Article Text

Abstract
Aim: To describe normal values of the cerebral tissue oxygenation index (TOI) in premature infants.
Methods: TOI was measured by spatially resolved spectroscopy in preterm infants on the first 3 days of life. Infants with an abnormal cranial ultrasound were excluded. Other simultaneously measured variables were Pao2, Paco2, pH, mean arterial blood pressure, heart rate, haemoglobin, glycaemia, and peripheral oxygen saturation.
Results: Fifteen patients with a median postmenstrual age of 28 weeks were measured. There was a significant increase in median TOI over the first 3 days of life: 57% on day 1, 66.1% on day 2, and 76.1% on day 3. Multiple regression analysis showed no correlation between TOI and postmenstrual age, peripheral oxygen saturation, mean arterial blood pressure, Pao2, Paco2, and haemoglobin concentration.
Conclusion: Cerebral TOI increases significantly in the first 3 days of life in premature babies. This increase probably reflects the increase in cerebral blood flow at this time.
- near infrared spectroscopy
- brain oxygenation
- tissue oxygenation index
- NIRS, near infrared spectroscopy
- TOI, tissue oxygenation index
Statistics from Altmetric.com
Spatially resolved spectroscopy is a new method, using near infrared spectroscopy (NIRS), for measuring cerebral haemoglobin oxygen saturation. The tissue oxygenation index (TOI) is measured with a light detector with three sensors placed at different distances from the near infrared light source. If light with a given intensity is sent into tissue, it is attenuated because of “scatter” loss and “absorption” loss. If the distance between the light source and the sensor is large enough, the isotropy of scatter distribution becomes so homogeneous that the scatter loss is the same at the three sensors. Therefore any differences in intensity measured at the three different sensors can be interpreted as differences in absorption loss. Thus the local absorption change can be seen as a function of the distance between the light source and the three sensors. With this information, an oxygenation index can be calculated using a previously reported algorithm.1,2
Several research groups have measured TOI in healthy adults with different NIRS instruments,3–,7 and no differences in TOI values between the right and left forehead have been found. To our knowledge, no normal cerebral TOI values in the first days of life have been reported for premature babies (less than 30 weeks gestation). In this study, we measured TOI on days 1, 2, and 3 to obtain “normal” values and to investigate changes with postnatal age.
PATIENTS AND METHODS
Fifteen patients with a postmenstrual age of less than 31 weeks were included. The median postmenstrual age was 28 weeks (range 25–30). A brain ultrasound was performed on all patients before measurements were started. Exclusion criteria were an abnormal brain ultrasound before the TOI measurement and severe pulmonary hypertension as evidenced by echocardiography and/or congenital malformations.
An NIRO 300 (Hamamatsu Phototonics K.K., Tokyo, Japan) was used for spatially resolved spectroscopy. The optode was placed at the right frontoparietal side with the sensors at 4 cm distance. All patients were measured within 6 hours of birth for at least 30 minutes. The second and third measurements were performed 24 and 48 hours later. The specific variable measured was TOI.
The simultaneously studied electrocardiogram, pulse rate and peripheral oxygen saturation (beat to beat, on a Nelcor-2000 monitor), and mean arterial blood pressure (Siemens, Sirecus) were recorded in an analogous way with a sampling frequency of 100 Hz by the data acquisition system Codas (Dataq Instruments, Akron, Ohio, USA) and stored in a PC. The NIRO-300 signals are digital and recorded with a sampling rate of 6 Hz. They are converted into analogue signals with a sample and hold function before their introduction into the Codas system. Paco2, Pao2, pH, glycaemia, haemoglobin, and percentage of fetal haemoglobin were measured in an arterial blood sample on a blood gas analyser (Radiometer, Copenhagen, Denmark) before and after the measurement. The same author (GN) performed all the measurements.
The median and 95% confidence interval (CI) was calculated for the TOI values if the peripheral oxygen saturation did not change more than 5%. The median and 95% CI of heart rate, peripheral oxygen saturation, mean arterial blood pressure, Pao2, Paco2, haemoglobin, percentage of fetal haemoglobin, and glycaemia over this period were also calculated. A Kolmogorov-Smirnov test was used to test for a normal distribution of the TOI for the whole group and the three subgroups (different days). The median and 95% CI of the standard deviation on each TOI measurement was calculated to show the variability in this parameter.
Analysis of variance was applied to see if there was a significant difference between TOI and postnatal age. The Student-Newman-Keuls test was used for all pairwise comparisons. p<0.05 was considered significant. Multiple regression analysis was used to detect significant effects of the other variables on TOI.
RESULTS
Fifteen patients were studied during the first 3 days of life. The mean (SD) birth weight was 1053 (395) g, and the mean (SD) head circumference was 24.8 (2.5) cm. All patients had a normal ultrasound of the brain before measurement on day 1. Further follow up of the ultrasound on days 3, 5, and 7 showed an intraventricular haemorrhage grade I or II in seven of the 15 patients. However, no posthaemorrhagic hydrocephalus or intraventricular haemorrhage grade III or IV was noted. One patient developed cystic periventricular leucomalacia three weeks later. Seven patients developed retinopathy of prematurity grade III, and three of these patients needed cryotherapy. Psychomotor follow up was normal in 10 patients at the age of 6 months.
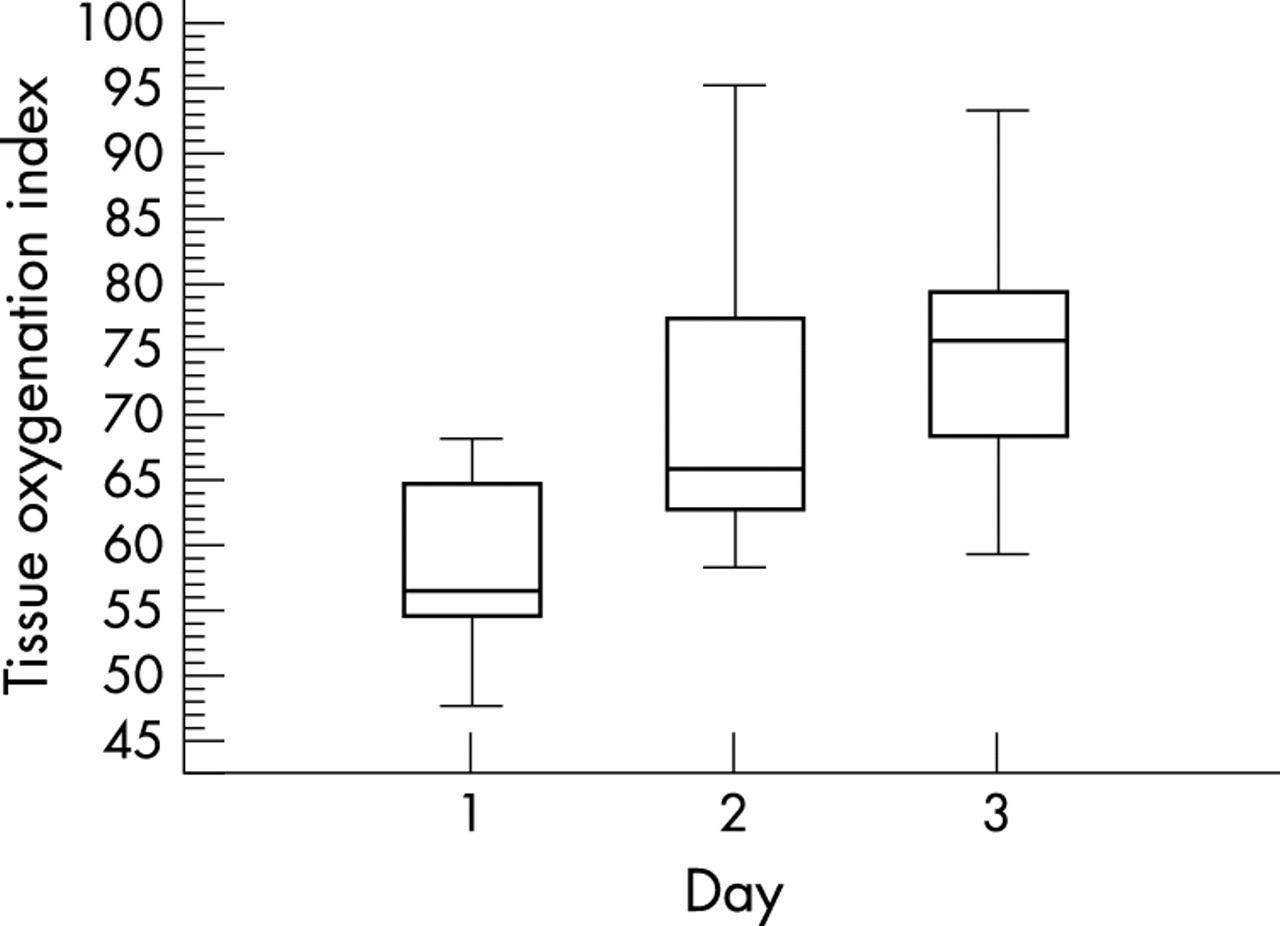
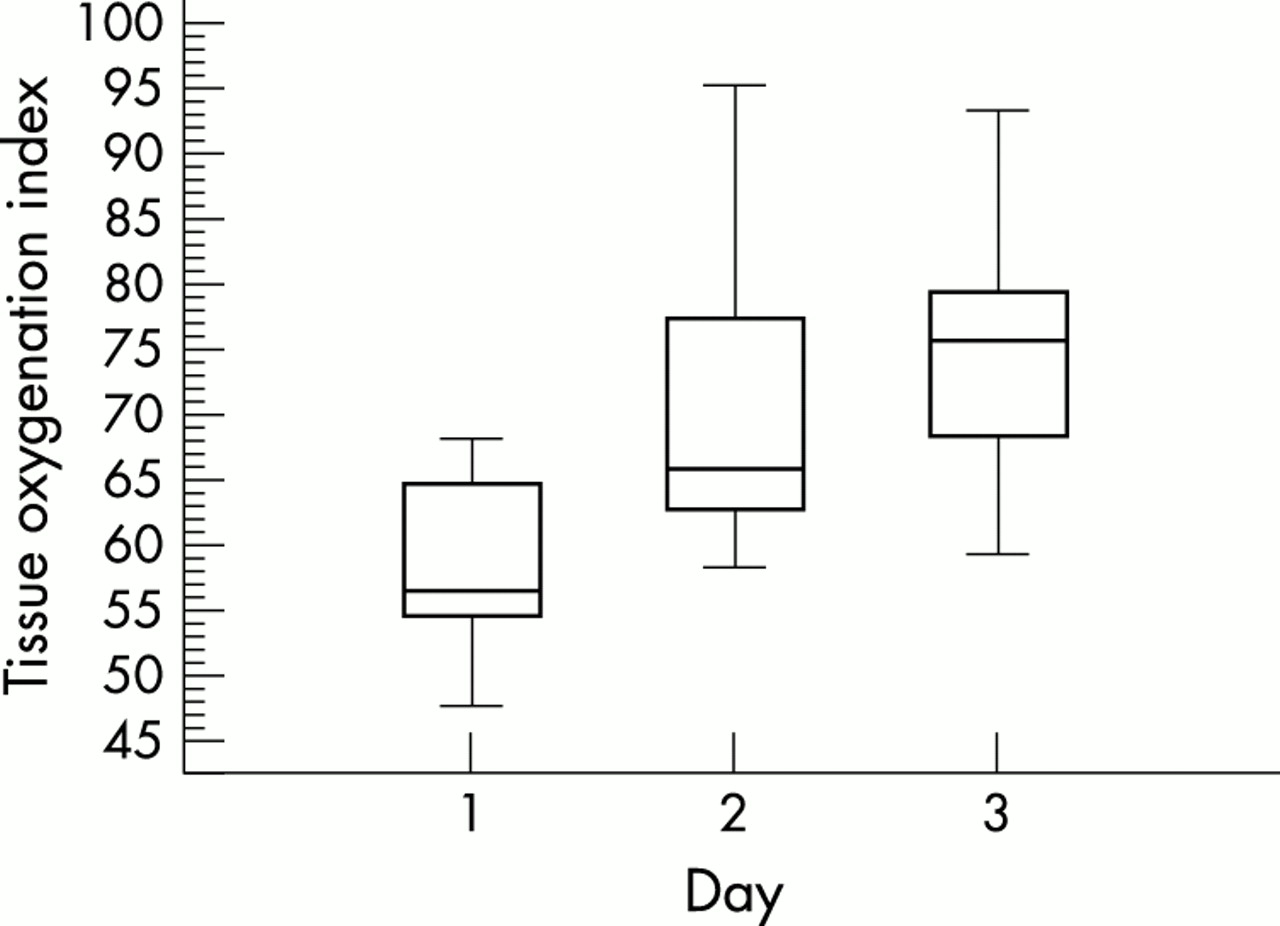
Figure 1⇓ shows the TOI values. The median TOI was 57% (95% CI 54 to 65.7%) on day 1, 66.1% (95% CI 61.982.2%) on day 2, and 76.1% (95% CI 67.8 to 80.1%) on day 3. The mean standard deviation of the TOI values was 2.2% (95% CI 2.4%). There was a normal distribution for the whole group as well as for the three different subgroups (Kolmogorov-Smirnov test for normal distribution, p>0.2). Analysis of variance showed a significant difference (p<0.001) between TOI and postnatal age. A Student-Newman-Keuls test for all pairwise comparisons showed that there was a significant increase in TOI from day 1 to day 2 and from day 1 to day 3, but not from day 2 to day 3.
{kind=link}
Box and whisker plot showing the median and interquartile range for the tissue oxygenation index (%) measured on days 1, 2, and 3. The increase from day 1 to day 2 and from day 1 to day 3 was significant (p<0.05).
Table 1⇓ shows the different variables. To test the effect of oxygenation, analysis of variance was performed to find an eventual difference in peripheral oxygen saturation for the different days. No significant difference was found (p = 0.44). A significant (p = 0.003) increase in blood pressure from day 1 to day 3 was found. The increase in blood pressure from day 1 to day 2 was not significant. There was also a significant difference in Paco2 on the different days. Mean Paco2 on day 1 was 31 mm Hg, on day 2 45 mm Hg, and on day 3 36.5 mm Hg. This is a significant difference (p < 0.001) between the three days, but there was an increase from day 1 to 2 and a decrease from day 2 to 3. There was no significant difference in Pao2, bicarbonate, and pH on the different days. Haemoglobin concentration was 14.1 g/dl on day 1, 13 g/dl on day 2, and 14.1 g/dl on day 3. The percentage of fetal haemoglobin was only measured in eight patients. It was 86.7% on day 1, 88.5% on day 2, and 69.7% on day 3. This significant decrease on day 3 is explained partly by the fact that these patients had received a blood transfusion.
Median and 95% confidence interval for tissue oxygenation index, THI, mean arterial blood pressure, peripheral oxygen saturation, Pao2, Paco2, haemoglobin, and fetal haemoglobin on days 1,2, and 3.
Multiple regression analysis showed an increase in TOI only from day 1 to day 3 (p < 0.05). No correlation between TOI and blood pressure, Paco2, peripheral oxygen saturation, haemoglobin concentration, fetal haemoglobin, glycaemia or postmenstrual age was found with multiple regression analysis. No correlation was found between TOI or the standard deviation of TOI and head circumference.
No relation was found between TOI and intraventricular bleeding, periventricular leucomalacia, retinopathy, or abnormal psychomotor follow up.
DISCUSSION
NIRS is a non-invasive method for measuring oxygenated and deoxygenated haemoglobin and derived values of brain oxygenation, cerebral blood flow, and cerebral blood volume. Until now, it has been used only in research because it is very sensitive to movement artefacts. Furthermore, it does not provide absolute values, only values relative to the starting point in a continuous way. TOI, in contrast, is an absolute value and can be measured on different occasions in the same patient. Although in this study TOI was determined in very premature babies and their head circumference was small, very stable TOI values with a mean standard deviation of 2.2% were obtained from measurements taken over at least 30 minutes.
Whether TOI mainly reflects cerebral venous saturation is still under discussion. Several studies report TOI values obtained in healthy adult volunteers.3–,7 Quaresima et al3 compared TOI with cerebral venous oxygen saturation, measured by NIRS (NIRO 300, Hamamatsu), and concluded that TOI mainly reflected saturation of the intracranial venous compartment. Two studies using different NIRS instruments also found a correlation, but between TOI and jugular bulb oximetry.8,9 Other studies comparing jugular bulb oximetry with TOI did not find any correlation.10–,14 Al-Rawi et al15 measured TOI in 60 patients undergoing endarterectomy. They found a significant correlation between TOI and flow velocity, measured by transcranial Doppler of the ipsilateral middle cerebral artery. The change in TOI was predominantly associated with internal carotid artery clamping, and a change during external carotid artery clamping was only seen if there was also a change in blood pressure. The sensitivity of TOI to intracranial and extracranial changes, when there were no blood pressure changes or an extracranial to intracranial anastomosis, was 87.5% and 0% respectively and the specificity was 100% and 0% respectively. They conclude that TOI predominantly measures intracranial changes. Another important finding was that a decrease in TOI is much more important than the absolute value. Different patients had different absolute values, but they all showed a large decrease when the internal carotid artery was clamped (mean (SD) difference in TOI = −9.4 (7.1)%).
In adults, normal TOI values have been reported to range from 65% to 85%.3–,7 Teller et al16 reported TOI values for the liver and brain during feeding in 25 infants, aged 1–54 days (mean 15.2) with a postmenstrual age of 29–40 weeks (mean 34 weeks and 1 day) and a weight of 1400–3365 g (mean 2385). Mean (SD) TOI of the brain was 62.1 (9.7)%, which is lower than the values reported in adults. They are comparable to our results on day 1 (59.2 (6.4)%), although TOI values on days 2 and 3 were higher and more compatible with the results in adult volunteers. Dani et al17 described mean cerebral oxygen saturation during caffeine (group A) and aminophylline (group B) treatment in 40 infants with a mean (SD) gestational age of 30.4 (3) weeks in group A and 29.4 (1.4) weeks in group B. The postnatal age was 19 (13) days in group A and 22 (13) days in group B. The mean cerebral oxygen saturation before and after treatment ranged from 68.5 (9.1)% to 70.1 (6.6)% in group A and from 64.6 (13)% to 68.1 (15)% in group B. These results are comparable to our results on days 2 and 3.
There are different plausible explanations for the increase in TOI found in this study during the first 3 days of life. An increase in oxygenation was ruled out by including only the results obtained while peripheral oxygen saturation remained stable. Also arterial oxygen content did not change significantly on the different days. Haemoglobin content decreased from day 1 to day 3, but no significant correlation was found with TOI. Fetal haemoglobin content decreased significantly, but again no correlation was found with TOI. Further studies are indicated, as fetal haemoglobin was measured in only eight patients.
One explanation for the increase in TOI is an increase in cerebral blood flow, as has been found previously.6,18 Meek et al19 described a significant increase in cerebral blood flow during the first 72 hours in premature infants, independent of mean arterial blood pressure, Paco2 and packed cell volume. An important bias in our study is the low Paco2 values on the first day. This could partly explain the lower cerebral blood flow and hence the lower TOI values, although we found no correlation between Paco2 and TOI. In adults no correlation was found between TOI and Paco2.12,14 A decrease in cerebral blood flow during hypocapnia is well described in neonates.20 The combination of low Paco2 with low blood pressure may explain a lower cerebral blood flow and hence a greater oxygen uptake with a lower venous saturation. Measurements of the venous oxyhaemoglobin saturation confirm this hypothesis. Venous oxyhaemoglobin saturation can be measured by NIRS with partial jugular venous occlusion. Yoxall et al21 validated this technique with co-oximetry of jugular bulb blood obtained during cardiac catheterisation in infants and young children. When cerebral blood flow and cerebral venous oxyhaemoglobin saturation are measured, cerebral oxygen consumption can be calculated. An increase in cerebral oxygen consumption was found with advancing gestational age.22 Wardle et al23 found an increase in the fractional oxygen extraction with a decrease in Pco2 and an increase during blood transfusion. This may explain the lower TOI in our patients on the first day when there was a significantly lower Paco2.
We found no relation between TOI and neurological complications or retinopathy, but the measurements were limited to half an hour a day. The neurological and ophthalmic complications may be related to hypocapnia on the first day. In preterm babies, a statistical correlation has been found in different studies between hypocapnia and brain damage and later developmental deficit.20
Yoxall et al21 suggest that measurement of cerebral oxygenation gives more information than measurement of cerebral blood flow for the prevention of cerebral hypoxia and ischaemia. Measurements of venous oxyhaemoglobin saturation, cerebral oxygen consumption, and cerebral fractional oxygen extraction can be performed with NIRS.21–,23 However, measurement of cerebral venous oxyhaemoglobin saturation is still difficult and cannot be performed continuously. TOI is a non-invasive parameter for measurement of cerebral oxygenation and may be useful for continuous monitoring of venous oxyhaemoglobin saturation. Although several validation studies have been carried out in adults, further studies in animals need to be performed to study the relation between TOI, venous jugular saturation, and cerebral blood flow. In neonates, further studies are needed to determine the relation between TOI and venous oxyhaemoglobin saturation as measured by partial jugular venous occlusion. Further clinical studies should attempt to elucidate the variation in TOI over several days. These longer lasting measurements may be able to detect the relation between periods of low cerebral oxygenation and neurological complications such as periventricular leucomalacia. As the measurement of TOI is less sensitive to movement artefacts, these studies may result in a new way to detect and prevent severe cerebral ischaemia by continuous monitoring of cerebral oxygenation.
In conclusion, measurement of TOI in premature infants is a new non-invasive method for measuring aspects of cerebral brain oxygenation. An increase in TOI over the first 3 days of life was found in 15 premature babies. This increase in TOI may reflect an increase in cerebral blood flow during this time.
Rapid responses
Letters on the following Archives of Disease in Childhood Fetal and Neonatal Edition papers have been published recently as rapid responses on the ADC website. To read these letters visit www.archdischild.com and click on “Read eLetters”
Posthaemorrhagic ventricular dilatation in the premature infant: natural history and predictors of outcome. B P Murphy, T E Inder, V Rooks, et al. OpenUrlAbstract/FREE Full Text
Neonatal shaken baby syndrome: an aetiological view from Down under. A N Williams, R Sunderland. OpenUrlFREE Full Text
If you would like to post an electronic response to these or any other articles published in the journal, please go to the website, access the article in which you are interested, and click on “eLetters: Submit a response to this article” in the box in the top right hand corner.
Acknowledgments
This research was sponsored by the Belgian Programme IVAP V-10-29, the Flemish GOA project MEFISTO-666, and the KV Leven project IDO/99/03.