Article Text

Abstract
Background: A significant and prolonged decline in the incidence of necrotising enterocolitis (NEC), nearing virtual elimination in some centres, has been observed consistently since implementation of a standardised feeding regimen.
Aim: To systematically review the observational studies reporting incidence of NEC in preterm, low birth weight (LBW) neonates “before” and “after” implementation of a standardised feeding regimen.
Methods: The Cochrane Central Register of Controlled Trials (CENTRAL, The Cochrane Library, Issue 4, 2002), Medline, Embase, Cinahl, and proceedings of the Pediatric Academic Societies (published in Pediatric Research from 1980) were searched in July and again in October 2003. The reference lists of identified observational studies, and personal files, were searched. No language restriction was applied. Key words were: standardised, enteral, feeding, neonates, necrotising enterocolitis. Authors were contacted for clarification of data.
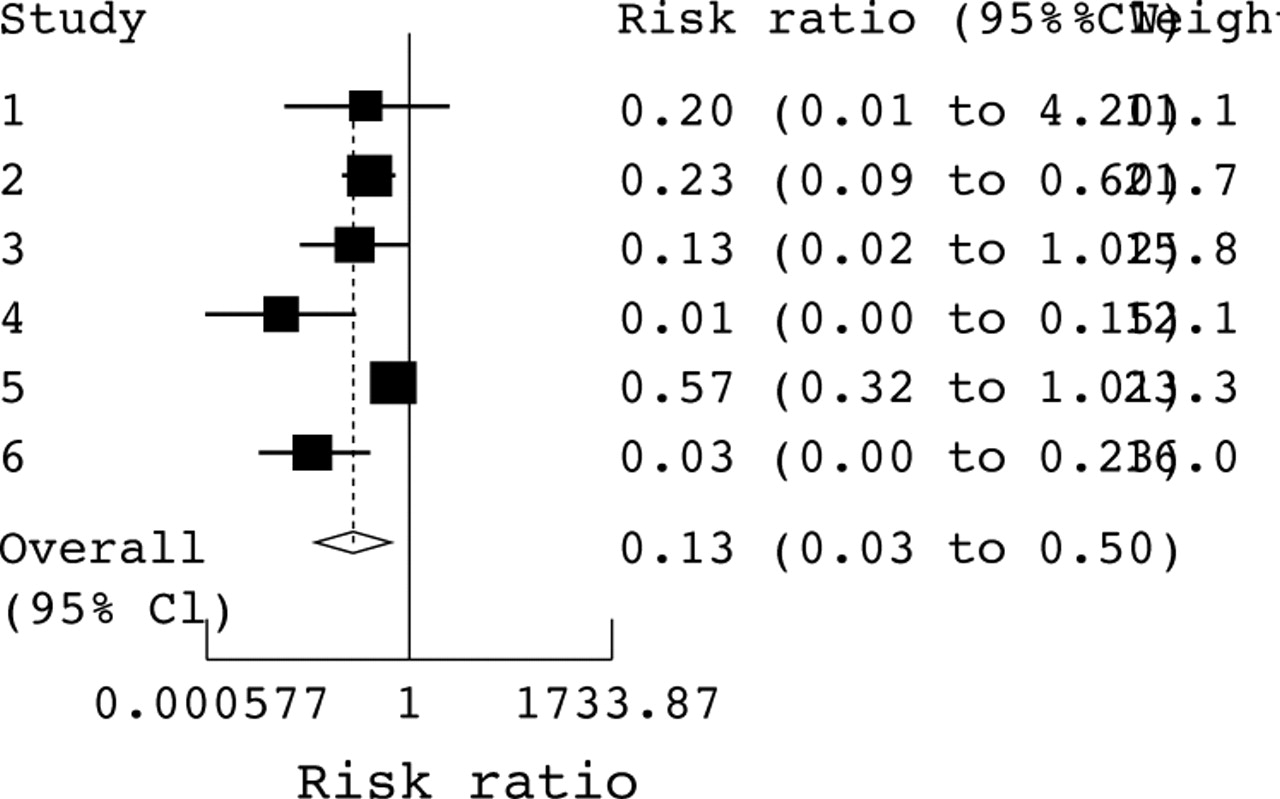
Results: Six eligible studies (1978–2003) were identified. A significant heterogeneity was noted between the studies indicating the variations in the population characteristics and feeding practices over a period of 25 years. Meta-analysis of the six studies using a random effects model revealed a pooled risk ratio of 0.13 (95% confidence interval 0.03 to 0.50)—that is, introduction of a standardised feeding regimen reduced the incidence of NEC by 87%.
Conclusion: Standardised feeding regimens may provide the single most important global tool to prevent/minimise NEC in preterm neonates. Randomised controlled trials are needed.
- CPG, clinical practice guidelines
- LBW, birthweight
- NEC, necrotising enterocolitis
- PDA, patent ductus arteriosus
- SFR, standardised feeding regimen
- VLBW, very low birthweight
- necrotising enterocolitis
- feeding
- nutrition
- preterm
Statistics from Altmetric.com
- CPG, clinical practice guidelines
- LBW, birthweight
- NEC, necrotising enterocolitis
- PDA, patent ductus arteriosus
- SFR, standardised feeding regimen
- VLBW, very low birthweight
Necrotising enterocolitis (NEC) is the most common gastrointestinal emergency in neonates. The result of dramatic advances in perinatal/neonatal care has exposed preterm neonates now living longer to a higher risk of NEC.1 Currently no single specific preventive strategy exists for NEC. Many consider NEC as almost unpreventable given its poorly understood pathophysiology, and the difficulties in preventing prematurity, the single most important risk factor.2 Besides prematurity, only enteral feedings have a firm association with NEC, considering that only 10% of the cases occur in neonates who have never been fed.3,4 Epidemiological data strongly suggest that NEC has an iatrogenic component related to variations in clinical practices including feeding strategies.5,6 A significant and prolonged decline in the incidence of NEC, nearing virtual elimination in some centres, has been reported consistently since implementation of a standardised feeding regimen (SFR) in the form of clinical practice guidelines (CPG).7,8,9,10,11 A systematic review and meta-analysis was therefore conducted to test the hypothesis that the incidence of ⩾ stage II NEC in low birthweight (LBW: birth weight <2500 g) neonates is decreased after implementation of a SFR.
METHODS
Only observational studies reporting the incidence of definite or ⩾ stage II NEC in preterm, LBW neonates “before” and “after” implementation of a SFR were considered eligible for inclusion.12,13 The presence of well documented guidelines for enteral feeding rather than their fine details was important for inclusion of any study in the analysis. The Cochrane Central Register of Controlled Trials (CENTRAL, The Cochrane Library, Issue 4, 2002), Medline, Embase, Cinahl databases, and Proceedings of the Pediatric Academic Societies (published in Pediatric Research from 1980) were searched in July and again in October 2003. The reference lists of identified observational studies, and personal files, were searched. No language restriction was applied. The following key words were used: standardised, enteral, feeding, neonates, and necrotising enterocolitis. Authors were contacted for clarification of data or additional data. Data were independently extracted by both the investigators and cross checked to avoid any errors. Any inconsistencies were sorted out after discussions and agreement. Assessment of study quality was not performed in view of the strict criteria for inclusion. No funding was needed for the study. A subgroup analysis of data on very low birthweight (VLBW) neonates was also planned given their higher risk of NEC. The guidelines for reporting meta-analysis of observational studies were followed.14 Data analysis used the program Metan (M J Bradburn, J J Deeks, D G Altman. sbe 24; Fixed and random effects meta-analysis STB 44) in software package STATA (StataCorp 2003; Stata Statistical Software: Release 8.0. StataCorp LP, College Station, Texas, USA)
RESULTS
Six eligible studies (1978–2003) were identified reporting incidence of ⩾stage II NEC in preterm, LBW neonates before and after implementation of a SFR.7,8,9,10,11,15,16Tables 1 and 2 summarise the characteristics of these studies and the SFRs reported in them. Meta-analysis of these studies using a random effects model estimated a pooled risk ratio of 0.13 (95% confidence interval (CI) 0.03 to 0.50)—that is, introduction of a SFR reduced the incidence of NEC by 87% (fig 1). Although all studies showed a lowered risk of NEC after adoption of a SFR, there was, as expected, significant heterogeneity (p<0.001) between the studies, indicating the variations in the population characteristics and standards of neonatal care, including feeding practices over a period of 25 years.
Characteristics of studies included in the analysis
Summary of feeding guidelines (part I)

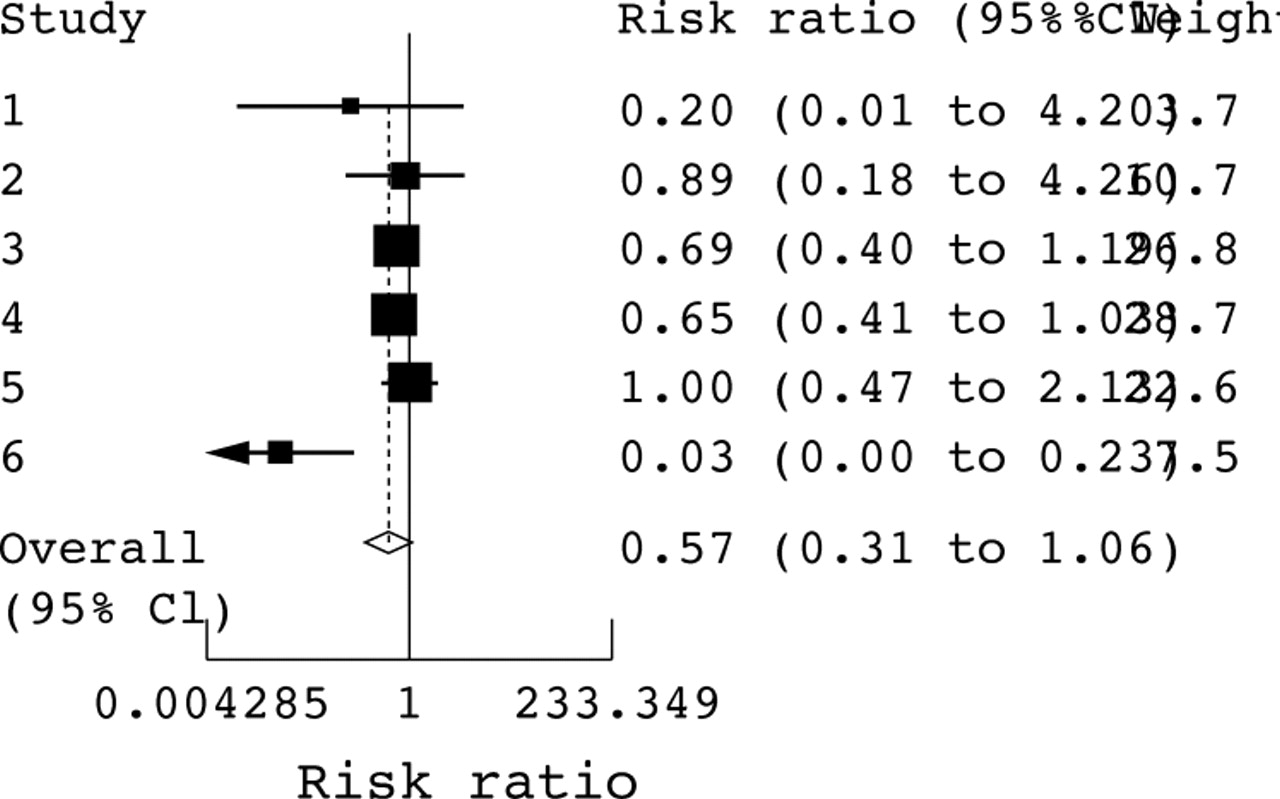
Given that VLBW neonates are at a higher risk of NEC and its complications, and that neonatal care has dramatically advanced in recent years, a preplanned subgroup analysis was conducted for VLBW neonates in the studies from the surfactant era.9,10,15,16 Authors KMD and KRB were contacted for specific data on VLBW neonates. The results revealed less of a protective effect of SFR on the incidence of NEC (pooled relative risk (RR) (95% CI) 0.57 (0.31 to 1.06), p = 0.08, heterogeneity p = 0.02; fig 2). The study by Patole et al showed the strongest protective effect of SFR (RR (95% CI) 0.03 (0.004 to 0.227)). Repeat analysis after exclusion of this study, although resulting in an increased pooled risk ratio, indicated a more significant effect because the lack of heterogeneity resulted in a much lower variance (pooled RR (95% CI) 0.71 (0.52 to 0.97), p = 0.03, heterogeneity p = 0.8; fig 3). Overall the results indicated that any SFR results in a 29% (95% CI 3% to 48%) decrease in the risk of NEC. Analysis of all studies, excluding that by Patole et al, was also performed using a fixed effects model, with almost identical results.

{kind=link}
{kind=link}
Subgroup analysis for very low birthweight neonates from four studies: 1, Premji et al15; 2, Kamitsuka et al9; 3, Kuzma-O’Reilly et al16; 6, Patole et al.10,11 The data from the three participating centres in Kuzma-O’Reilly et al are presented separately (studies 3–5). CI, Confidence interval.
DISCUSSION
Our results indicate that any SFR will reduce the risk of NEC. The benefit of SFR could be related to minimisation of variations in enteral feeding practices as well as an increased awareness leading to early detection and management of signs of “feed intolerance” (⩾ stage I NEC). Variations in clinical practice have been proposed to be the “iatrogenic” component of NEC.5,6 In a study of biodemographic and clinical correlates of NEC, intercentre differences in clinical practice involving fluid balance, patent ductus arteriosus (PDA) management, and feeding regimens were proposed to be the significant factors linked to the prevalence of NEC in VLBW neonates.5 The two centres with the highest prevalence of NEC had the shortest times required to regain birth weight. Similarly the centre with the lowest prevalence of NEC had the longest median time required to regain the birth weight. No other illnesses in this study group, including PDA and respiratory distress, were significantly different from one centre to another, strongly suggesting that clinical practices determine the risk of NEC. The centres that practiced fluid restriction in the management of haemodynamically significant PDA had a higher prevalence of “suspected” NEC. The centres practising no fluid restriction for such PDA had a higher prevalence of “definite” NEC.5 Variations in enteral feeding strategies for preterm neonates have also been reported recently by Patole et al.17 Given such evidence and the consistent reports of a significant and prolonged decline in the incidence of NEC after implementation of a SFR, it is almost certain that variations in clinical practice contribute to the incidence of NEC.
The significant heterogeneity noted between the studies indicates the variations in the population characteristics and standards of neonatal care, including feeding practices, over a period of 25 years. Some of the specific issues related to the reasons for developing the SFRs, constituents of SFR, and heterogeneity need to be discussed.

Subgroup analysis for very low birthweight neonates excluding the data from Patole et al. Studies: 1, Premji et al15; 2, Kamitsuka et al9; 3, Kuzma-O’Reilly et al.16 The data from the three participating centres in Kuzma-O’Reilly et al are presented separately (studies 3–5). CI, Confidence interval.
The SFR reported by Patole et al11 was developed to standardise enteral feeding during a clinical trial of erythromycin18 in preterm neonates and continued during their subsequent clinical trial of carboxymethylcellulose19 in a similar group of neonates. Apart from a sustained reduction by 52% in the time to full enteral feeds, NEC ⩾stage II was virtually eliminated (compared with six NEC related deaths a year during the previous five years) during the trial period of three years. The authors then adopted the SFR for routine use during the next two years when no trials were conducted. They state that the SFR was strictly adhered to throughout this five year period when no significant differences in the maternal/neonatal characteristics—for example, antenatal glucocorticoid therapy, intrauterine growth restriction, gestation, birth weight, need for resuscitation, PDA, neonatal exposure to indomethacin, and formula versus breast milk feeds—were observed. The first author (SKP) can confirm that no obvious changes in clinical practice (or personnel) occurred during this period. Kamitsuka et al9 developed a SFR to reduce variability in feeding practice for neonates weighing ⩾1250 g. The risk of NEC was reduced by 84% after the introduction of feeding schedules. Before the feeding schedules, those who developed NEC were more likely (73.3% v 52.1%) to have been started on formula and receive it as the first feed (83% v 20%) than those who developed NEC after implementation of the feeding schedules. The distribution of exclusive formula (22.9% v 14.8%, p<0.001) or breast milk intake (20.5% v 34.8%, p = 0.002) also differed significantly. The use of prenatal steroids increased significantly (30% v 57.1%, p<0.0001) after the feeding schedules. The number of infants with NEC, however, significantly decreased regardless of whether their mothers were pretreated with steroids. Multivariate analysis indicated that the risk of NEC increased with prenatal steroids, although this did not reach significance (p = 0.0621). These findings indicate the potential of changes in clinical practice that may influence the incidence of NEC. The SFR reported by Kuzma-O’Reilly et al16 formed part of the eight potentially better practices identified to improve nutritional support and outcomes of preterm neonates in the three participating centres. The group identified several aims including drafting and implementing written nutrition practice guidelines and decreasing/maintaining the incidence of NEC to ⩽ 50th centile of the Vermont-Oxford database. They have provided only the gestational age (26.42 (2.23) v 28.27 (2.76) weeks) and birth weight (836.46 (211.64) v 1032 (287.85) g) of the neonates for the study period (20 v 12 months). Appropriate as well as small for gestation neonates were included. Their specific aim was to evaluate, develop, and implement potentially better practices in neonatal intensive care nutrition. It is thus difficult to know whether any other seen/unseen changes in practice or perinatal/neonatal characteristics affected the nutritional outcomes including NEC. Premji et al15 developed an evidence based SFR in view of the wide variations in feeding practices. The primary outcome of interest in this matched (for gestation ±1 week and birth weight ±100 g) cohort study of 200 neonates was the time taken to establish full enteral feeds. The incidence of NEC was among the eight secondary outcomes. A total of 142 neonates were excluded for reasons such as Apgar score ⩽3 at five minutes and intrauterine growth retardation. An additional 41 neonates (18 lost, 23 not matched) did not contribute to the final analysis. Outliers and extreme values corresponding to critically ill neonates in the “real world” who were too ill to receive early feeds, which could influence the outcomes, were included in the analysis. There was no significant improvement in any of the outcomes after implementation of the CPG. Significant differences were noted between the standard practice and CPG group in the incidence of caesarean section, prolonged rupture of membranes (>24 hours), maternal glucocorticoids, and neonatal exposure to indomethacin: 85% v 74% (p = 0.02), 6% v 50% (p = 0.003), 28% v 16% (p = 0.04), 25% v 45% (p = 0.02) respectively. The incidence of NEC in neonates transferred after birth for the two groups (9 v 14) was not reported. The authors comment that “outside events or changes in clinical practice, whether observed or not, may have an impact on the outcomes in a before-after study”. They also report that factors such as fetal distress, mode of delivery, and severity of illness may have influenced the implementation of the CPG. Caution again is thus warranted in interpreting these results. Brown et al7 reported that NEC was virtually eliminated from their nursery after they implemented a cautious and conservative feeding schedule. They decided to report the feeding schedule “in the hope that others might be stimulated to properly compare its effect on the frequency of NEC”. Feeds were delayed for up to a week for neonates born after complicated deliveries with fetal distress and stopped in the presence of conditions such as severe apnoea, bradycardia, NEC, and shock in which bowel ischaemia was a possibility. Maternal/neonatal characteristics, risk factors for NEC, and any changes in other clinical/non-nutritional practices during the period of observation (3.5 v 4 years) were not reported. Spritzer et al8 introduced a cautious SFR based on the recommendations of Brown et al,7 and reported their experience after a dramatic decrease in the incidence of NEC. The decrease in NEC did not coincide with any significant changes in neonatal birth weight and gestation or in the incidence of mechanical ventilation, PDA, sepsis, and death during the period (3 v 5 years) of observation. The reports by Brown et al7 and Spritzer et al8 are from the presurfactant era when the population characteristics and clinical practices were vastly different and involved exclusive use of formula for feeding. It is possible that the changing incidence of other factors such as intrauterine growth retardation and antenatal glucocorticoid therapy or unperceived changes in practice may have affected the incidence of NEC. Although the more recent reports by Kamitsuka et al,9 Patole et al,10,11 Premji et al,15 and Kuzma-O’Reilly et al16 are all from developed nations with possibly comparable standards of neonatal care, the population characteristics and clinical practices are still expected to differ. Caution is thus necessary in interpreting our results in view of the considerable heterogeneity and a high likelihood of reporting bias. It is, however, important to appreciate that such heterogeneity may be desirable when interpreting the results in relation to a multifactorial illness such as NEC.20 We accept the fact that the quality of the evidence obtained by a meta-analysis cannot exceed the quality of the individual studies, and combining observational studies with significant heterogeneity is not expected to provide robust evidence. However, the importance of SFRs as a simple global public health tool should not be underestimated given the current lack of a single, specific preventive strategy for NEC.
The process per se of developing and implementing a SFR is associated with an increased awareness of the existing evidence and with early detection and management of NEC. The benefits of SFR may be related to the process of developing and implementing the SFR as well as to the constituents of the SFR itself. The differences in the population characteristics, clinical practices, and constituents of SFR (table 2) in the various studies, however, indicate that the benefits are most probably related to the process of developing and implementing the SFR rather than its specific constituents. Studies evaluating evidence based potentially better practices as well as CPG have reported significant improvements in neonatal outcomes after the introduction of guidelines.21,22
In summary, we conclude that SFRs may provide the single most important tool to prevent/minimise NEC while facilitating clinical research in the area. The protective effect of antenatal steroids and breast milk in the prevention of NEC must also not be forgotten.23–31 Although randomised controlled trials of SFR are justified on the basis of our results, designing and conducting such trials in the centres that have already adopted SFR will be difficult given the significant decrease in the incidence of NEC (primary outcome) that occurs after adoption of such regimens. The factors related to the dramatic reduction in the risk of NEC as reported by Patole et al also need to be explored in prospective trials. These could be related to either the patient population characteristics or their specific guidelines towards enteral feeding in the presence of “risk factors” such as haemodynamically significant PDA and/or sepsis and bile stained gastric aspirates.
REFERENCES
Footnotes
-
Competing interests: none declared