Article Text

Abstract
Objective: To determine the levels of sound to which infants are exposed during routine transport by ambulance, aircraft, and helicopter.
Design: Sound levels during 38 consecutive journeys from a regional level III neonatal intensive care unit were recorded using a calibrated data logging sound meter (Quest 2900). The meter was set to record “A” weighted slow response integrated sound levels, which emulates the response of the human ear, and “C” weighted response sound levels as a measure of total sound level exposure for all frequencies. The information was downloaded to a computer using MS HyperTerminal. The resulting data were stored, and a graphical profile was generated for each journey using SigmaPlot software.
Setting: Eight journeys involved ambulance transport on country roads, 24 involved fixed wing aircraft, and four were by helicopter.
Main outcome measures: Relations between decibel levels and events or changes in transport mode were established by correlating the time logged on the sound meter with the standard transport documentation sheet.
Results: The highest sound levels were recorded during air transport. However, mean sound levels for all modes of transport exceeded the recommended levels for neonatal intensive care. The maximum sound levels recorded were extremely high at greater than 80 dB in the “A” weighted hearing range and greater than 120 dB in the total frequency range.
Conclusions: This study raises major concerns about the excessive exposure of the sick newborn to sound during transportation.
- sound
- developmental care
- stress
- transport
- aviation medicine
Statistics from Altmetric.com
Sound levels have been monitored in neonatal intensive care units (NICUs) to develop international guidelines.1 Recommendations were made that they should not exceed 45–50 dB.2 More recently, these recommendations have been extended to optimise developmental care for premature infants.3,4 The adverse effects of excessive sound levels on preterm behaviour have been noted5,6 and appear to be most pronounced in the sickest and smallest infants.7,8 The transportation of the sick newborn or premature infant should be viewed as an extension of the NICU environment, and, although international guidelines recommend that sound levels during transport do not exceed 60 dB,9 there is a paucity of data on sound level exposure in common modes of transport.
The aim of this study was to determine the level of exposure of sick infants to sound during transportation by a specialised neonatal transport team in ambulance, helicopter, and fixed wing aircraft.
METHODS
Subjects
Consecutive neonatal transportations from a regional level III NICU in Christchurch, New Zealand from March 2000 to January 2001 were selected. These included interhospital transfer of term and premature newborn infants, transport for investigations, and return of stable infants to their referring area hospital. A detailed record of all events during the journey was kept to allow correlation with sound levels. The data recorded included the times of arrival and departure, events requiring intervention for the infant, problems en route, and the type of transport. All three transport incubators used in the study had identical specifications (Airshields TI 500 models). The fixed wing aircraft used for all flights was a Cessna Golden Eagle 421, and the helicopter was a Eurocopter BK-117.
Sound level recording device
A calibrated data logging sound meter Quest 2900 (Quest Technologies, Oconomowoc, Wisconsin, USA) with a standard 0.5 inch prepolarised condenser microphone was used to record the sound levels. The measurement range was 20–140 dB with frequency range from 10 Hz to 20 KHz. The meter was set to record “A” weighted slow response integrated sound levels (LEQ), with a 3 dB exchange rate, and maximum levels (LMax). “A” weighted slow response is the international standard for assessing sound pressure levels, which emulates the response of the human ear. It is used to assess industrial sound measurements, as they reflect sound level exposure in the hearing range. “C” weighted response sound levels were also recorded as a measure of total sound level exposure for all frequencies, including those outside the range of the human ear. Each transport study produced a time weighted average automatically analysed over one minute epochs during transport. At the end of the journey, the results were also subdivided into transport modes.
Recording device placement
The meter was placed inside the incubator secured to the bar running parallel with the length of the mattress to which the safety straps were located. This was on the non-opening side of the incubator away from the main portholes. It was wrapped in dense, vibration absorbing, sorbo-rubber material 0.4 cm thick and then in disposable thin plastic to simulate the smoothness of the incubator wall. This also protected against fluid spill and/or infection contamination and was disposable. The end of the microphone was covered by the manufacturer’s wind shield. This was retained as a safety measure to prevent injury to the infant if the sound meter became dislodged from the fixture during turbulence or sudden movement of the incubator. The placement of the microphone was approximately 10 (0.5) cm from the infant’s ear. The variation in distance was due mainly to difference in head size and positioning of the baby in the incubator. The meter was activated when the transport team left the base hospital and not touched until after the baby had been removed. Therefore at no time was the transport team distracted from caring for the infant.
Sound level analysis
The information stored by the meter was downloaded to a computer using MS HyperTerminal. The data were stored, and a graphical representative profile was generated for each journey using SigmaPlot software. The relation between decibel levels and events or changes in transport mode was established by correlating the time logged on the sound meter with the standard transport documentation sheet. Statistical analysis for the comparison of sound levels in the different transport modes was by Student’s t test or one way analysis of variance for normally distributed data.
RESULTS
Thirty eight transportations were analysed. Eight included periods of country road ambulance transport lasting more than 30 minutes. Twenty four involved fixed wing aircraft. Four were by helicopter.
Reason for transport
Twenty of the transportations involved the retrieval of sick newborn infants from regional hospitals; these infants were predominantly prematurely born. Some 15% of the transportations were transfers of sick infants between hospitals for specialist investigations or treatment, with these infants being predominantly term born. Twelve were transfers of stable premature or term infants back to level II units.
Sound levels
The maximum sound levels were recorded during air transport (table 1). The maximum levels recorded were extremely high at greater than 80 dB in the “A” weighted hearing range and greater than 120 dB in the total frequency range.
Sound levels (dB) recorded in various modes of transport
Ambulance trips
There were 38 ambulance trip recordings in the city region, and eight of these had an additional period of country road transport. The mean sound levels (LEQ median “A” weighted levels, LMax “A”, and Peak “C” levels) were all significantly higher on country roads than on city roads (table 1; p<0.01 all values) Thus, there was a significant effect of the rougher country roads.
Air transport
The sound levels in fixed wing aircraft and helicopter were both significantly higher than in an ambulance (table 1; p<0.01 all measures). There was no significant difference between the noise exposure between helicopter and fixed wing aircraft for any of the sound level measures (table 1; p>0.1 all values). Figures 1 and 2 show the changes in exposure during transport by ambulance and aircraft.

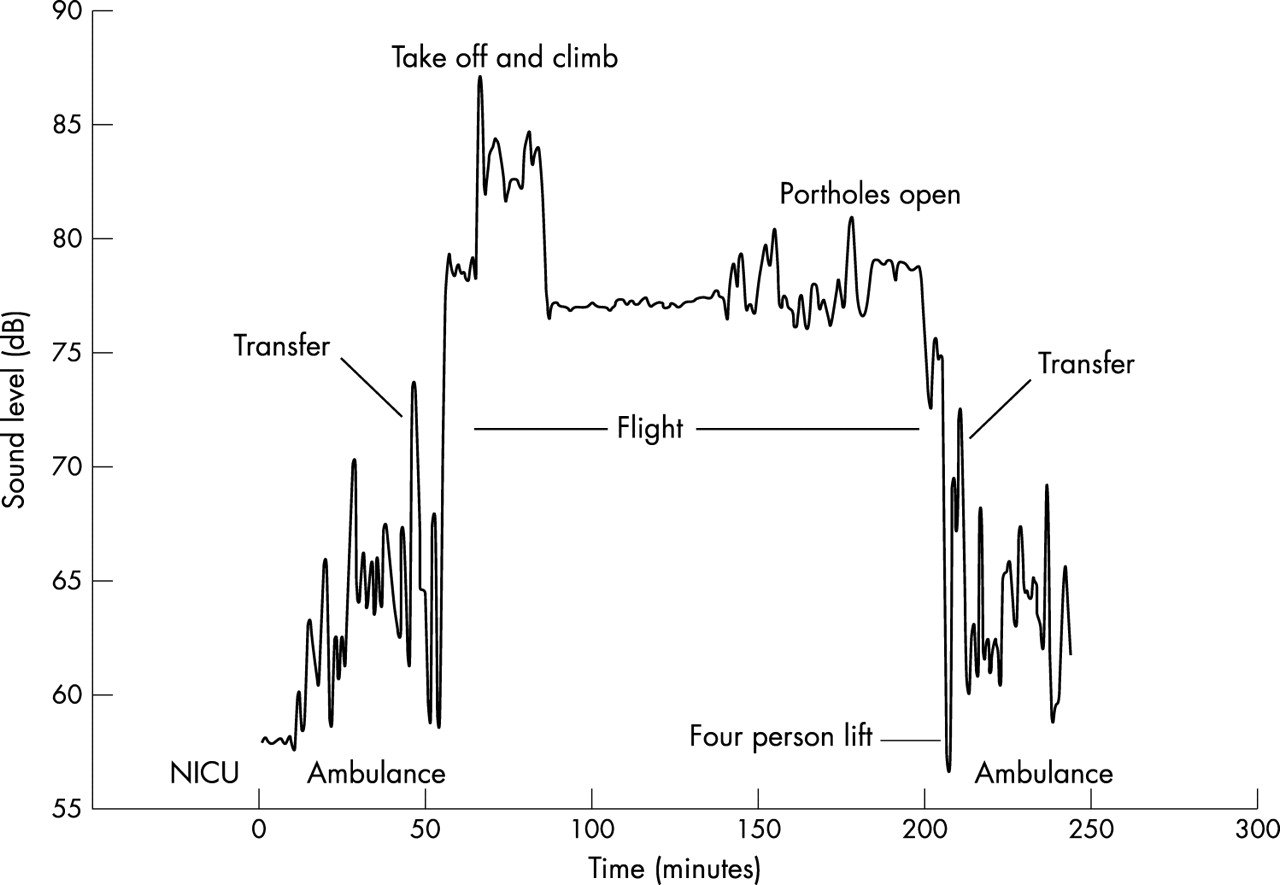
Transport of a non-ventilated infant to a specialised cardiac unit in Auckland, New Zealand from Christchurch Womens Hospital, lasting 240 minutes. Note the increased noise exposure during take off and when the portholes of the incubator were opened, and the variation in ambulance noise levels due to acceleration, speed, and road surface. Also note that all recordings are above the recommended level of 60 dB. NICU, Neonatal intensive care unit.

{kind=link}
{kind=link}
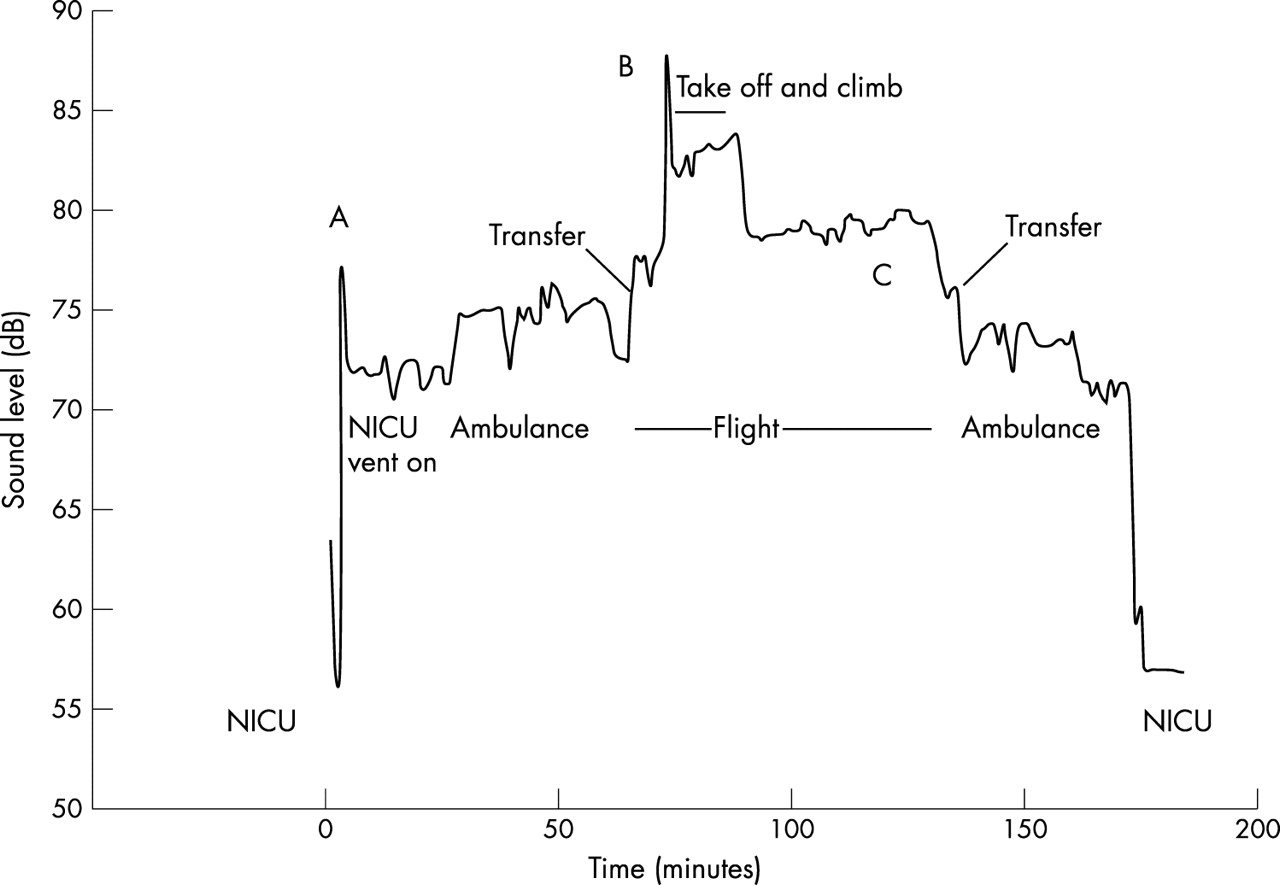
Transport of ventilated infant by ambulance and air over 180 minutes. Note: (A) the impact of the internal air compressor used to drive the ventilator, which raises sound levels above 70 dB before the start of transport; (B) the highest sound level recorded was on aircraft take off; (C) the high (close to 80 dB) continuous level of exposure for more than an hour. NICU, Neonatal intensive care unit.
It is notable that there are brief, extremely high noise levels during take off (figs 1 and 2), when the portholes of the incubator are opened (fig 1), and when the internal air compressor used for the ventilator in the transport incubator is started (fig 2).
DISCUSSION
This study clearly documents that sick and premature infants are exposed to high levels of sound during all modes of standard neonatal transportation. The highest exposure occurred with aircraft transport, but all modes exceeded current recommended levels.2,9 The higher levels of noise recorded in ambulances on country roads may be due to both the road surface and increased speed, both of which increase road noise.
There are few guidelines for acceptable sound levels during the transport of critically ill neonates.10,11 McNab9 recommended that, during paediatric and neonatal transportation, they should not exceed 60 dB, recognising that excessive and unusual sound levels may occur during transport and thus allowing a higher exposure than that recommended for the NICU. This rationale to make a higher sound level acceptable during transport of a sick vulnerable newborn infant may be flawed, as these infants may indeed be much more sensitive to these auditory stimuli than the infant in hospital. However, our study clearly shows that nearly all sound levels recorded within the human hearing range during neonatal transport significantly exceeded these more lenient guidelines.
The transport crew in a small aircraft all wear hearing protection.12 Personal commercial hearing protection for adult passenger use produces a reduction of 21–28 dB. Commercially available ear protection for neonates in neonatal units attenuates sound by only 7 dB, which is insufficient for the level of exposure found in our study.
Sound and vibration are recognised trauma encountered in aviation medicine,13 causing fatigue, increased oxygen requirement, stress, and disorientation in adults. Noise during neonatal transport is acknowledged to be a problem too, but the prime concern expressed seems to be the difficulty of communication between personnel12 to further the care of the infant, not the effect on the physiological state of the infant.14 In contrast, the effect of sound stress in the NICU is internationally acknowledged.2,15,16
Some infants may be more vulnerable than others to sound levels during transportation. Exposure to sudden noise in infants with hypoxic ischaemic encephalopathy can be associated with desaturation.17,18 In aviation physiology, episodes of hypoxic stress are additive in their effect on the compromised patient.19
This study raises major concerns about the excessive exposure of the sick newborn to noise during transportation. There is now clear recognition that we need to modify exposure of such infants to light and sound to give better immediate and long term outcomes. Such recognition has influenced modern NICU designs.16 The same principles should be applied to the critical period of transportation of the sick newborn. It would be advantageous for all organisations engaged in neonatal and paediatric transport to conduct a data logging survey to highlight sound attenuation requirements. Then sound reduction strategies for transport incubators, such as incubator covers, internal sound absorbing material, and more effective sound reducing ear protection, could be designed.