Article Text

Abstract
Objective: To investigate the effects of umbilical cord milking on the need for red blood cell (RBC) transfusion and morbidity in very preterm infants.
Patients and Methods: 40 singleton infants born between 24 and 28 weeks’ gestation were randomly assigned to receive umbilical cord clamped either immediately (control group, n = 20) or after umbilical cord milking (milked group, n = 20). Primary outcome measures were the probability of not needing transfusion, determined by Kaplan–Meier analysis, and the total number of RBC transfusions. Secondary outcome variables were haemoglobin value and blood pressure at admission.
Results: There were no significant differences in gestational age and birth weight between the two groups. The milked group was more likely not to have needed red cell transfusion (p = 0.02) and had a decreased number (mean (SD)) of RBC transfusions (milked group 1.7 (3.0) vs controls 4.0 (4.2); p = 0.02). The initial mean (SD) haemoglobin value was higher in the milked group (165 (14) g/l) than in the controls (141 (16) g/l); p<0.01). Mean (SD) blood pressure at admission was significantly higher in the milked group (34 (9) mm Hg) than in the controls 28 (8) mm Hg; p = 0.03). There was no significant difference in mortality between the groups. The milked group had a shorter duration of ventilation or supplemental oxygen than the control group.
Conclusion: Milking the umbilical cord is a safe procedure, reducing the need for RBC transfusions, and the need for circulatory and respiratory support in very preterm infants.
Statistics from Altmetric.com
Recent advances in perinatal and neonatal medicine have improved the survival of even extremely low birth weight (ELBW) infants.1 ,2 However anaemia of prematurity with the subsequent need for red blood cell (RBC) transfusion is still a common problem in very low birth weight (VLBW) infants. The current Cochrane review by Aher et al showed that early or late administration of recombinant human erythropoietin (rHu-EPO) reduced the RBC transfusions in VLBW.3 ,4 However, they concluded that early administration of rHu-EPO is not recommended because the small reductions of RBC transfusion were of limited clinical importance and there was a significant increase in the risk of stage ⩾3 retinopathy of prematurity.5 ELBW infants still have the greatest risk for needing RBC transfusions within the first 3 weeks of life, owing to combined therapy of rHu-EPO, iron, folate and vitamin B12.6
Our previous study found that the initial haemoglobin value was one of the important factors affecting the need for RBC transfusions in ELBW infants who are treated with erythropoietin and an iron supplement.7 In 1993, Kinmond et al showed that delayed umbilical cord clamping increased the initial haematocrit and decreased the need for RBC transfusions compared with no intervention in infants born between 27 and 33 weeks’ gestation.8 However, a delay in cord clamping of 30–45 seconds, which can often interfere with resuscitation, was often not possible in ELBW infants.9 We proposed the hypothesis that umbilical cord milking as an alternative to delayed cord clamping might increase the circulatory blood volume expressed as the haemoglobin value and reduce the number of infants requiring a RBC transfusion as compared with control conditions. Increase in circulatory volume, however, might lead to increased blood pressure. Thus, the purpose of this randomised controlled clinical trial was to investigate the impact of umbilical cord milking on the transfusion requirements and morbidity in very preterm infants.
MATERIALS AND METHODS
The study design was a randomised controlled trial with two treatment arms.
Sixty-three fetuses were assessed for eligibility; 23 fetuses were excluded. Thus, 40 of 63 VLBW infants born between 24 to 28 weeks’ gestation were randomised and were admitted to the level III neonatal intensive care unit at Nihon University Itabashi Hospital, Tokyo, Japan.
This study was carried out in a single tertiary perinatal centre over a 24-month period between January 2001 and December 2002. Exclusion criteria were (a) multiple births; (b) major congenital anomalies or chromosomal anomalies; and (c) hydrops fetalis. Women were admitted to the hospital at least 6 hours before delivery to allow time for enrolment. The chief neonatologist decided to enrol the patients in the present study. For randomisation, we used serially numbered opaque envelopes that were opened by neonatology staff after enrolment and just before delivery. Patients were randomised to having their umbilical cord clamped either immediately or after umbilical cord milking. A neonatologist informed obstetricians of the intervention type. Thus the resuscitation team and therapeutic team were aware of the infants’ grouping. Infants in the milked group were placed at or below the level of the placenta, and about 20 cm of the umbilical cord was vigorously milked towards the umbilicus two to three times before clamping the cord. The milking speed was about 20 cm per 2 seconds.
Prenatal and delivery data were collected from the mother’s charts. Infant data were collected from records.
Informed consent was obtained from the parents after full explanation of the procedure. This study was approved by the hospital investigation committee.
The primary outcome measures were the probability of not needing a transfusion and the number of RBC transfusions during the hospital stay. The secondary outcome variables were haemoglobin value and blood pressure at admission.
The following variables were measured: initial haemoglobin values, age of starting rHu-Epo treatment, haemoglobin value at the start of rHu-EPO treatment, age in days at the time of the first transfusion, number of transfusions, total phlebotomy loss during the first 4 weeks, systolic, diastolic and mean blood pressure, peak serum bilirubin, duration of phototherapy, nutritional conditions, polycythaemia, respiratory distress syndrome (RDS), patent ductus arteriosus (PDA), intraventricular haemorrhage (IVH), hyperkalaemia, periventricular leucomalacia (PVL), chronic lung disease (CLD), retinopathy of prematurity (ROP) and duration of mechanical ventilation and oxygen supplementation.
A peripheral or umbilical arterial catheter was placed to obtain arterial pressure readings and blood samples. If it was difficult to place a peripheral artery catheter because of the very fragile skin in infants born under 25 weeks’ gestation, an umbilical arterial catheter was placed instead. Systolic, diastolic and mean blood pressure were monitored continuously using an arterial catheter and a multichannel neonatal monitor (Siemens patient monitor SC7000; Siemens-Asahi Medical Technologies Ltd, Japan).
Whole blood counts were measured by a Coulter LH755 (Beckman Coulter Inc, USA). The daily total blood loss in each infant was recorded in the first 28 days of life.
Polycythaemia was defined as a haemoglobin value ⩾220 g/l at any time. RDS was defined on the basis of the clinical and radiographic findings and a negative or weak microbubble test.10 The diagnosis of PDA was determined from the clinical symptoms and the presence of PDA flow on colour Doppler echocardiography. Significant PDA was defined as deterioration in the respiratory condition, decrease in urine output (<1 ml/kg/h) or feeding intolerance. IVH was diagnosed by serial cranial ultrasound and was graded from I to IV according to Papile’s classification.11 Attending neonatologists performed cardiac and cranial ultrasonographic studies. Hyperkalaemia was defined as a serum potassium level ⩾6.5 mmol/l. The diagnosis of PVL was made if cyst development was seen on serial cranial ultrasound or if magnetic resonance imaging showed several abnormalities, including cystic lesions, enlarged ventricles, delayed myelination, high-intensity areas in the white matter and cortical atrophy.12 CLD was defined as the need for supplemental oxygen at 4 weeks of age or at 36 corrected weeks and the presence of positive radiographic findings. The diagnosis of ROP was based on the International Classification.13
If the haemoglobin concentration dropped below 120 g/l, infants received 200 IU/kg of rHu-EPO (Epoetin alfa; Kirin Brewery Co, Ltd, Tokyo, Japan) twice a week. If oral feeding was tolerated, an oral iron supplement at a daily dose of 4 mg/kg of body weight was recommended when starting rHu-EPO treatment; the dosage of iron was adjusted based on the serum iron (⩽9 μmol/l) or ferritin (⩽100 μg/l) concentration, and the iron dose was increased to 6 mg/kg/day. Parenteral iron was not used owing to the increased risk of oxidative stress in these preterm infants.
Breast milk was strongly recommended during the first 4 weeks. Intravenous hyperalimentation started at 7 days of life without intravenous iron supplementation. If the total amount of oral feeding exceeded 80 ml/kg, intravenous hyperalimentation ceased.
Table 1 presents the guidelines for RBC transfusions. All transfusions consisted of 10 ml/kg packed red cells of haematocrit 0.60 stored in mannitol adenine phosphate (Red Cells M·A·P Nisseki; Japanese Red Cross Society, Tokyo, Japan).
STATISTICAL
On the basis of the results of the previous meta-analysis of early versus delayed umbilical cord clamping, which had shown that the relative risk of transfusions for anaemia in the early clamping group was 2.01 (95% CI 1.24 to 3.27),5 a sample size calculation determined that 17 babies in each group would be needed to show a 45% difference between the two groups, with a two-sided α of 0.05 and 80% power.
Kaplan–Meier analysis and the log-rank test were used to evaluate the transfusion free time. In patients who did not need transfusion, the time from birth to hospital discharge was used. Normally distributed continuous outcome variables were compared with the unpaired Student t test, and non-parametric continuous outcome variables were analysed with the Mann–Whitney U test. Categorical variables were compared with the χ2 test. The Fisher exact test was used for contingency tables showing expected cell counts <5. Data are expressed as mean (SD). All analyses were conducted with two-tailed tests. p Values were considered significant, at p<0.05. Statistical analyses were carried out using doctor SPSS II for Windows (SPSS, Japan Inc, Tokyo, Japan).
RESULTS
Figure 1 shows the patients’ flow chart. During the study period, 63 fetuses were eligible and 40 were subsequently randomly assigned. Consent was not obtained from four parents. Twenty infants were allocated to the milked group and 20 to the control group. A total of 40 VLBW infants were admitted and were analysed for the present study.

Table 2 shows the baseline characteristics of the infants. There were no significant differences in gestational age and birth weight in the two groups. Two infants in the milked group died—one at 15 days owing to sepsis and one at 35 days owing to intestinal perforation, while, three infants in the control group died—one at 8 days owing to intraventricular haemorrhage, one at 26 days owing to intestinal perforation and one at 42 days owing to sepsis. The 1-minute Apgar score was higher in the milked group than in the control group, but the 5-minute Apgar score was comparable in the two groups.
Figure 2 shows the probability of having no transfusion by using the Kaplan–Meier curves. There was a significant difference between the groups in the need for transfusions (log-rank test; p = 0.02).
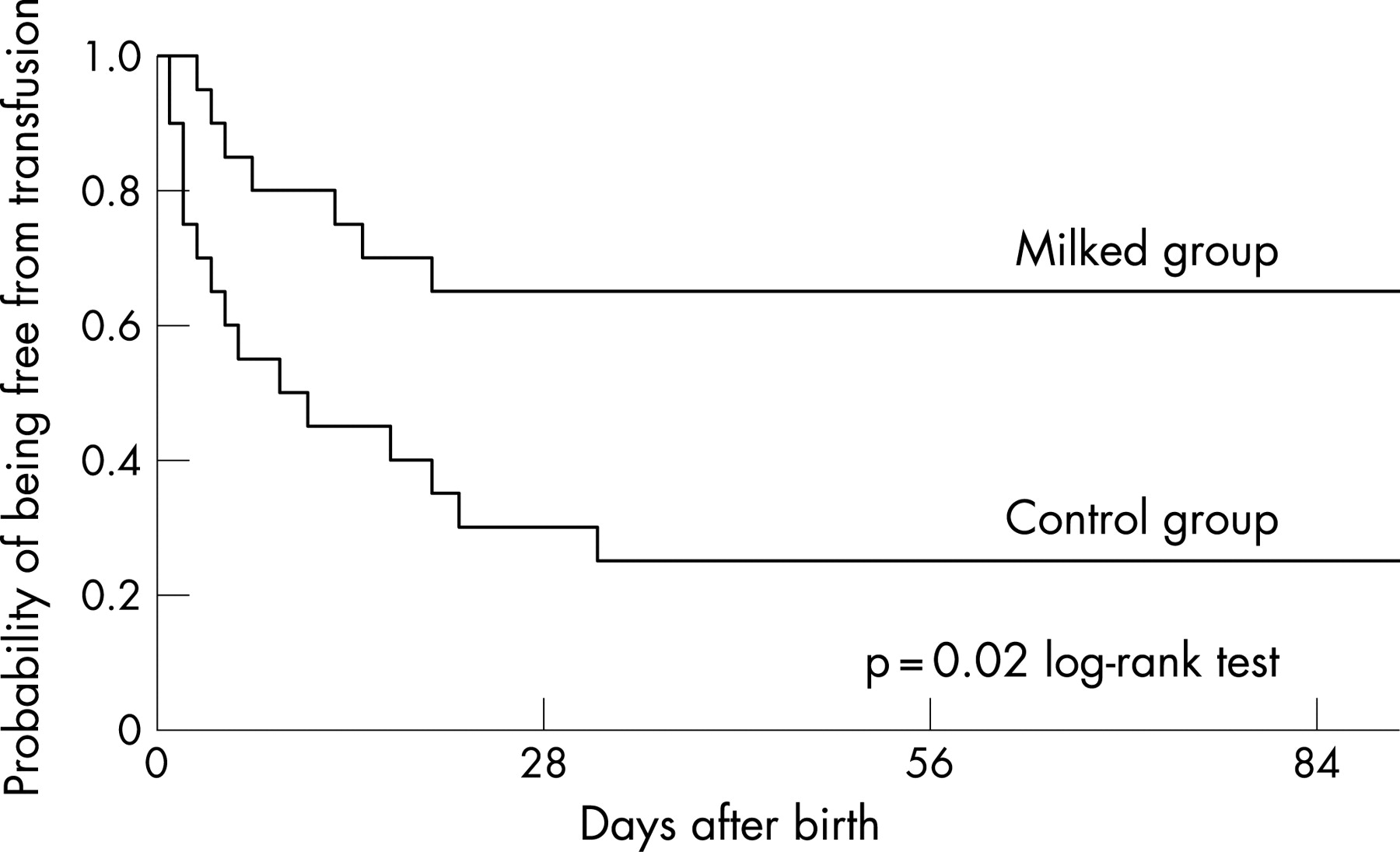
Figure 3 shows the distribution of haemoglobin values at birth and transfusion in infants with or without the milking of the cord. Infants with haemoglobin value <160 g/l and weighing less than 750 g were likely to receive one or more transfusions despite any intervention.

{kind=link}
{kind=link}
{kind=link}
Table 3 shows the clinical characteristics. The initial mean (SD) haemoglobin value in the milked group was significantly higher than in the control group (165 (14) g/l vs 141 (16) g/l, respectively, p<0.01). In the control group, 6/20 (30%) infants had no RBC transfusions compared with 13/20 (65%) in the milked group (p = 0.03). The mean number of transfusions in the milked group was significantly lower than in the control group (0.7 (1.2)/hospital stay vs 2.5 (3.3)/hospital stay, respectively (p = 0.02). The mean peak serum bilirubin and the duration of phototherapy were comparable in the two groups. A significantly shorter duration of mechanical ventilation (p = 0.04) or oxygen supplementation (p<0.01) was seen in the milked group than in the control group. The initial systolic, diastolic and mean blood pressures in the milked group were significantly higher than in the control group (p<0.05).
Table 4 lists the indicators of nutritional status. There was no significant difference between the two groups in the percentage of infants breast fed at 28 days. The day at which feeding of 100 ml/kg milk occurred and the day at which recovery of birth weight occurred were earlier in the milked group than in the control group (p<0.01).
Table 5 shows the major morbidity in the NICU stay. No infants developed polycythaemia in either group. The incidence of RDS, significant PDA, and hyperkalaemia were similar in both groups. Four (20%) infants had grade III or IV IVH in the control group, but only two (10%) infants in the milked group (p = 0.38). Among survivors, 2/17 (11.8%) infants in the control group and 1/18 (5.6%) infants in the milked group had PVL. The incidence of CLD at 36 weeks was significantly lower in the milked group than in the control group (p<0.05).
DISCUSSION
As far as we know, this is the first randomised controlled trial to examine the practice of milking the umbilical cord in very preterm infants. This study showed that umbilical cord milking reduced the need for RBC transfusion and the number of transfusions. The need for transfusion was reduced particularly in infants weighing more than 750 g.
Recent meta-analysis by Ohlsson and Aher showed that the small reduction in the volume of RBC transfusion obtained by using early erythropoietin was of limited clinical importance owing to the increased risk of ROP.5 Therefore, they did not recommend early erythropoietin treatment. A high dose of rHu-EPO also could not completely eliminate the need for RBC transfusion in ELBW infants.3 ,4
Our previous report showed that birth weight, gestational age and haemoglobin value were the best predictors of the need for transfusion in ELBW infants.7 In particular, the initial haemoglobin value is correlated with the need for blood transfusions within the first 3 weeks of life.7 ,14 ,15 It has been noted that the haemoglobin values increase with increasing gestational age16 and that the mean initial haemoglobin value in ELBW infants was 146 (21) g/l and ranges widely from 105 g/l to 188 g/l.7 So it was natural that the concept of placental transfusion was considered in order to expand the circulating blood volume at birth.
In 1993, Kinmond et al first demonstrated that there were significant beneficial haematological and circulatory effects of delayed cord clamping in low birth weight or VLBW infants.8 However, the optimal time for umbilical cord clamping is not known. Immediate umbilical cord clamping deprives the neonate of a significant volume of blood17 and creates a state of potential circulatory compromise,18 resulting in hypotension in premature infants. Six published reports evaluated the relationship between the haemoglobin or haematocrit levels and the timing of umbilical cord clamping in premature infants8 ,9 ,19–22; however, four of these showed no significant association.9 ,19 ,21 ,22 Rabe et al analysed seven randomised trials and noted that delaying cord clamping by 30–120 seconds was associated with less need for transfusions than early clamping.23 On the other hand, Rabe et al pointed out that attempting to transfuse the infants from the placenta, by leaving the cord unclamped for a longer time at birth, may conflict with a perceived need for immediate resuscitation, which is usually done when the neonate is removed from the mother.23 Furthermore, the more seriously ill infants who have a lower birth weight or a shorter gestational age have a greater need for resuscitation at birth and RBC transfusions during the first 3 weeks. Such tiny infants might be expected to have increased heat loss outside a radiant warmer during the 30–45 seconds of late clamping.
Therefore, we attempted to milk or strip the umbilical cord instead of delaying cord clamping so as to not interfere with immediate resuscitation. Of note, Beck recommended this procedure for premature babies in 1941.24 Our study found that umbilical cord milking increased the initial haemoglobin level and decreased the need for RBC transfusions.
We also found that umbilical cord milking was associated with higher initial blood pressure. This is an important finding, since a higher initial mean blood pressure is a vital physiological factor that can improve organ perfusion and may facilitate the neonate’s transition.19 Hypotension in VLBW infants has been associated with poor outcomes, including not only mortality but also IVH, PVL25 and ROP.26
What is already known on this topic
One of the important interventions reducing the need for subsequent blood transfusions is to maximise circulatory volume at birth.
Delayed umbilical clamping is not always practical in very premature babies.
What this study adds
Milking of the umbilical cord is a simple and cost-free method that reduces the number of neonatal blood transfusions.
One important risk factor for IVH is thought to be rapid volume overload.27 Cord milking did not increase the risk of IVH in the present study. Although late clamping also induces a rapid volume expansion, this procedure was associated with a lower incidence of IVH.22 ,23 Several reports have emphasised the importance of initial hypotension as an IVH-inducing factor.28–30 The blood pressure in the milked group was higher than in the control group. The increase in cardiac output to the lung from 8% during fetal life to the 45% immediately after birth necessitates transfer of adequate blood volume.31 When the umbilical cord is clamped before an adequate placental transfusion to the infant has occurred, blood volume might be drawn out of the systemic capillary beds, resulting in relative hypoperfusion. The additional blood received by milking the umbilical cord before the first breath may help to expand lung capillaries and alveoli causing more initial capillary erection.32 Thus, in the milked group, pulmonary capillary erection acts as a “reservoir” as a result of the first breath and may minimise the effect of systemic blood pressure.
Several infants in the control group received oxygen at 36 weeks corrected age. However, unexpectedly, none of the infants in the umbilical cord milked group received oxygen. A shorter duration of mechanical ventilation or O2 supplementation was seen in the milked group. Similar findings have also been reported with delayed cord clamping.8 ,19 Possibly, the additional blood received by cord milking may help to expand the lung capillaries and alveoli causing more initial capillary erection.32 Thus, a sufficient blood volume and a sufficient recruitment of capillary erection may provide structural support to prevent recruitment and de-recruitment with each breath.33 ,34
Our study also showed that infants in the control group were slower to reach the feeding volume of 100 ml/kg and to regain the birth weight than the milked group. One explanation might be associated with the diving reflex. Lack of relative circulatory blood volume as a result of the lower blood pressure in the control group, may result in poor perfusion in the digestive system as the negotiable organs.
Based on our data, the following conclusions can be drawn. First, milking of the umbilical cord contributes significantly to an increased probability that transfusions will not be needed and to a decrease in the number of transfusions. Second, umbilical cord milking was associated with a higher Apgar score at 1 minute, higher blood pressure and shorter duration of mechanical ventilation and O2 supplementation. Third, despite the fact that umbilical cord milking is thought to cause rapid volume loading, this procedure dose not appear to be associated with a risk of IVH.
Given that umbilical cord milking may have both clinical and economic benefits in the management of VLBW infants, further investigation is warranted. There are a considerable number of concerns that need to be studied with respect to the short- and long-term effects of umbilical cord milking. Large trials are needed to examine these concerns.
Acknowledgments
We are especially grateful to Dr T Yamamoto, Dr M Masaoka, Dr Y Miyakawa and other obstetricians for their excellent technical assistance. We also thank the doctors (Dr M Shimada, Dr I Inami, Dr T Kitamur, and Dr S Chinen) and nurses of the NICU. Finally, we thank the parents who consented to inclusion of their baby in this study.
REFERENCES
Footnotes
Competing interests: None.
Linked Articles
- Perspectives
- Fantoms