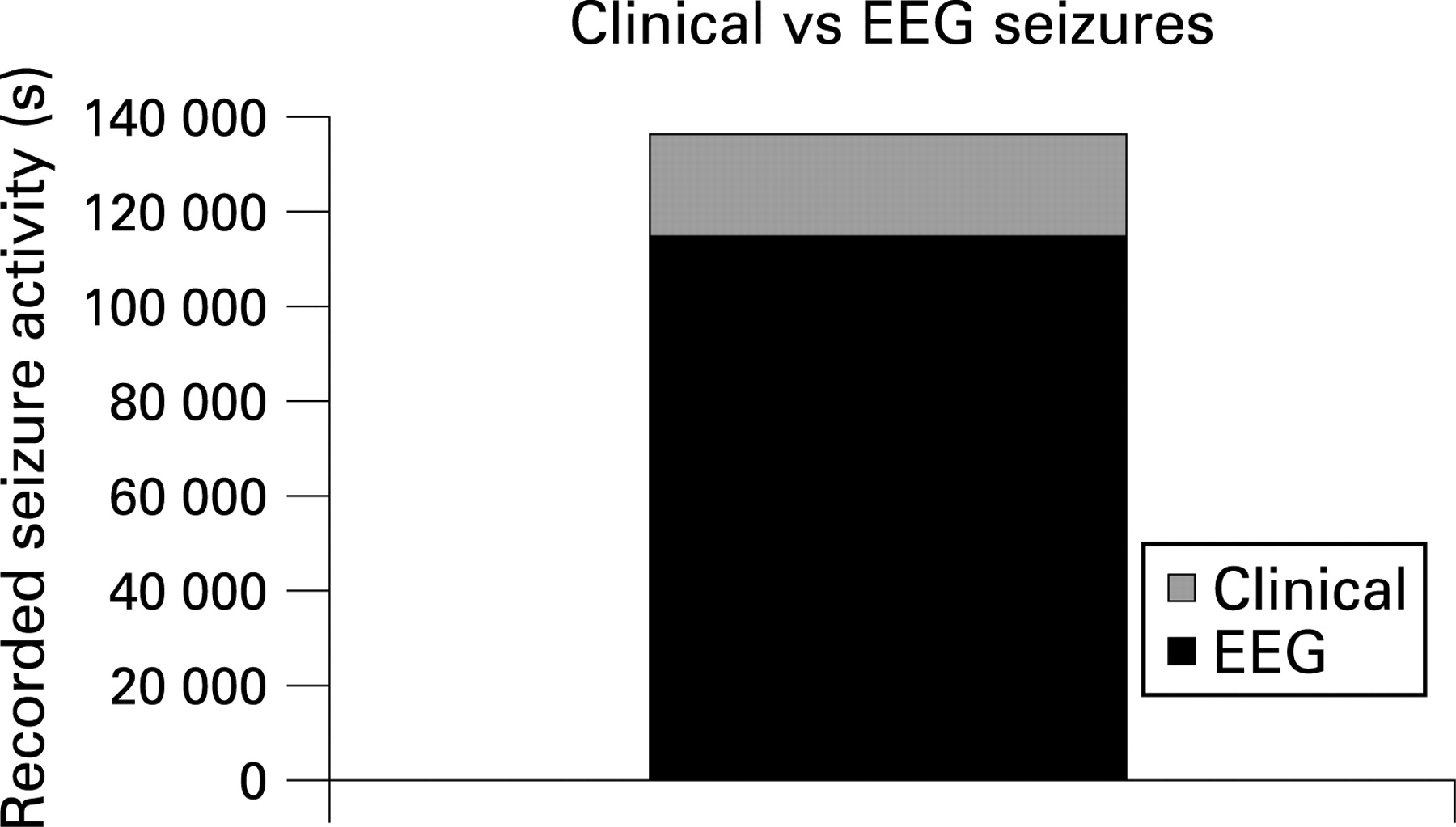
Electrographic seizures occurred in nine of the 12 infants. Clinically suspected seizures without electrographic evidence occurred in three of the 12 infants. The total number of EEG seizures recorded with simultaneous video-EEG was 526, with a total seizure burden of 112 987 seconds. Of these 526 seizures, only 179 (34%) had clinically recognisable seizure activity in the simultaneous video recording. The types of clinical seizures seen were clonic (125, 70%), subtle (42, 23%) and tonic (12, 7%). No myoclonic seizures were noted. All of the nine infants with electrographic seizures had clinical signs at some stage during their video-EEG seizures. Eight of the nine infants were recognised as having clinical seizures by nursing/medical staff (table 2).
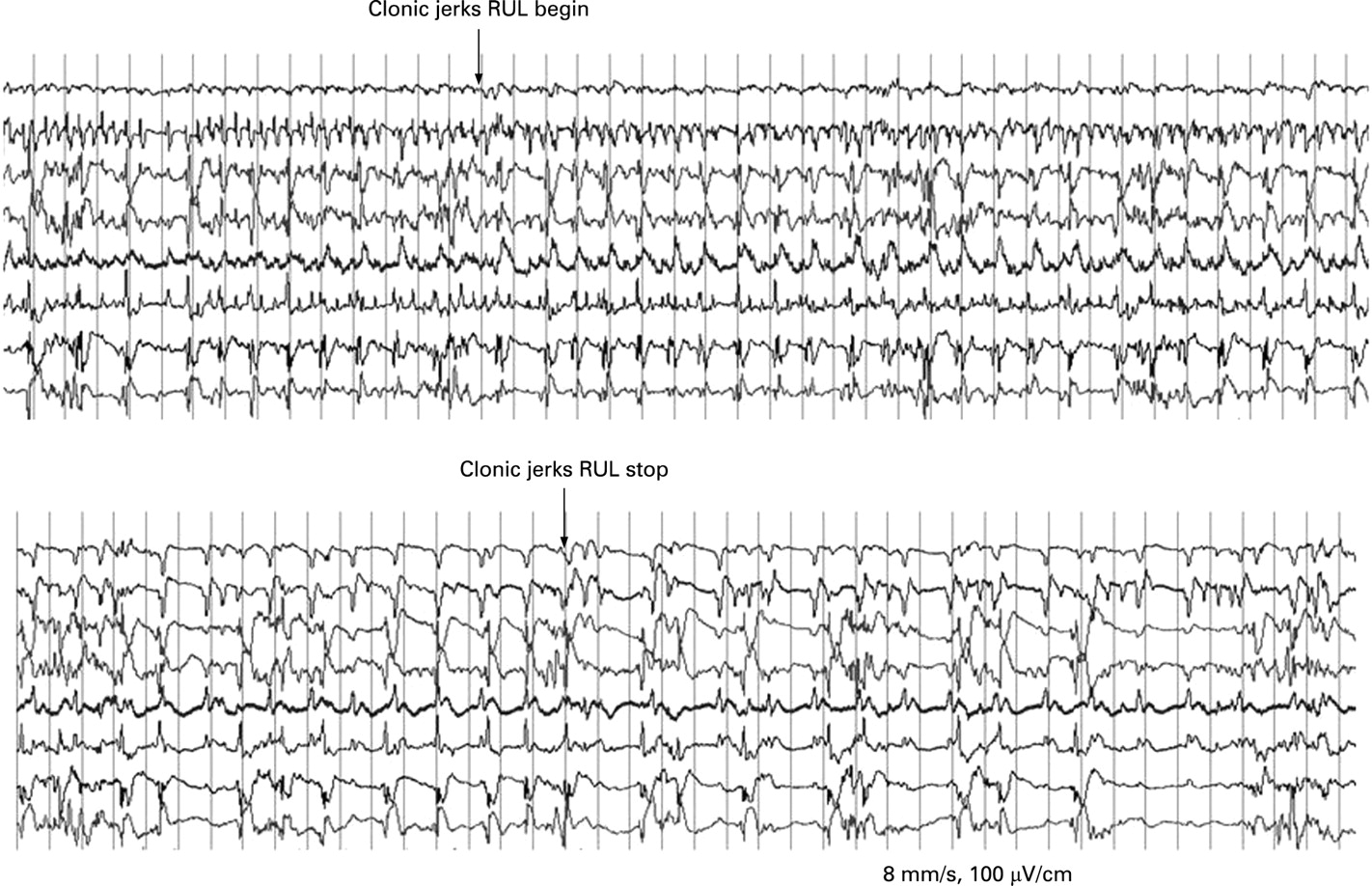
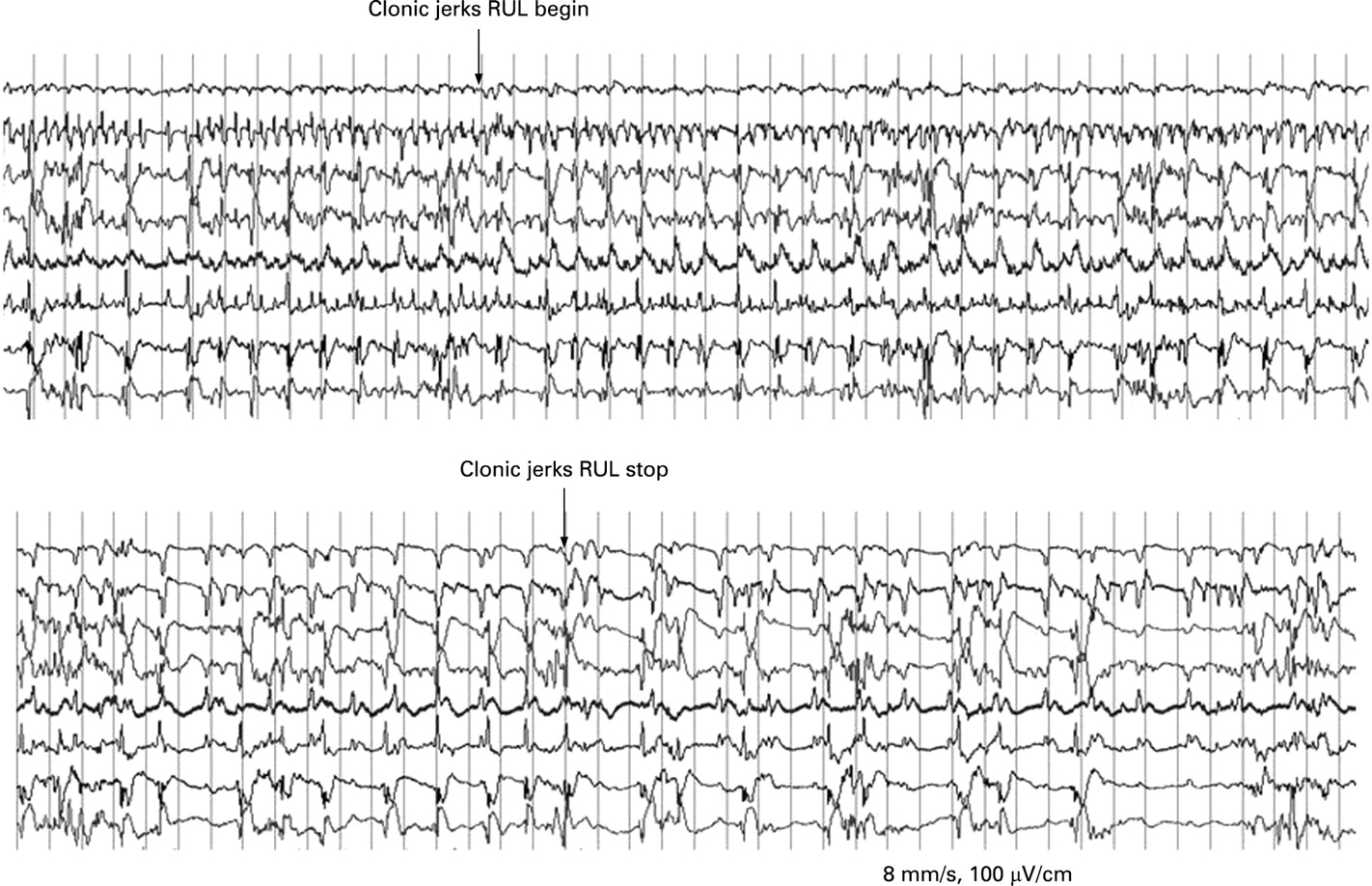
The mean duration of the clinical seizure manifestations, when they did occur, was shorter than that of the electrographic components (118 seconds and 215 seconds, respectively). In total only 18.8% (21 203/112 943 seconds) of the total electrographic seizure burden had obvious clinical signs on video-EEG (fig 1). An individual example from case 8 is shown in fig 2.
{kind=link}
{kind=link}
Clinically suspected seizure activity was recorded in the medical notes of 11/12 infants. In these 11 infants, the number of suspected seizure episodes was 177. Forty-eight of these events were confirmed to be electroclinical seizures on simultaneous video-EEG. In all only 48/526 (9%) electrographic seizures had clinical signs which were recognised and documented by nursing/medical staff. Table 3 gives the findings for each individual infant.
Only 48/179 (27%) of the seizures which had clinical features were recognised and recorded by medical and nursing staff. One patient (case 2) had 45 brief focal and multifocal clonic seizures recorded on video-EEG, none of which were documented by medical staff. The infant did not receive anticonvulsant medication despite having an electrographic seizure burden of 4668 seconds over 44 hours.
Overdiagnosis of seizures also occurred frequently, with 73% (129/177) of seizures documented in medical/nursing notes having no correlating electrographic seizure activity. Misinterpreted abnormal movements consisted of generalised muscle clonus/jitteriness, as well as subtle movements such as mouthing, and fisting. These movements occurred during periods of EEG with suppressed amplitude and no seizure activity.
Ten of the 12 infants had received anticonvulsant medication (phenobarbitone) before the initiation of video-EEG. Cases 2 and 9 did not receive anticonvulsants before, or during, the video-EEG recordings.
DISCUSSION
Our data confirm the extent of the unrecognised burden of subclinical seizures in neonates. Even with detailed review of continuous video-EEG monitoring, only 34% of electrographic seizures had overt clinical signs. This implies that even at its best, clinical detection of seizures will miss over 65% of neonatal seizures.
Previous video-EEG studies, recorded during attempts to treat electrographic seizures, have reported that only 15–20% of all neonatal seizures have clinical manifestations.14 15 We have shown that the number of correctly identified and documented seizures is even lower (9%). This reflects the brief and focal nature of neonatal seizures. Although the majority (70%) of the clinical manifestations were clonic in nature, they often involved brief jerking of a single hand or foot. As the seizures progressed, the movements shifted from limb to limb. These signs were essentially the “tip of the iceberg” against a background of more prolonged electrographic seizures (fig 1). We found that only 23% of the clinical seizure manifestations were subtle in nature. This is similar to the results reported in previous detailed descriptions of seizures in term infants.3 9
Do subclinical seizures matter? Animal studies suggest that seizures cause neuronal apoptosis and impaired neurogenesis in the immature brain.16 17 Infants with hypoxic–ischaemic encephalopathy may be particularly susceptible to seizure-associated brain damage. Since 20–50% of infants with neonatal seizures experience later epilepsy,18 diagnostic accuracy is essential, particularly for the newborn who has prolonged electrographic seizures. Past studies have linked neonatal seizures with worse developmental outcome, but these studies were based on clinical diagnosis alone, with its inherent limitations.2 19 Despite the amount of electroclinical dissociation which we have demonstrated, 8/9 infants did, at some stage, have clinical seizures correctly identified by their carers, and received anticonvulsants. It is the extent of their subclinical seizure burden that remains unrecognised. Does it matter if we are unaware of the majority of their seizures burden? Only with detailed continuous video-EEG studies of electrographic seizures, and long-term neurological outcome, will we be able to answer these important questions.
What is already known about this topic
The greatest risk of seizures is in the neonatal period.
Neonatal seizures are associated with a high risk of long-term neurological deficit.
Neonatal seizures are difficult to diagnose accurately and may be subclinical.
We have also shown that overdiagnosis of seizures occurs frequently, with only 27% of clinically suspected seizures confirmed electrographically. Many of the movements identified correctly by staff as being abnormal (eg, fisting, mouthing, clonus) were not accompanied by electrographic discharges. These movements have been described by Mizrahi and Kellaway as “motor automatisms”, of uncertain origin.3 They may reflect brainstem release phenomena, or may be electrical seizures in deep cerebral structures, which are not transmitted to surface EEG electrodes. Although their aetiology remains unclear, their presence usually reflects a severe underlying encephalopathy, with an increased risk of concurrent electrographic seizures, adding to the confusion.
What this study adds
Only one-third of neonatal seizures have clinical expression on simultaneous video-EEG.
Only one-third of that clinical expression is correctly recognised by experienced neonatal staff.
Neonatal seizures are frequently overdiagnosed with inappropriate administration of anticonvulsants.
These factors led to three infants in our group receiving large doses of anticonvulsants unnecessarily. The possible adverse effects of unnecessary anticonvulsant treatment in critically ill neonates are important. Hypotension, hypoventilation resulting in the need for mechanical ventilation, and fatal cardiac arrhythmias have all been attributed to anticonvulsant treatment in the newborn period.10 11
We used a reduced electrode montage for EEG recording (12 channels) in this study. The reason for this was simply that it was easier and more practical to maintain the reduced number of electrodes over long recording periods (>24 hours). However, our EEG montage did comprehensively cover the head and included wide-spaced derivations to maximise seizure detection. In a study by Tekgul et al,20 a full electrode montage was compared with a reduced electrode montage (nine electrodes) for the ability to detect and characterise neonatal seizures and background electroencephalography (EEG). The sensitivity and specificity of the reduced montage for detecting electrographic seizures was 96.8% and 100%, respectively. For grading background abnormalities, the sensitivity and specificity of the reduced montage was 87% and 80%.
Most of the seizures which we recorded occurred after administration of phenobarbitone, which is known to increase electroclinical dissociation, and may partially explain the number of subclinical seizures seen in this study. However, our findings give an accurate reflection of the management of neonatal seizures in the neonatal intensive care unit. In most units, anticonvulsants are administered based on the clinical judgment of the staff. Clinical signs of seizures may stop, to the relief of all, with the electrographic seizure activity continuing unabated. Clinical signs, when they did occur were, on average, only half the duration of the underlying electrographic seizures. Our current armamentarium of anticonvulsants is limited to ineffective drugs with significant side effects.21 22 There is an urgent need for randomised controlled trials of a new generation of anticonvulsants in the management of neonatal seizures, involving continuous video-EEG monitoring, and more importantly, long-term developmental follow-up.
In conclusion, neonatal seizures are difficult to detect, diagnose and manage. Clinical diagnosis alone is not enough. Accurate, reliable and easily accessible EEG monitoring in neonates is an urgent need.
Acknowledgments
We acknowledge the help and support of the nursing staff of the Unified Maternity Services, and the parents and families of the infants involved in this study.
REFERENCES
Footnotes
Funding: This study was funded by a grant from the Irish Institute of Clinical Neuroscience and an interdisciplinary grant from the Health Research Board of Ireland.
Competing interests: None.
Ethical approval: Approved by the ethical committee of Cork University Hospital.
Linked Articles
- Fantoms