Article Text

Abstract
Objective: To determine the incidence of spontaneous closure of the patent ductus arteriosus (PDA) and the use of medical therapies for treatment of PDA-related conditions among very low birth weight (VLBW) infants with ductal patency at the time of initial hospital discharge.
Study design: We conducted a single-centre, retrospective, observational study of VLBW infants (birth weight <1500 g) born during 2004 and 2005 and discharged with a PDA. PDA was defined by echocardiographic and/or clinical criteria. We identified the related discharge needs, subsequent interventions, and the post-menstrual age (PMA) at which there was no longer evidence of a PDA.
Results: Three hundred and ninety one VLBW infants were admitted; 310 survived to discharge. Ninety five were diagnosed with a PDA during their hospitalisations; 21 had a PDA at discharge (10 received indomethacin, 11 were never treated). Among these, mean gestational age was 28 weeks, mean birth weight was 998 g, and median duration of hospitalisation was 73 days. Two infants were discharged on oxygen, two on diuretics, and two on both. None had congestive heart failure, and none died during infancy. Spontaneous closure occurred in 18 of 21 infants at a median PMA of 48 weeks (range 34–76; interquartile range 46–56). Two infants had coil occlusion at 11 months of age. One patient had a PDA at 14 months of age.
Conclusions: Among a select group of VLBW infants with a PDA at initial hospital discharge, spontaneous closure during early infancy occurred in most infants.
Statistics from Altmetric.com
The diagnosis of patent ductus arteriosus (PDA) is common among very low birth weight (VLBW) infants, with approximately 40% to 60% of VLBW infants assigned this diagnosis some time during the first few weeks of life.1 Despite this common occurrence, opinion about the use of interventions to promote closure of a PDA is controversial.2 Because of the lack of evidence of benefit from treatments for closure, and recent data that suggest that both medical3 and surgical4 treatments for the PDA are associated with poor outcomes, an increasing number of clinicians, including some in our institution, rarely treat PDAs.5 The result of this pattern of practice is the persistence of ductal patency at the time of discharge in some infants. Unfortunately, little is known about the outcome of these infants. Information about the probability of closure after discharge and problems associated with persistent patency would help inform physicians considering early treatment.
The objective of this study was to examine the outcome of VLBW infants with PDAs at the time of discharge from their initial hospitalisation. We identified rates and times of spontaneous closure, the use of adjunctive therapies for problems related to ductal shunting (eg, diuretics, digoxin), and procedures for permanent closure (eg, cardiac catheterisation) during the 18 months following discharge.
METHODS
We performed a retrospective, observational cohort study of VLBW infants discharged with a PDA. To identify our cohort, we examined the outcome of all VLBW infants receiving care during 2004 or 2005 in the North Carolina Children’s Hospital. Medical records, echocardiograms, and pharmacy logs of infants diagnosed with a PDA at any time were reviewed, and the medical and surgical interventions used to aid in closure from birth to the time of discharge were recorded.
The Vermont Oxford Network definition of PDA6 was used which includes: (1) clinical evidence of a left to right PDA shunt documented by continuous murmur, hyperdynamic precordium, bounding pulses, wide pulse pressure, congestive heart failure, increased pulmonary vasculature or cardiomegaly by chest x ray, and/or increased oxygen requirement or; (2) echocardiographic evidence of a PDA with documentation of left to right flow through the ductus. In infants with a PDA, closure was presumed if clinical evidence of shunting resolved and a murmur was no longer present. A repeat echocardiogram was performed in infants with persistent murmurs, and ductal patency at discharge was confirmed by echocardiography in all infants assigned the diagnosis of PDA at that time.
Among infants with PDAs at discharge, we identified the related discharge needs (eg, oxygen, diuretics). For the 18 months after discharge or until closure of the PDA, we reviewed echocardiograms and follow-up clinic notes from the paediatrician and/or paediatric pulmonologist, and paediatric cardiologist for the presence and size of the PDA as well as signs or symptoms of PDA-related morbidities (eg, congestive heart failure), medical therapy of PDA-related morbidities (eg, diuretics, digoxin), and subsequent interventions for closure. Closure after discharge was defined as either absence of any signs or symptoms of ductal shunting or echocardiographic evidence of closure.
RESULTS
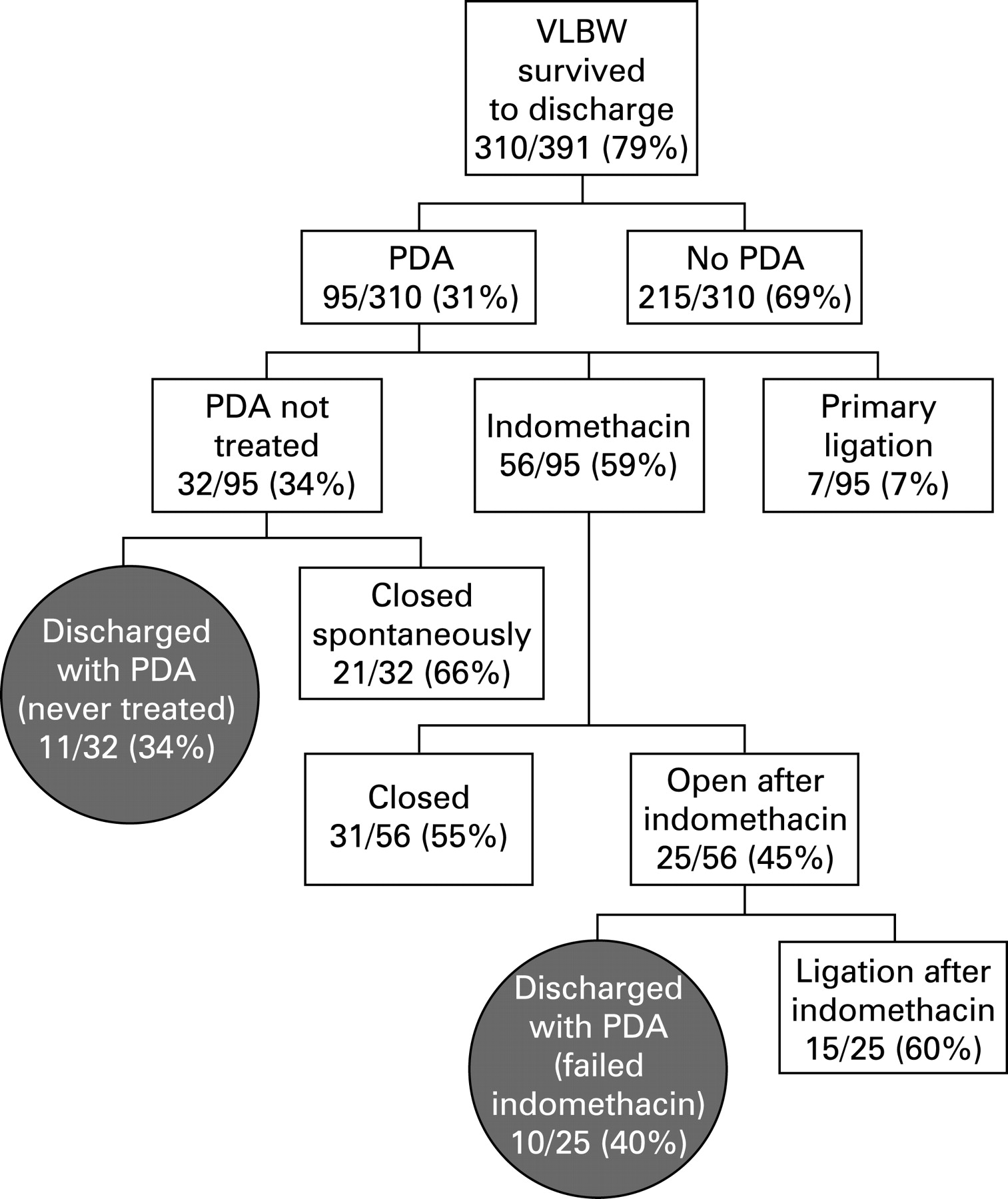
Three hundred and ten VLBW infants survived to discharge; 95/310 were diagnosed with a PDA at some time during their hospitalisation (fig 1). Among these infants, 63 (of 95) were treated either surgically or medically. The DA remained patent in 10 of these infants. An additional 32 infants with PDAs received no treatment for closure. The DA remained patent at discharge in 11 of these infants. Therefore, a total of 21 infants (10/95 who received treatment and 11/32 who received no treatment) had a PDA at the time of discharge.

{kind=link}
Among these 21 infants, mean gestational age was 28 weeks, mean birth weight was 998 g, and median duration of hospitalisation was 73 days (interquartile range; IQR 48–99). Two of these infants were discharged on oxygen, 2 on diuretics, and 2 on both. None were diagnosed with a PDA-related morbidity (eg, pulmonary hypertension, congestive heart failure, or bacterial endocarditis); none received medical therapy for a PDA-related morbidity (eg, digoxin); and none died before 18 months. Eighteen of the 21 PDAs present at discharge closed spontaneously (10 confirmed by echocardiography, 8 confirmed by clinical exam). Closure was confirmed at exams conducted at a median post-menstrual age of 49 weeks (range 34–76; IQR 46–56) (table 1). Two infants underwent percutaneous transarterial coil occlusion, at 12 and 14 months of age. One patient had a PDA at a corrected age of 14 months (18 months chronological age). No infants were lost to follow-up.
DISCUSSION
Little is known about the natural history of the DA in extremely premature infants because of the widespread acceptance of treatments to promote closure of a PDA as a standard of care.7 Recently, a few studies have added to our understanding by reporting rates of closure when treatment for a PDA has been delayed because of a clinical trial design or physician preference.8–10 We add to this growing body of literature by describing rates of spontaneous closure, and related outcomes, among VLBW infants with persistent patency of the DA at the time of initial hospital discharge. In this small cohort of infants with PDAs at the time of initial hospital discharge from our institution, spontaneous closure was common, occurring in the majority of infants, and usually occurring within several months of discharge. Morbidities attributable to persistent ductal shunting were not observed. No therapies to manage congestive heart failure were necessary. Only 4 of 21 infants were receiving diuretics at the time of discharge, presumably as a treatment for chronic lung disease. Two of 21 infants underwent uneventful closure of the DA by intra-arterial occlusion during catheterisation.
Despite these apparently good outcomes, our results should be interpreted with caution. All study infants had either small-or moderate-sized PDAs, presumably resulting in relatively small aorto-pulmonary shunts. The absence of large PDAs may be a result of the manner in which PDAs are treated in our institution where approximately two-thirds of infants with PDAs receive treatment for closure. In institutions where little or no treatment is provided, the incidence of large PDAs at discharge might be higher.10 We do not know whether infants with large PDAs and shunts would have experienced the same rate of favourable outcomes as was observed in our cohort. Further, we did not evaluate growth or neurodevelopment, outcomes that may have been impacted by persistent shunts. However, because spontaneous closure occurred relatively soon after discharge, major impairment of growth and development seems unlikely. Another possible consequence of persistent aorto-pulmonary shunting would be abnormal growth of the pulmonary vasculature.11 Pulmonary hypertension and cor pulmonale are adverse sequelae of longstanding right to left intracardiac shunting.12 Although not evaluated in our study, there was no suggestion that similar problems were present in this cohort based on examinations by cardiologists. However, long-term follow-up would be necessary to evaluate this outcome.
We found that spontaneous closure of PDAs among VLBW infants with persistent patency of the DA at the time of initial hospital discharge is common, and persistent patency during early infancy was not associated with significant morbidity. This observation suggests that withholding treatments to promote ductal closure during the latter period of hospitalisation may be a reasonable alternative to medical and surgical treatment of small to moderate PDAs in VLBW infants. However, close follow-up of these infants following hospital discharge must be insured because of the potential adverse effects of longstanding aorto-pulmonary shunts.
Footnotes
Funding: Funded in part by a research grant received as part of a Professional Development Award by Pediatrix Medical Group.
Competing interests: None.
Ethics approval: This study was approved by the Biomedical Institutional Review Board of the University of North Carolina at Chapel Hill.