Article Text

Abstract
Objective: To determine the accuracy of three tests used to predict successful extubation of preterm infants.
Study design: Mechanically ventilated infants with birth weight <1250 g and considered ready for extubation were changed to endotracheal continuous positive airway pressure (ET CPAP) for three minutes. Tidal volumes, minute ventilation (V˙e), heart rate, and oxygen saturation were recorded before and during ET CPAP. Three tests of extubation success were evaluated: (a) expired V˙e during ET CPAP; (b) ratio of V˙e during ET CPAP to V˙e during mechanical ventilation (V˙e ratio); (c) the spontaneous breathing test (SBT)—the infant passed this test if there was no hypoxia or bradycardia during ET CPAP. The clinical team were blinded to the results, and all infants were extubated. Extubation failure was defined as reintubation within 72 hours of extubation.
Results: Fifty infants were studied and extubated. Eleven (22%) were reintubated. The SBT was the most accurate of the three tests, with a sensitivity of 97% and specificity of 73% and a positive and negative predictive value for extubation success of 93% and 89% respectively.
Conclusion: The SBT used just before extubation of infants <1250 g may reduce the number of extubation failures. Further studies are required to establish whether the SBT can be used as the primary determinant of an infant’s readiness for extubation.
- ET CPAP, endotracheal continuous positive airway pressure
- NIPPV, nasal intermittent positive pressure ventilation
- ROC, receiver operating characteristic
- SBT, spontaneous breathing test
- V˙e, minute ventilation
- Vte, expired tidal volume
- newborn
- positive pressure respiration
- respiratory function tests
- extubation
- very low birth weight
Statistics from Altmetric.com
- ET CPAP, endotracheal continuous positive airway pressure
- NIPPV, nasal intermittent positive pressure ventilation
- ROC, receiver operating characteristic
- SBT, spontaneous breathing test
- V˙e, minute ventilation
- Vte, expired tidal volume
The adverse effects of prolonged endotracheal intubation on the preterm infant include bacterial colonisation, sepsis, subglottic injury, and bronchopulmonary dysplasia.1 Thus extubation of ventilated infants as early as possible is desirable.2 The decision to extubate is usually based on clinical assessment, blood gases, and ventilator settings.3 However, up to 40% of infants weighing <1000 g who are extubated on these criteria require reintubation,4 suggesting that the ability of clinicians to predict successful extubation is limited.5 Reintubation is destabilising, traumatic, and may prolong the duration of mechanical ventilation and intensive care.3 Accurate prediction of readiness for extubation of preterm infants may reduce morbidity.
Pulmonary function tests to assess readiness for extubation of adults5–7 and children8,9 have included measures of respiratory muscle strength, respiratory drive, ventilatory reserve, lung function, and gas exchange. In newborn infants, pulmonary function tests10–12 and invasive tests assessing muscle strength13,14 were less informative than gestational age.
Respiratory drive is variable and sometimes inadequate in preterm infants. Spontaneous expiratory minute ventilation (V˙e) of intubated infants provides an assessment of respiratory drive.15 Most modern ventilators measure V˙e continuously and allow measurement during endotracheal continuous positive airway pressure (ET CPAP). Wilson and colleagues15 calculated the V˙e ratio (ratio of ET CPAP V˙e to ventilator V˙e) and found a ratio of >50% to have a positive predictive value of 86% for extubation success. In a randomised controlled study of infants of all gestations, the V˙e ratio was shown to reduce the time to extubation but not improve the rate of successful extubation.16
The aim of our study was to evaluate three tests of readiness for extubation in preterm infants. These were conducted during three minutes of spontaneous breathing on ET CPAP and included (a) measurement of V˙e, (b) calculation of V˙e ratio, and (c) the spontaneous breathing test (SBT), which the infant was deemed to have passed if there was no hypoxia or bradycardia during ET CPAP.
METHODS
Subjects/setting
The Royal Women’s Hospital, Melbourne, is a tertiary perinatal centre with over 5000 deliveries per year. This study was conducted between June 2003 and October 2004. Infants with a birth weight of <1250 g, ventilated using the Dräger 8000 plus (software version 3; Dräger Inc, Lubeck, Germany) for at least 24 hours, and thought by the clinical team to be ready for extubation were eligible. Infants were weaned by either reducing delivered tidal volume to 3.5 ml/kg using assist-control or reducing ventilator rates to 20–30 breaths/min on synchronised intermittent mandatory ventilation. The inspiratory time was 0.3 second, the positive end expiratory pressure 5–6 cm H2O, and inspired oxygen concentration ⩽40%. Extubation was considered if the infant had satisfactory blood gases and was breathing above the set ventilator rate. Sedation, when used, was stopped at least 12 hours before extubation. Methylxanthines were used before extubation or after extubation at the clinician’s discretion. Some infants were enrolled in a double blind trial of caffeine citrate versus placebo (the CAP trial).18 The endotracheal tube was suctioned within two hours of the study.
Manoeuvre
When the clinical team decided an infant was ready for extubation, the investigator switched the ventilator to ET CPAP at the same pressure as the positive end expiratory pressure setting. Airflow was measured using the sensor in the ventilator circuit just proximal to the ET tube. Airflow, integrated expired tidal volume (Vte), and respiratory rate were recorded at 200 Hz using Spectra software (Grove Medical, London, UK). Data were downloaded from the RS232 port of the ventilator during two minutes of mechanical ventilation immediately before ET CPAP and three minutes of ET CPAP. V˙e was the product of Vte and respiratory rate. Expiratory V˙e was used because, when there is an endotracheal tube leak, it is a more accurate measure of the volume of gas that enters the lungs than inspiratory V˙e. Mean respiratory rates, V˙e, and V˙e ratios were calculated. A failed SBT was recorded if the infant had either a bradycardia for more than 15 seconds and/or a fall in Spo2 below 85% despite a 15% increase in Fio2. At this point the study was stopped, and ventilation restarted. Heart rate was displayed on HP M1205A Omnicare monitors (Hewlett-Packard, Andover, Massachusetts, USA) averaging every five beats.
Clinical teams caring for the infants were not present during the test and were blinded to the results. All infants were extubated, regardless of the results of the test. Infants were extubated to either nasal CPAP using Hudson prongs or nasal intermittent positive pressure ventilation (NIPPV) at the clinician’s discretion.
The primary study outcome was reintubation within 72 hours of extubation. The indications for reintubation were specified a priori: (a) more than six episodes of apnoea requiring stimulation in six hours, or more than one significant episode of apnoea requiring bag and mask ventilation; (b) respiratory acidosis (Paco2 >65 mm Hg (>8.5 kPa) and pH<7.25); (c) Fio2 >0.60 to maintain Spo2 in the target range (90–95%). The use of NIPPV was not considered a failure of extubation.
The research and human research ethics committees of the Royal Women’s Hospital, Melbourne approved the study, and informed written consent was obtained before testing.
Statistical analysis
Review of nursery data collected in 2002 revealed a 25% failure rate. We hypothesised that V˙e measured during the three minute SBT would be lower in infants requiring reintubation. A sample size of 50 was planned to detect a difference of one standard deviation in mean V˙e in the group failing extubation, assuming an overall mean (SD) V˙e of 300 (50) ml/kg/min (power 80% and two tailed α of 0.05).
Continuous outcomes were compared by Student’s t test when normally distributed and by Mann-Whitney U test when skewed. Categorical data were assessed using the Fisher two tailed exact test. p<0.05 was considered significant. The ability of respiratory variables to accurately discriminate between successful and failed extubation was assessed using receiver operating characteristic (ROC) curves. ROC curves are constructed by plotting the true positive rate on the y axis against the false positive rate on the x axis. Analysing the area under the curve determines the predictive value of a diagnostic test. A value ⩽0.5 indicates no discriminatory value, and a value ⩾0.8 suggests high predictive value.19 Standard formulae were used to calculate sensitivity, specificity, and positive and negative predictive values and likelihood ratios. Statistical analyses were performed using SPSS version 11.5 (SPSS Inc, Chicago, Illinois, USA).
RESULTS
During the study period, 251 babies with a birth weight <1250 g were admitted. Sixty five were ventilated from birth for at least 24 hours. Parental consent was obtained for 50 infants (31 male, 19 female). All had respiratory distress syndrome. Forty one infants were weaned using synchronised intermittent mandatory ventilation and nine infants on assist-control. Extubation was successful in 39 (78%). There were no significant differences in gestational age, ventilator settings, internal diameter of ET tube, and birth or study weights between successfully and unsuccessfully extubated infants (table 1). Most (64%; 7/11) reintubations occurred in the first 24 hours (median 21 hours; range 1–71). Methylxanthines were used in 40 infants (23 before and 17 after extubation). Two infants never received methylxanthines and remained extubated. Eight infants were enrolled in the CAP study, and five were reintubated. Infants were extubated to either nasal CPAP (47) or NIPPV (three) as the primary mode of respiratory support. An additional 14 (28%) subsequently received NIPPV as rescue treatment for apnoea. Significant apnoea accounted for eight of the 11 reintubations.
Basic and clinical data on the study infants
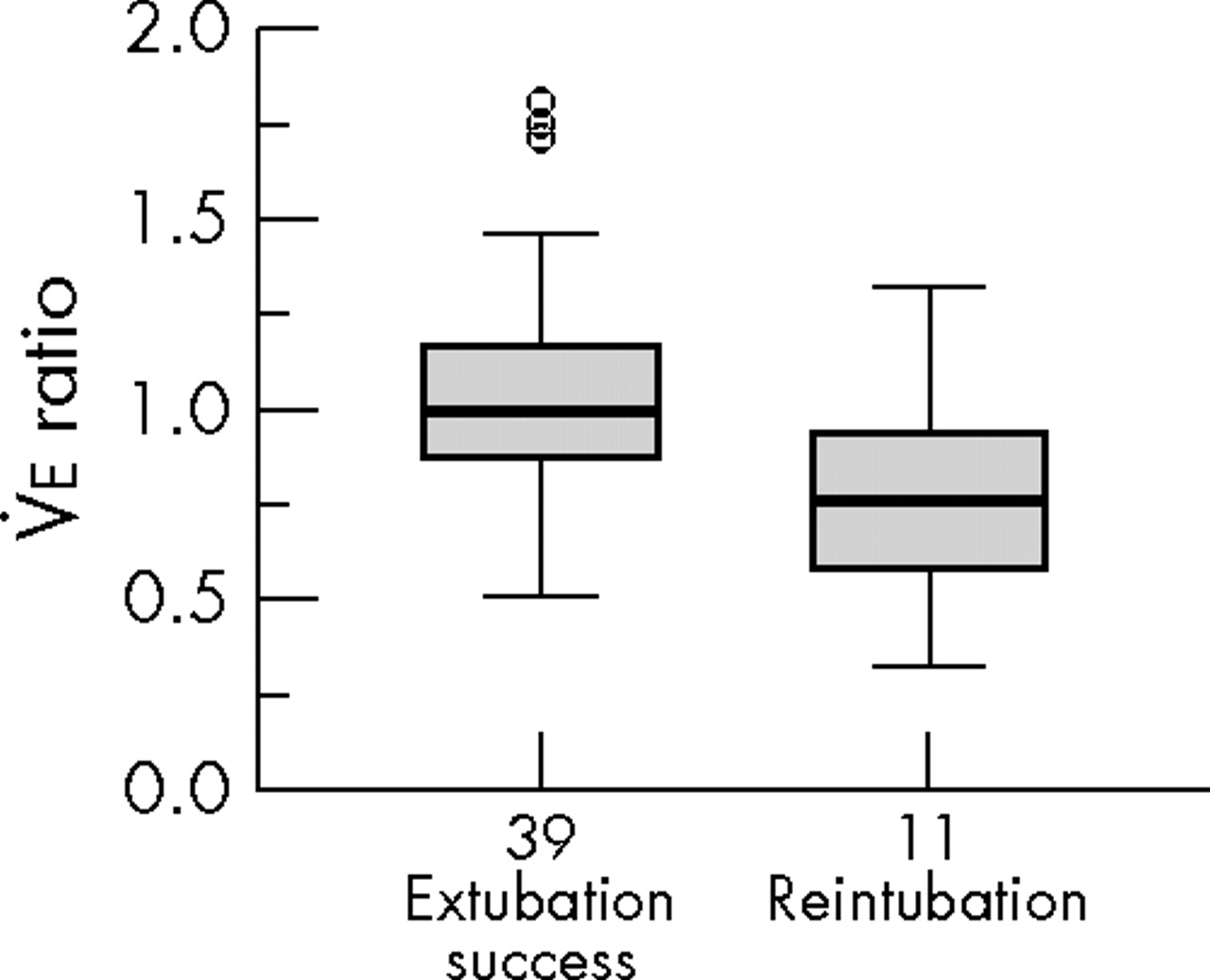
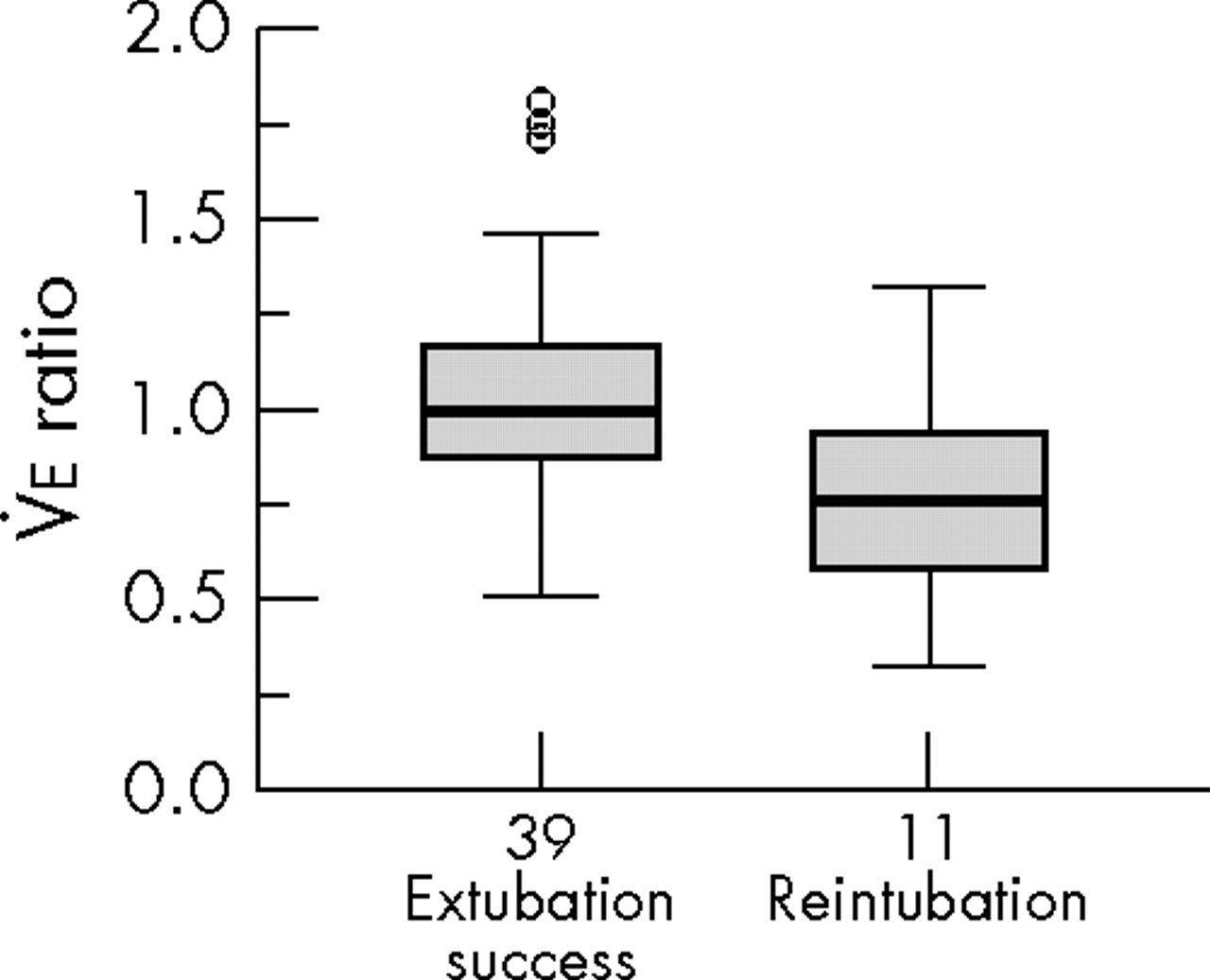
The mean (SD) V˙e during ET CPAP was greater in successfully extubated infants (314 (116) v 271 (113)), but the difference did not reach statistical significance. Figure 1 compares the V˙e ratios for the infants who were successfully extubated with those reintubated. Although median V˙e ratios were lower in infants who were reintubated (p = 0.015), there was considerable overlap between the groups.
{kind=link}
Minute ventilation (V˙e) ratios (ratio of endotracheal continuous positive airway pressure V˙e to ventilator V˙e) in infants who were either successfully extubated or reintubated. Comparison of medians (Mann-Whitney) p = 0.015.
Table 2 presents the area under the ROC curves and the 95% confidence intervals. The inflection points of the ROC curves were 220 ml/kg/min and 0.8 for V˙e and V˙e ratios respectively.
Variables predicting success or failure of extubation by ROC curve analysis
Accuracy of the SBT was greater (higher sensitivity, specificity, positive and negative predictive values) than the other two tests (table 3). Only three infants who passed the SBT were reintubated; one developed apnoea 71 hours after extubation, one was intubated for respiratory acidosis and an increasing oxygen requirement, and one developed stridor soon after extubation.
Summary statistics for the three variables used to predict extubation success
DISCUSSION
Our study was designed to determine the accuracy of three tests (V˙e, V˙e ratios, and the SBT) in preterm infants judged ready for extubation on clinical grounds. In our study population, the SBT performed better than both V˙e and V˙e ratios.
This pragmatic observational study investigated infants who were considered by clinicians to be ready for extubation. Our findings suggest that, if used to guide timing of extubation, the SBT, although not infallible, may result in fewer extubation failures and a greater proportion of successful extubations. False positive tests, such as those seen in two infants in this study (one with apnoea associated with subsequent sepsis and one with upper airway obstruction), are unlikely to be anticipated by any test at the time of extubation.
Infants who are immature and recovering from respiratory distress syndrome are at greatest risk of complications of prolonged mechanical ventilation. However, it is not easy, even for experienced clinicians, to determine when these infants have sufficient respiratory drive to tolerate extubation. It is not surprising that reported rates of reintubation vary from 15% to 40%.3,4,10,12–14,16,17,20,21 This variability is largely due to differences in study population. Only four studies investigated extubation of preterm infants.4,11,12,17 We limited our study to infants <1250 g because they represent the majority of intubated infants and are at highest risk of extubation failure. Accurate tests of readiness for extubation would be a valuable addition to the clinical armamentarium. Studies examining respiratory muscle strength are invasive and need expert application and interpretation. This and measurements of lung volumes after extubation limits their clinical utility.13,14,21 Measurements of dynamic compliance, Vte, V˙e, and lung volumes have not provided clear threshold values for reliable discrimination between extubation success and failure.3,6,8,10–12,14,20
The optimal duration of a trial of spontaneous breathing before extubation to determine an infant’s independent breathing ability is uncertain. An adult study compared 30 and 120 minutes and found no differences in safety or rates of extubation success.22 Vento et al17 measured mean V˙e of infants <1000 g during a two hour period on ET CPAP and concluded that the test “could be useful” in identifying an infant’s readiness for extubation. However, ET CPAP adds to the resistance of the respiratory system23 leading to increased work of breathing, potentially jeopardising successful extubation. There is evidence that extubation after several hours of ET CPAP is less successful than extubation from low rate ventilation.24 Published studies evaluating V˙e ratios used 10 minutes,15,16 whereas Veness-Meehan and coworkers6 measured Vte during one minute of ET CPAP. Before conducting this study, we observed that most infants who failed a trial of ET CPAP did so in the first 90 seconds. Our results suggest that three minutes is long enough to identify most infants who would fail extubation without risking fatigue. The advantages and potential benefits of the SBT are that it is easy to apply using standard monitoring devices in the neonatal intensive care unit and simple to interpret.
What is already known on this topic
-
Prolonged endotracheal intubation of preterm infants is associated with short and long term morbidity
-
At present there are no accurate tests for predicting readiness for extubation, and up to 40% of extubated infants require reintubation
What this study adds
-
Compared with measures of minute ventilation, information from a three minute period of endotracheal CPAP in infants considered ready for extubation is more likely to identify those likely to require reintubation
-
The spontaneous breathing test is simple to apply and easier to interpret than other predictors of extubation success
In summary, we have shown that a simple three minute SBT has a high negative predictive value when used in a unit with access to both NCPAP and NIPPV to optimise management after extubation. Whether this test can be applied earlier in the course of weaning to reduce the duration of mechanical ventilation remains to be investigated.
Acknowledgments
COFK is supported by a Research Scholarship from the Royal Women’s Hospital, Melbourne, and PGD is supported by an Australian National Health and Medical Research Council Practitioner Fellowship.
REFERENCES
Footnotes
-
Published Online First 12 January 2006
-
Competing interests: none declared