Article Text

Abstract
Objective: To study late onset systemic infections with coagulase negative staphylococci.
Methods: Prospective longitudinal study of coagulase negative staphylococcal infection in 18 Australasian neonatal nurseries.
Results: From 1991 to 2000 inclusive, there were 1281 cases of coagulase negative staphylococcal (CoNS) sepsis, comprising 57.1% of all late onset infections. The male/female ratio was 1.27:1 (p < 0.05). The incidence of CoNS sepsis was 3.46 episodes per 1000 live births. Most infected babies (71%) were 24–29 weeks gestation at birth (mode 26 weeks). The first positive culture was day 7–14 in 49% of babies (mode 10 days). Five cases of meningitis were reported, an incidence of 0.4% of all CoNS infections. Twenty nine babies (2.3%) had concurrent necrotising enterocolitis and CoNS septicaemia. Four babies (0.3%) died from CoNS infection, but CoNS infection possibly contributed to the death of an additional 20 babies (1.6%). The mortality directly attributable to CoNS infection was significantly lower than that from late onset infections with Staphylococcus aureus (13.1%; relative risk (RR) = 36.1 (95% confidence interval (CI) 13.0 to 100.2) or with Gram negative bacilli (14.2%; RR = 45.5 (95% CI 16.8 to 123.3)).
Conclusions: CoNS are currently responsible for most late onset neonatal infections. Most infected babies are < 30 weeks gestation at birth, and usually present between 7 and 14 days of age. CoNS infections may be associated with necrotising enterocolitis, although causality is unproven. Neonatal CoNS infections are relatively benign: meningitis is rare and mortality low compared with infection from other organisms. Over-vigorous attempts to reduce the incidence of CoNS infections using prophylactic antibiotics are not advisable.
- Staphylococcus epidermidis
- nosocomial infections
- late onset
- necrotising enterocolitis
- meningitis
- CoNS, coagulase negative staphylococci
- CSF, cerebrospinal fluid
- NEC, necrotising enterocolitis
Statistics from Altmetric.com
Before 1980, most late onset or nosocomial infections in neonatal nurseries in industrialised countries were caused by Staphylococcus aureus and Gram negative bacilli.1–,7 For the last 20 years, however, coagulase negative staphylococci (CoNS) have predominated and been responsible for at least half of all late onset infections.1–,7 Babies with CoNS infection are smaller and more premature than controls, but even after controlling for prematurity, they stay longer in neonatal intensive care units than non-infected babies, and at considerable cost.5
There is a dearth of data on the complications and outcome of neonatal CoNS infections. As skin commensals, CoNS are common contaminants of cultures of blood and cerebrospinal fluid (CSF), which complicates the interpretation of positive blood and CSF culture results. Stoll et al1 found that very low birthweight babies with CoNS infection had a significantly higher death rate (10%) than uninfected babies (7%), although the mortality associated with Gram negative (40%) and fungal (28%) sepsis was much higher. Karlowicz et al7 reported a mortality for CoNS sepsis of 1.3% (four of 277 infected babies).
In this paper, we report the incidence, associations, and outcome of CoNS infections studied in a large prospective study of neonatal infections in Australia. The strengths of our study are the very large number of infections studied, the ability to calculate rates of infection as a proportion of all live births, and the involvement of clinicians to make decisions about the clinical significance of CoNS infections. The weaknesses of our study are that data were not collected on risk factors for CoNS sepsis, such as the presence of indwelling catheters, speciation of CoNS was not routinely performed, and the definition of CoNS sepsis is open to debate.
METHODS
This report includes data collected prospectively by the Australasian Study Group for Neonatal Infections (ASGNI) for 10 years from 1 October 1991 until 30 September 2000 inclusive. The ASGNI is a group of neonatal clinicians in Australia and New Zealand. In 1991, the group comprised seven neonatal units, but by 1995 it included 18 units in Australia and New Zealand, of which 11 are attached to maternity hospitals and able to provide data on the annual number of live births. These live births represent 10–20% of all annual births in Australia.
Babies who fulfilled the study definition of sepsis were reported on a standard questionnaire, recording the baby's initials but no other identifying data, the birth weight, gestational age, race, sex, time of first positive culture, organism, and results of blood and CSF cultures. Participants were asked to report associated infections, such as pneumonia or skin sepsis. The only outcome recorded was survival. Institutional bioethics committee approval was obtained to collect the data.
Neonatal sepsis was defined as clinical sepsis6,8 (usually one or more of fever, hypothermia, or temperature instability, apnoea, bradycardia, increased oxygen requirement, feed intolerance, lethargy, and hypotonia) together with a pure growth of a single organism from blood or CSF. When the positive culture was a possible contaminant, such as CoNS, the clinician was asked to report the case only if the baby was clinically septic, and had at least one abnormal haematology test (abnormally high or low peripheral neutrophil count or abnormal immature to total white cell ratio, based on the reference ranges of Manroe et al,9 or thrombocytopenia < 150 × 109/l). Clinicians were asked not to report likely contaminants. Blood cultures growing more than one organism were considered to be contaminants.
Bacterial meningitis was defined as a clinical picture consistent with meningitis, and either a positive CSF culture or elevated CSF white cell count (> 100 × 106/l or > 100/μl) in association with a positive blood culture. Babies with ventricular shunt infections were excluded. Clinicians were asked to report the immediate outcome of each infection, as follows: S, survived; D, died from sepsis; P, died, possibly from sepsis; U, died, unrelated to sepsis. Septicaemic babies who died from necrotising enterocolitis (NEC), as defined by Isaacs and Moxon,8 were always classified as P—that is, possibly having died from sepsis.
For this study, the only babies included in the analysis were babies with late onset sepsis, defined as sepsis occurring more than 48 hours after delivery. Babies were therefore included if they were reported as having CoNS septicaemia and/or meningitis with onset on day 3 or later. The rate of CoNS sepsis was determined as the sum of the number of inborn babies with CoNS infection as a proportion of all live births at the attached maternity hospitals.
Statistical analysis was by analysis of relative risks (RR) with 95% confidence intervals (CI).
RESULTS
In the 10 years from 1991 to 2000, there were 1281 episodes of sepsis due to CoNS, affecting 1249 babies. The 1281 episodes represented 57.1% of the total number of 2243 episodes of late sepsis reported. Of the episodes of CoNS sepsis, 717 (56.0%) affected males and 564 females (44.0%), giving a male/female ratio of 1.27:1 (p < 0.05).
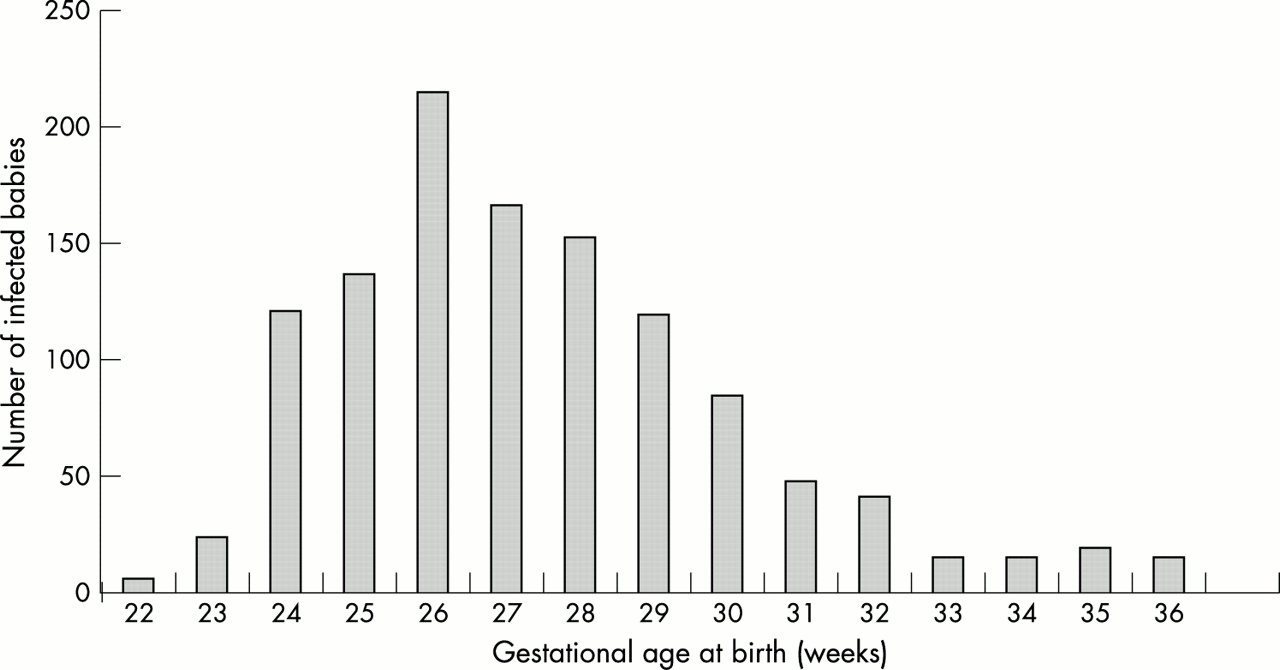
There were 1096 episodes of CoNS sepsis affecting 1070 inborn babies in neonatal units attached to maternity hospitals, and over the same period there were 316 559 live births in those hospitals. This gives an incidence of late onset coagulase negative staphylococcal sepsis of 3.46 episodes per 1000 live births. Australian Aboriginal mothers gave birth to 10 229 of the inborn babies, and they experienced 41 episodes of CoNS sepsis, an incidence of 4.01 per 1000 live births. The incidence in Australian Aboriginal babies was not significantly different from the incidence in non-Aboriginal babies (RR = 1.16, 95% CI 0.85 to 1.47). The gestational ages at birth of the infected babies ranged from 22 weeks to full term (fig 1⇓). Most (71%) of the babies had gestational ages between 24 and 29 weeks, and the mode was 26 weeks gestation. There were 104 babies (8.1%) born at 37 weeks gestation or later. The mean (SD) birth weight of infected babies was 937.7 (759.7) g (range 370–4402).

Gestational age of infected babies at birth. NB 81 babies born at > 37 weeks gestation are not included.
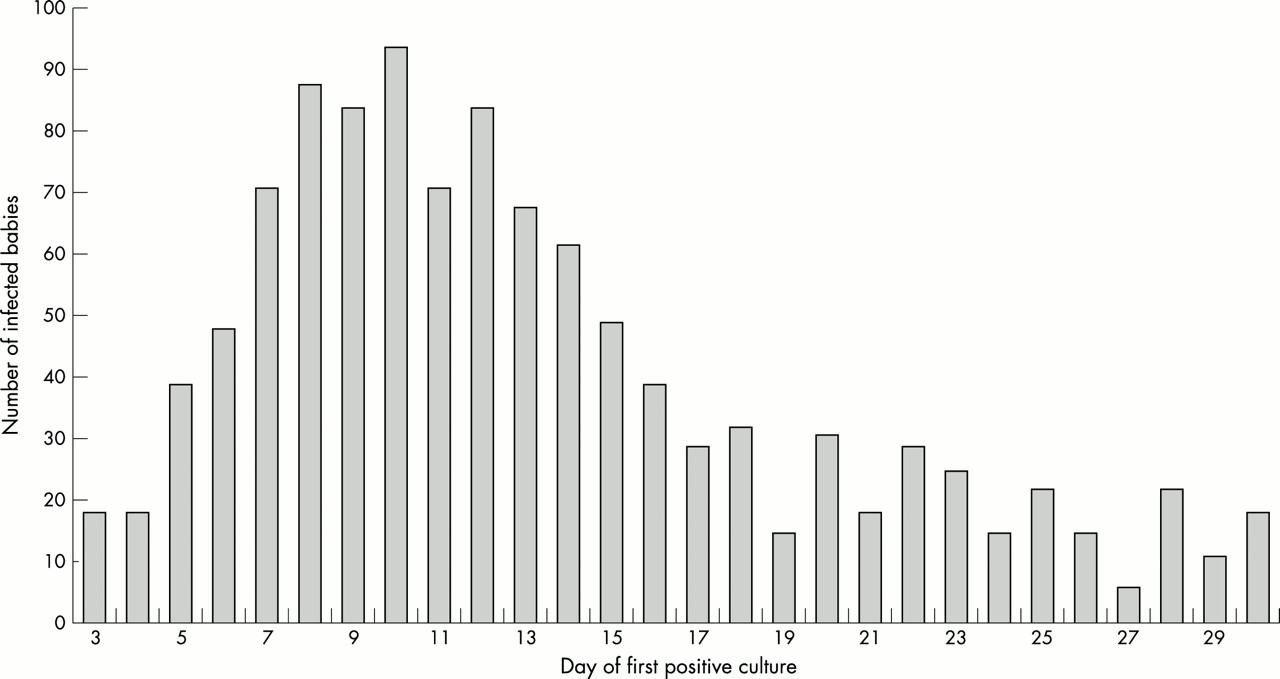
Figure 2⇓ shows the day of first positive culture. The peak age was between days 7 and 14 (49% of all cases), particularly days 8–12 (33% of the total), with day 10 the single most common day. However, 12.5% of all babies had a positive culture after 30 days of age.

{kind=link}
{kind=link}
Day of first positive culture of coagulase negative staphylococci from blood or cerebrospinal fluid. NB 160 babies whose first positive culture was at > 30 days old are not included.
Table 1⇓ reports the infections associated with CoNS sepsis. There were five cases of meningitis, an incidence of 0.4% of all CoNS infections. The single most commonly reported association was with NEC (29 babies). Other important associations were with skin sepsis (14), urinary tract infection (two), and infective endocarditis (three). Only six babies were reported to have concurrent pneumonia.
Infections associated with 1281 episodes of coagulase negative staphylococcal sepsis, 1991–2000
Four babies (0.3%) were reported to have died as a direct result of CoNS sepsis: a baby of gestational age at birth 23 weeks and birth weight 645 g, who died aged 4 days; a baby of gestational age at birth 26 weeks and birth weight 511 g, who died aged 10 days; a baby of gestational age at birth 27 weeks and birth weight 485 g, who died aged 6 days; and a baby of gestational age at birth 27 weeks and birth weight 760 g, who died aged 7 days. None had meningitis.
In addition, 20 babies (1.6%) were reported as having died, with CoNS sepsis having possibly contributed. Of these 20 babies, eight died from NEC. Another 43 babies died, but death was classified by the clinician as unrelated to their recent CoNS infection. In comparison, 289 babies developed late onset S aureus septicaemia/meningitis, of whom 38 (13.1%) died, and the mortality from late onset sepsis caused by all Gram negative bacilli, excluding babies with NEC, was 81 (14.2%) of 569 babies. RR and 95% CI compared with CoNS infection was 36.1 (13.0 to 100.2) for S aureus infection and 45.5 (16.8 to 123.3) for Gram negative bacillary infections.
DISCUSSION
CoNS infections have emerged since the 1980s as the leading cause of late onset or nosocomial sepsis in neonatal nurseries in industrialised countries.1–,7 In recent years they have been reported as causing over 50% of all late onset infections. It has been calculated5 that each CoNS infection prolongs the hospital stay of a very low birthweight baby by an average of 14 days at a cost of US$25 000. The reasons for the emergence of CoNS as such important pathogens are probably multifactorial, attributable in part to invasive procedures, the thin, fragile skin of increasingly premature babies, and the use of central venous catheters and lipid emulsions in parenteral nutrition.8–,11
CoNS, being normal skin commensals, are common contaminants of blood and CSF cultures, which complicates the interpretation of culture results and our ability to describe the natural history of CoNS infections. Quantitative or semiquantitative cultures increase the reliability of culture results,12,13 but are too expensive for routine use. We recognise that the interpretation of what constitutes sepsis by one clinician may differ from another, which necessarily introduces a degree of uncertainty as to the validity of all our cases. US researchers define CoNS sepsis as requiring two positive cultures from venous or catheter.6,7 It is not, however, routine practice in Australasia to take two cultures from a baby with suspected sepsis before starting antibiotics, so we were unable to use this definition. We therefore used a combination of a clinical definition together with the requirement for haematological evidence of sepsis in order to strengthen our definition of CoNS sepsis.
The overall incidence of CoNS sepsis was 3.46 per 1000 live births. We did not find an increased incidence in Australian Aboriginal pregnancies. In contrast, the incidence of early onset group B streptococcal sepsis is significantly higher in the Aboriginal than the non-indigenous Australian population.14
We did not collect data that would allow us to examine all the potential risk factors for development of CoNS sepsis, including central venous catheter and fat emulsion use.10–,13 We found previously, however, that about 50% of babies with CoNS sepsis had a central venous catheter in situ at the time of sepsis development.3
There is relatively little published on the mortality of CoNS sepsis. The mortality of very low birthweight babies who developed late onset sepsis with any organism in the National Institute of Child Health and Human Development (NICHD) study1 increased from 7% to 17%, but 40% of babies with Gram negative sepsis and 62% of those with Pseudomonas infection died, compared with only 10% with CoNS sepsis. Karlowicz et al7 found a 1.3% mortality for CoNS infections, compared with 56% for Pseudomonas sp, 19% for Escherichia coli, and 6% for S aureus. We found that 0.3% of the babies in our study died as a direct result of CoNS infection, and that sepsis possibly contributed to the deaths of a further 1.6%, giving a maximum estimate of the mortality of 1.9%. This figure is consistent with data from the United States.1,7 We asked units participating in our study about their antibiotic policy for suspected late onset sepsis. Nine (50%) used vancomycin and an aminoglycoside as the first line empirical treatment, and the mortality from CoNS sepsis was no different between units that used vancomycin as first line treatment and those that used ampicillin, or another anti-staphylococcal agent, flucloxacillin, together with an aminoglycoside. We did not routinely record antibiotic sensitivities of CoNS isolates, but local data suggest that at least 80% of isolates are resistant to flucloxacillin. Thus, it appears that the mortality from CoNS sepsis is low, even if methicillin resistance is common and vancomycin is not used as first line treatment. Karlowicz et al7 similarly reported no difference in CoNS mortality when oxacillin was used instead of vancomycin as first line treatment for suspected late onset sepsis. One possible explanation is that gentamicin has sufficient activity against CoNS to treat the organism or at least to prevent overwhelming infection. Another possibility is that CoNS are often of sufficiently low pathogenicity that host defences are able to cope with the low level bacteraemia and prevent the infection from becoming fulminant.7
We found an interesting association between CoNS sepsis and NEC, with 2.3% of all infected babies having concurrent NEC, and eight babies who died from NEC having positive blood cultures for CoNS. It is possible that the positive blood cultures are contaminants or result from central catheter related sepsis, but the cultures could reflect a genuine causal relation. Scheifele and colleagues15,16 first proposed a pathogenic role for CoNS infections in NEC, describing an association with a delta-like toxin produced by the organisms. They were supported by surgical colleagues.17 Others found no differences between the CoNS isolated from babies with NEC and controls,18 or were unable to find a consistent infectious agent in babies with NEC.19 Ng and colleagues,20 however, described a convincing scenario of preterm twins given expressed breast milk contaminated with Staphylococcus epidermidis who developed septicaemia with this organism and died from NEC.
The role of CoNS in meningitis is equally controversial. CoNS are known to be a common cause of central nervous system infections in patients with intraventricular catheters or shunts. When cases of neonatal CoNS meningitis are described in the absence of foreign material, however, it is hard to know whether or not they represent CSF contaminants. Gruskay et al21 described 10 babies with CoNS meningitis, but with normal CSF white cell counts and chemistry, strongly suggesting that the organisms were contaminants. The reliability of laboratory based studies with minimal clinical input is uncertain. A laboratory based Australian study22 reported that six (5%) of 116 babies with neonatal meningitis from 1987 to 1989 were infected with CoNS, while between 1975 and 1991 in Britain the reported incidence23 was 28 (1.5%) of 1846 babies. In one small, clinician based study from Oxford, no cases of CoNS meningitis were reported,24 whereas in a larger, active surveillance study,25 conducted through the British Paediatric Surveillance Unit, clinicians notified three cases of CoNS meningitis in one year out of a total of 274 babies with meningitis (1.1%).
Three babies in our study had endocarditis caused by CoNS. Although S aureus is the major cause of neonatal endocarditis, CoNS was the infecting organism in three of 25 cases in one review of neonatal endocarditis,26 and two of 11 in another recent review.27 It is particularly likely to cause right sided endocarditis.26,27 Although neonatal endocarditis was once almost uniformly fatal, the mortality has improved. None of the three babies in our study died.
There have been some reports linking CoNS infection with pneumonia, notably a series from Hall et al,28 who identified 12 babies with hospital acquired pneumonia out of 27 with CoNS bacteraemia. Nine of the 12 were intubated at the time, and the other three had been intubated previously. We found a far lower incidence of pneumonia. This could be due to under-reporting or it may be a genuine change. One possible explanation is the far shorter duration of endotracheal intubation since the widespread use of artificial surfactant.29
We did not include babies reported as having CoNS infection before 3 days of age, because our definition of late onset sepsis specified positive cultures occurring after 48 hours of age. On reviewing our records, there were only four reports of babies with CoNS infection on day 1, and three on day 2, and none of these babies died. The low number of reports of early onset CoNS sepsis may have been because of scepticism about the significance of positive cultures for CoNS in the first two days after birth. The NICHD reported 22 neonates with early blood cultures positive for CoNS.31 On chart review, it was felt that 11 of them had “true” early onset sepsis, including three with persistently positive cultures and four with pulmonary haemorrhage. The babies affected were all extremely premature, with birth weight under 1500 g, and were at high risk for death and morbidity unrelated to sepsis.31 The validity of reports of early onset CoNS sepsis remains uncertain. In our study, the inclusion of reports of early onset CoNS infections would not have materially altered any of our conclusions.
We have reported previously that the overall incidence of late onset neonatal infection appears to be relatively constant in any one institution from year to year, although the organisms responsible may vary greatly over time.32 The major factors determining the rate of late onset sepsis appear to be the degree of prematurity and the use of invasive procedures.1–,3 We and others have described CoNS infections as relatively benign infections, at least in comparison with infections with Gram negative bacilli or S aureus.1,3,7 CoNS infections rarely cause meningitis, and the mortality is low. Over-vigorous attempts to reduce the incidence of CoNS infections, for example by the use of prophylactic vancomycin, not only run the risk of inducing antibiotic resistance, but also of replacing CoNS infections with infections caused by more virulent organisms, and would be ill advised.
Acknowledgments
Thanks to many colleagues for data collection, including particularly, Andrew Daley, Mary Poynten, David McIntosh, Michael Nissen, Melanie Wong, Janelle Meyers, Kate Panaretto and Anne Arthur.
The Australasian Study Group for Neonatal Infections consists of: C Barfield MB FRACP (Monash Medical Centre, Melbourne, Australia); D Bouchier MB FRACP (Waikato, New Zealand); G Bury MB FRACP (Hobart Hospital, Tasmania, Australia); I Bucens MB FRACP; A Ruben MB FRACP (Royal Darwin Hospital, Darwin, Australia); D Cartwright, MB FRACP (Royal Women's Hospital, Brisbane, Australia); T Clothier MBBS; J Ehrlich MB FRACP; F Morey PhD (Alice Springs Hospital, Alice Springs, Australia); B Darlow MB FRACP (Christchurch, New Zealand); S Fraser MB FRACP (Mercy Hospital, Melbourne, Australia); L Gilbert MD FRCPA (Westmead Hospital, Westmead, Australia); K Grimwood MD FRACP; P McDougall MD FRACP; J Royle, MB FRACP (Royal Children's Hospital, Melbourne, Australia); D Henderson-Smart MD FRACP; H Jeffery MD FRACP (King George V Hospital, Sydney, Australia); D Isaacs MD FRACP; J Peat PhD (statistician) (Royal Alexandra Hospital for Children, Sydney); R Kohan MB FRACP (King Edward Memorial Hospital, Perth, Australia); A McPhee MB FRACP (Women's and Children's Hospital, Adelaide, Australia); R Messer MB FRACP (Cairns Base Hospital, Cairns, Australia); C Minutillo MD FRACP (Princess Margaret Hospital, Perth, Australia); D. Tudehope MD FRACP (Mater Hospital, Brisbane, Australia); J Whitehall MB FRACP (Kirwan Hospital, Townsville).