Article Text

Abstract
BACKGROUND Thrombosis is a relatively rare event in children. However, many conditions in the neonatal period result in an increased risk of thrombus formation. The major risk factor is the indwelling intravascular catheter. Numerous small studies have reported experience of thrombolytic treatment for neonatal thrombotic disease with a wide range of different thrombolytic agents in various forms of administration, dosage, and duration, but no conclusions on the most effective treatment for neonates has been reached.
OBJECTIVE To assess the efficacy and safety of thrombolytic treatment of neonatal catheter related thrombus (CRT) formation with recombinant tissue plasminogen activator (rt-PA).
METHOD Over a six year period, 14 neonates with CRT were treated with the same rt-PA protocol (an initial bolus of 0.7 mg/kg over 30–60 minutes followed by infusion of 0.2 mg/kg/h).
RESULTS Complete clot dissolution was documented in 11 patients, and partial clot lysis in two patients, leading to a patency rate of 94%. In two cases, local bleeding occurred, resulting in treatment failure in one case. Finally, antithrombin III substitution was required in one case. No other complications such as severe bleeding were recognised.
CONCLUSION With the use of close clinical and haematological monitoring on a neonatal intensive care unit combined with serial two dimensional colour echocardiography, the present rt-PA protocol was shown to be a safe and effective method of clot dissolution in neonates.
- thrombus
- thrombolysis
- blood clot
- tissue plasminogen activator
Statistics from Altmetric.com
Thrombosis is a relatively rare event in children. In adults the incidence of thrombotic complications increases with increasing age.1 However, in childhood, newborns are at the greatest risk of thromboembolic complications.2 The incidence of clinically apparent neonatal thrombosis in recent reports varies from 5.1 per 100 000 births3 to 2.4 per 1000 admissions.2 ,4
There are numerous clinical and environmental conditions during infancy and childhood, such as peripartum asphyxia, infant of diabetic mother, renal disease, dehydration, septicaemia, malignant or autoimmune diseases, trauma or surgery, that result in increased thrombin generation with subsequent fibrin or thrombus formation.2-6 One of the major risk factors is undoubtedly the widespread use of indwelling intravascular catheters. The reported incidence is 13–14% in term infants,7 ,8but rises to 64–85% in low and very low birthweight infants,9 although thrombosis prophylaxis with low dose heparin is used in probably all neonatal units when central lines are in use. Clinical outcome is often serious.5 ,10
Although small catheter related thrombi (CRTs) do not usually cause a problem if the line is simply removed, there is general agreement that treatment is needed in cases of large and fragile CRTs, because of the risk of embolism. This is particularly high in persistent ductus arteriosus and persistent foramen ovale. Treatment varies from centre to centre, with a wide range of administration, dosage, and duration of treatment, and different thrombolytic agents—for example, streptokinase, urokinase, and recombinant tissue plasminogen activator (rt-PA).
rt-PA offers several theoretical advantages to the newborn infant, including short half time, minimal antigenicity, direct activation of plasminogen, lack of inhibition by α2 antiplasmin, and localisation of fibrinolytic activity.11 ,12 The literature on thrombolytic treatment with rt-PA for neonatal thrombotic disease contains numerous reports of single cases and small series,3 ,12-18 but no conclusions about the efficacy and safety of thrombolytic treatment in neonates can be drawn.
The aim of this study was to assess the efficacy and safety of a thrombolytic treatment for neonatal CRT, using a standardised rt-PA protocol.
Materials and methods
STUDY DESIGN
Over six years, all neonates in a critical condition—for example, severe neonatal sepsis, prolonged asphyxia, severe respiratory distress syndrome, see also table 2—who developed CRT were matched for possible fibrinolytic treatment. The diagnosis of formation of an intracardiac or great vessel thrombus was established by two dimensional echocardiography (see example in fig 1) and clinical examination in 14 neonates. All patients were monitored in the neonatal intensive care unit and were treated with rt-PA. All data were collected prospectively, including birth weight, gestational age, underlying disease, treatment regimen, clot patency, and complications or side effects.
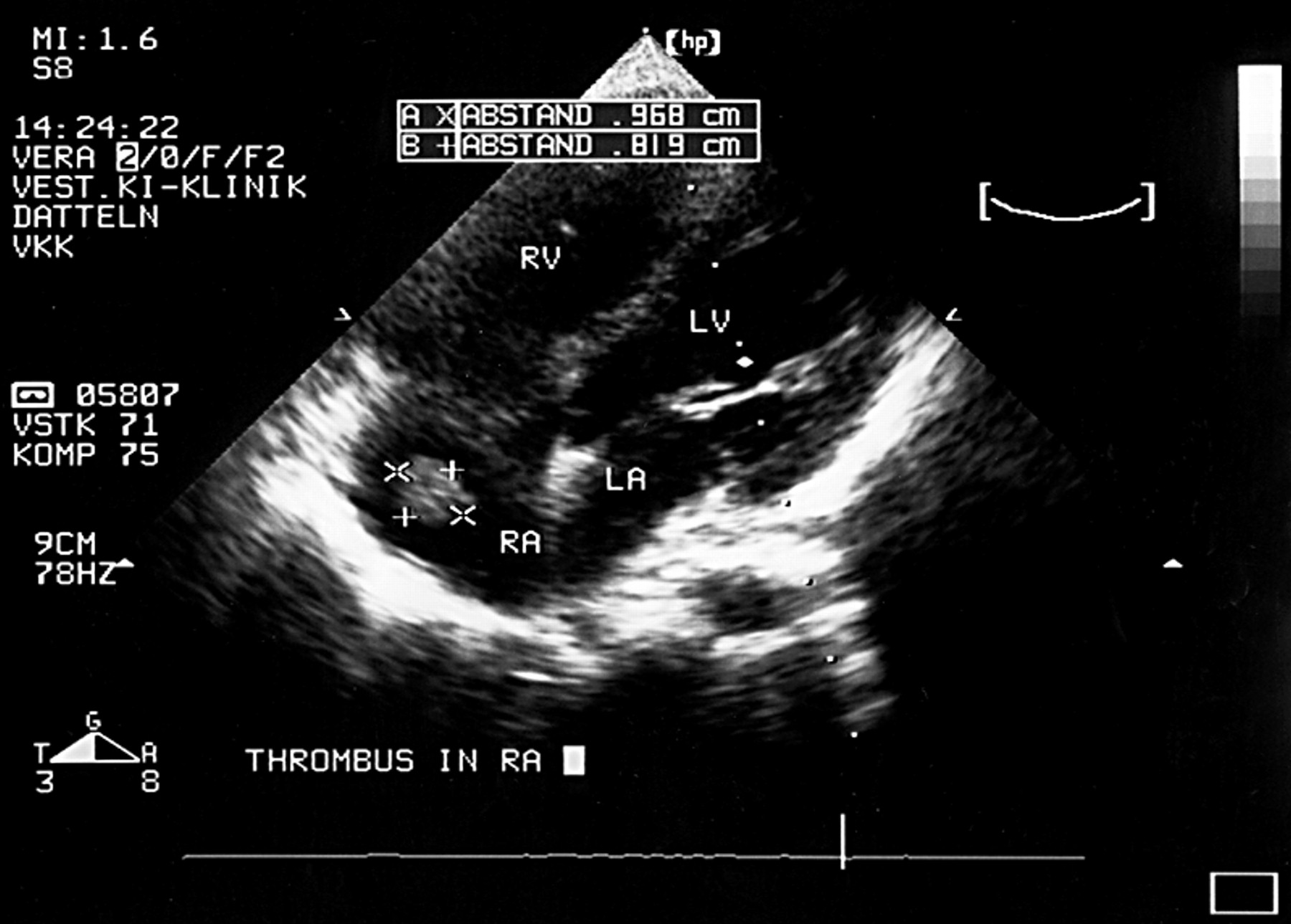
Thrombus formation in the right atrium (four chamber view). RV, Right ventricle; LV, left ventricle; RA, right atrium; LA, left atrium.
EVALUATION BEFORE TREATMENT AND CONTRAINDICATIONS
Before initiation of rt-PA treatment, coagulation studies, including prothrombin time, activated partial thromboplastin time, fibrinogen, and fibrin split products, were obtained to evaluate possible bleeding disorders.19 Additional studies included complete blood cell counts and detection of protein C or protein S deficiency or activated protein C resistance and other haemolytic disorders. All patients had a clinical and radiological evaluation to ensure the absence of contraindications, such as acute intracranial, pulmonary, or gastrointestinal bleeding.
RT-PA PROTOCOL
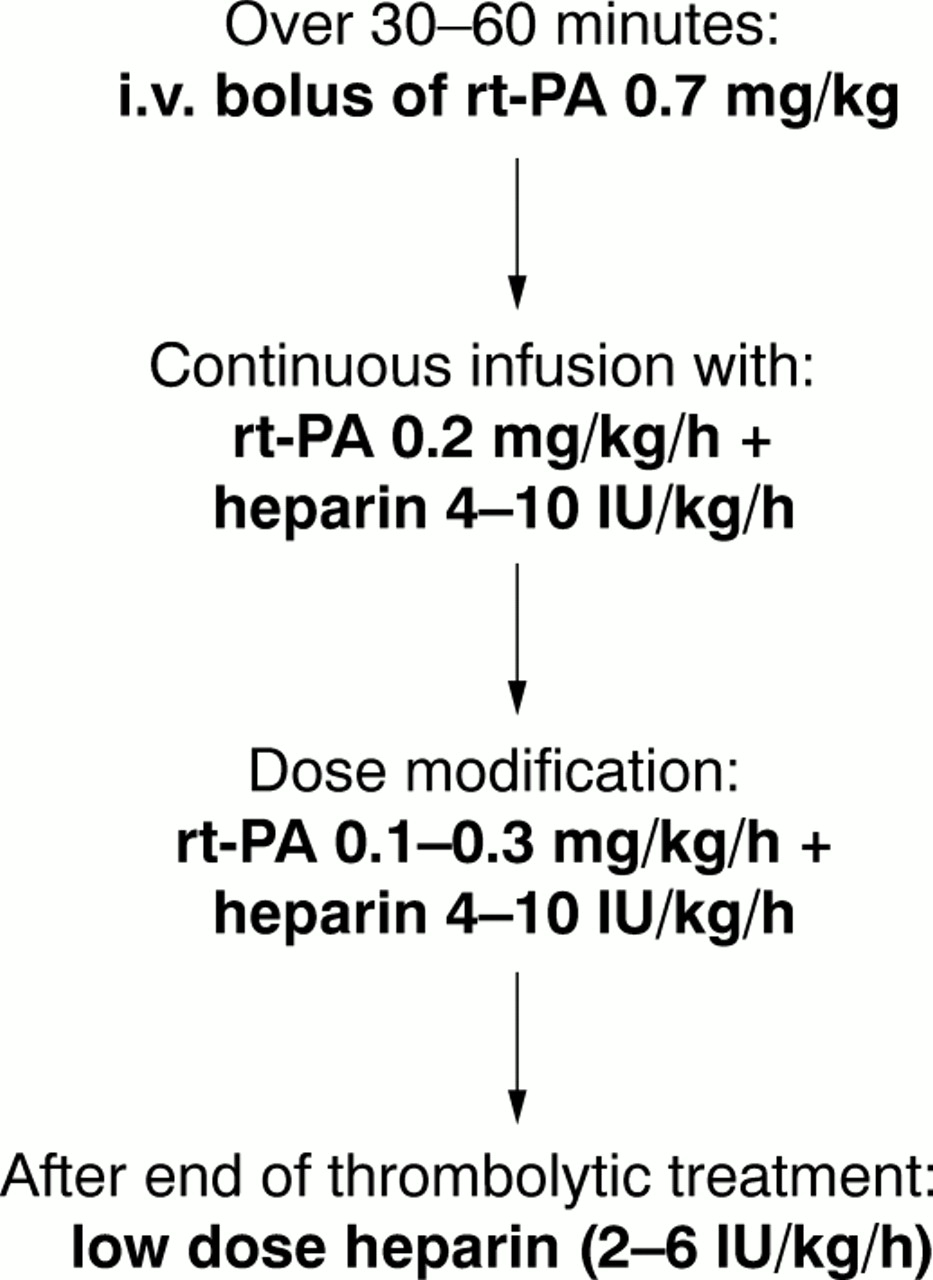
By analysing rt-PA studies in adults, we created the rt-PA protocol given in fig 2. Babies were treated with rt-PA (Actilyse; Boehringer, Ingelheim, Germany) if their parents consented. Coagulation values were measured at least once a day to keep them in the preferred range (table 1).19 rt-PA was given intravenously mostly by using a new central line. Sometimes the affected catheter or peripheral venous lines were used.

{kind=link}
{kind=link}
Schedule for thrombolytic treatment with rt-PA in neonatal period. Dose modification depended on the success of the thrombolytic treatment, complications, and coagulation status (see also table 2). Heparin prophylaxis was continued as long as central venous lines were required.
Selected values (taken from Weiner et al18) for components of the coagulation, coagulation inhibitor, and fibrinolytic system in neonates
TREATMENT MONITORING
The effect of the thrombolytic treatment was controlled at least daily by two dimensional echocardiography. Treatment was stopped in the case of total clot lysis, partial clot lysis with only minor clot residue after five days of treatment, or complications, such as general or significant local bleeding or coagulation disorders. To detect organ bleeding, in particular intracerebral bleeding, an ultrasound scan was performed at least twice a week. To control thrombolysis and anticoagulation, haemoglobin, platelet count, prothrombin time, activated partial thromboplastin time, antithrombin III, fibrinogen, and fibrin split products were assayed. To avoid a reoccurrence of thrombosis, after rt-PA treatment low dose heparin treatment was initiated and continued as long as central venous lines were required.
LITERATURE REVIEW
All reports of rt-PA use in neonates found in Medline by the keywords neonates-infants-thrombus formation-thrombolysis-rt-PA-urokinase-streptokinase were reviewed. Basic data, thrombus location, rt-PA and heparin dosage regimens, treatment duration, complications, labour findings, and clot outcome were determined as far as possible.
Results
The diagnosis of CRT was established by two dimensional echocardiography (except for patient 14 (table 2) for whom the diagnosis was made by clinical examination), at an average of 13 days of life (range 3–22) (except for patient 12, in whom the CRT was detected at the corrected age of 6 months). The latter was included because of extreme immaturity with prolonged growth failure and because he remained in the neonatal intensive care unit.
Clinical data
Neonates with sepsis (71%), preterm delivery (64%), or respiratory distress syndrome (57%), and infants of diabetic mothers (43%) were most affected (table 2), whereas persistent pulmonary hypertension (29%), peripartum asphyxia, small size for gestational age (each 21%), meconium aspiration (14%), extreme immaturity (birth weight ⩽ 1000 g or gestational age ⩽ 28 weeks; 14%), patent ductus arteriosus, transient tachypnoea, and hypoglycaemia (each 7%) were rarer events.
In 10 cases, the precipitating cause was an umbilical venous catheter, in three cases (21%) an umbilical artery catheter, and in one case a central venous line.
Complete clot dissolution was documented in 11 patients, and partial clot lysis in two patients; in the first of these, the thrombus had disappeared at the time of discharge, and in the second the thrombus was completely dissolved by 9 months of age. Duration of lysis was on average three days (range one to five). The patency rate was 94%. In one patient (number 4), rt-PA administration was discontinued because of local bleeding from various venepuncture sites. In another patient (number 10), treatment had to be interrupted for three hours because of the same minor complications; after the infusion was stopped, the symptoms subsided and reinstitution of rt-PA treatment was successful. Severe complications such as intracranial bleeding were not seen. In patient number 2, we were able to reduce the rt-PA dose on the second day of treatment because of rapid clot lysis, and in five patients the dose had to be increased by the use of a repeated bolus (patients 9 and 14), a higher dosage (patients 6, 8, and 9), or a second infusion protocol (patient 12).
Coagulation was successfully prolonged in 11 cases; in patient 14 lysis had to be interrupted three times because of low fibrinogen levels, but was finished successfully. In patient 8, antithrombin III had to be substituted. In addition, coagulation studies showed a modest decrease in fibrinogen concentration (100–150 mg/dl) in seven cases; a transient abnormal elongated prothrombin time and activated partial thromboplastin time were seen in a couple of patients, but all values were restored to normal after treatment was finished. Neither severe bleeding complications, such as intracranial haemorrhage, nor other side effects, such as allergic reaction to the thrombolytic agent, were observed.
Discussion
The thrombotic risk of central lines used in neonates7-9 and the pathophysiology of thrombogenesis2 ,11 ,20-23 have been extensively reported. Since the use of central catheters in neonates, CRT is an increasingly observed complication,4-7 ,20 and, although overall it is still rare, in major neonatal units it is increasing.
Effective and safe thrombolytic treatment is essential in the management of neonates and infants with life threatening thrombosis. Efficient thrombolytic agents available are streptokinase, urokinase, and rt-PA. Administration of streptokinase has been abandoned because of its antigenic qualities, relatively long half time (20–30 minutes), and systemic side effects.24 Nowadays, rt-PA is commonly recommended, because of its short half time (about five minutes), non-antigenic qualities, and local specific action on plasminogen bound fibrin.25 There are established protocols for fibrinolytic treatment with rt-PA in adults,26 ,27 and the efficacy of thrombolysis in childhood has been documented.28-30
However, there is still very little experience with fibrinolytic treatment in the neonatal period. Treatment for neonatal thrombosis remains controversial, guidelines are available but rare,12 ,23-31 and randomised double blinded trials are still lacking. Therefore many doctors follow adult guidelines.32-35 Table 3 gives an overview of studies focusing on thrombolytic treatment with rt-PA in neonatal arterial and venous diseases, including CRT and spontaneous thrombotic disease. The overall patency rate of 94% (68% for complete clot dissolution and 26% for partial clot dissolution) is comparable with our experience (94% patency rate: 79% complete clot dissolution and 14% partial clot dissolution). Comparison of the reports of a low dose rt-PA regimen (0.02–0.08 mg/kg/h)36 ,37 with those of a high dose regimen (0.1–1 mg/kg/h)12 ,29 ,38 ,39 shows an apparently significant difference in patency rate (81%v 95%), although in the first group an initial bolus was given. In both groups, complications ranged from none to severe, but, for both patency rate and complications, data collection was too random to draw any conclusions.
Literature review (Medline) on recombinant tissue plasminogen activator (rt-PA) treatment in neonatal period
Another comparison between bolus or no bolus shows interesting results. Whereas in the bolus group 95% of the patients were detected with positive clot outcome (39 of 56 patients (70%) with complete, and 25 of 56 patients (25%) with partial, clot dissolution), in the no bolus group only 88% (16 of 23 (67%) with complete, and 5 of 24 (21%) with partial, clot dissolution) showed an effect. Again, the groups are very small and bolus dose varies widely, so that conclusions should be made carefully. However, these results seem to justify an rt-PA bolus before continuous infusion.
In addition, thrombosis prophylaxis with low dose heparin is widely recommended, but the administration of heparin is controversial and the different regimens ranged from no heparin to low dose to high dose treatment during thrombolytic treatment. In most reports, administration of low dose heparin (an average of 5 IU/kg/h) was recommended. Statistical analysis of this data collection gives no further information about suitable thrombolytic treatment in the neonatal period because of inhomogeneous and incomplete data collection in several reports. Nevertheless, thrombolytic treatment with rt-PA combined with low dose heparin administration seems to be very efficient and safe.
There are still some reports of the successful use of urokinase40-44 and even streptokinase36 for thrombotic disease in the neonatal period. Randomised double blind trials, based on results from adult patients, have led to the recommendation that rt-PA should be used on the one hand37and equal benefits for rt-PA and urokinase40 on the other. rt-PA seems to act faster and to have more side effects.40Interestingly, several authors4 ,19 ,39 reported successful rt-PA treatment after insufficient trials with urokinase.
Reports differ with regard to the incidence of complications.14 ,31 ,38 In our experience, severe complications were rare and intracerebral haemorrhage did not occur. This is in agreement with other reports.45
To summarise, the literature does not provide enough information to enable recommendations to be made about rt-PA use in the newborn. The present rt-PA protocol with high dose infusion after an initial bolus seems to be an efficient and safe conservative procedure for neonatal clot dissolution. Although a homogeneous collection of cases has been presented, the study has several limitations. However, we feel that these promising results can be used as a starting point for further investigation.