Article Text

Abstract
AIMS The ability of oral vitamin K to eliminate all risk of vitamin K deficiency bleeding during the first three months of life was studied.
METHODS Babies (n=182 000) in the north of England judged well enough to be offered milk within 12 hours of birth were given 1 mg of phytomenadione (vitamin K1) suspended in a medium chain triglyceride oil by mouth at delivery between 1993 and 1998. The parents of those who were breastfed were given a further three doses to give to the baby once every two weeks after discharge.
RESULTS Four breastfed babies developed late vitamin K deficiency bleeding. In two, staff failed to follow policy guidelines, and in two there was undiagnosed α1 antitrypsin deficiency. Audit suggested that 93% of breastfed babies had all four doses, as advised.
CONCLUSIONS An oral product that parents can administer themselves would be popular if licensed, but the total dose offered may need to be more than in this study if babies with undiagnosed liver disease are to be protected.
- vitamin K prophylaxis
- bleeding
- breast feeding
Statistics from Altmetric.com
With the recognition that vitamin K deficiency can cause postneonatal as well as neonatal bleeding,1 ,2 there has been increased interest in the relative efficacy of oral and intramuscular prophylaxis. Countries with a uniform policy have been able to evaluate their practice, but divergent practice3has made any comparable exercise impracticable in most of the UK since 1992.
A uniform policy of oral vitamin K prophylaxis was, however, adopted by 17 of the 18 consultant led maternity units, by the four GP maternity units, and by all the community midwives working in the north of England in 1993. The only other maternity unit adopted a slightly different policy of oral prophylaxis (see below). We now report on the efficacy of these policies in preventing serious vitamin K deficiency bleeding in the first three months of life among all the babies born in the study area between 1993 and 1998 inclusive.
Methods
All babies were to be given 1 mg of an oral preparation of phytomenadione (vitamin K1) at birth. In a small group of babies (those born to mothers receiving warfarin, rifampicin, or anticonvulsant medication, and those not judged to be well enough to be offered milk in the first 12 hours of life) a 0.1 mg/kg dose of intramuscular phytomenadione was recommended immediately after delivery. The oral preparation was Orakay, which contains a medium chain triglyceride obtained from fractionated coconut oil (miglyol 812). The intramuscular preparation was Konakion, which contains phenol, propylene glycol, and polyoxyl 35 castor oil (a non-ionic surfactant). Irrespective of their treatment at birth, it was further recommended that the parents of all breastfed babies should then be given three 1 mg capsules of Orakay, and told to give their baby the contents of one capsule at fortnightly intervals after discharge.
One unit followed a slightly different policy, giving 2 mg (2 drops) of an oral Konakion product at birth, and again at discharge to all babies, whether breastfed or not. This product, which is widely licensed for use in Europe but not in the UK, contains methyl and propyl hydroxybenzoate, benzoic acid and polyoxyl 35 castor oil. Any baby judged not well enough to be offered milk in the first 12 hours of life received 0.1 mg/kg of intramuscular Konakion as in other units. There were 21 679 live births in this unit during the study period. None developed either early or late symptomatic vitamin K deficiency. The births from this unit have been excluded from the findings presented in the remainder of this report.
No attempt was made to impose a uniform strategy as to the way parents were informed of the issues relating to vitamin prophylaxis. Some units gave out written information in the antenatal period while others only raised the issue formally after delivery. Many, but not all, offered written information.
A retrospective audit of special care and postnatal ward case notes in each unit was undertaken to estimate the proportion of babies receiving intramuscular prophylaxis at birth, and to estimate the proportion who failed to receive any prophylaxis. While it was possible to determine, from the case notes, whether the mothers had been prescribed a further supply of vitamin K for use after discharge, this does not guarantee that the family actually received it.
Two parental surveys were undertaken therefore, to establish whether parents had been given a supply of vitamin K at discharge. Parents were also asked, at the same time, whether they understood why prophylaxis was recommended, whether they had any concerns over what they had been advised, and whether they had given the further doses as recommended. A sample of breast feeding mothers were seen and questioned by local health visitors in Northumberland 6–9 weeks after delivery. A second group of mothers from South Cleveland who were breast feeding at discharge were later sent a short attitudinal questionnaire. Both questionnaires approached the issue of compliance obliquely by asking whether the parents had had any problems giving the additional doses as recommended. All paediatricians in the Northern Region were contacted at intervals and asked if they had encountered any possible cases of early or late vitamin K deficiency bleeding. The notes of any cases identified were then reviewed in detail and the case classified using the same internationally agreed criteria as in other epidemiological studies.4 Returns were also cross checked against those that had been made monthly to the British Paediatric Surveillance Unit in 1993–4. No discrepancies were found. All deaths in the first year of life were checked against returns both to the Office of National Statistics and, separately, to the region's long running Survey of Perinatal and Infant Mortality, to make sure that no death that could have been due to vitamin K deficiency bleeding went unrecognised. Significant ascertainment failure due to movement out of the study area can be discounted because other studies have shown that this affects less than 4% of all families in the first two years of life.5 ,6
Results
A total of 193 472 babies were born in the study units between 1993 and 1998 inclusive. Audit of a sample of 1400 case notes found that only about 6% (95% confidence intervals 4.8–7.4%) of babies received intramuscular prophylaxis. There were no cases in the sample where prophylaxis was not prescribed at birth, but the sample contained the notes of two babies (0.1%) whose mothers refused either intramuscular or oral prophylaxis.
None of the estimated 182 000 babies treated with Orakay developed any sign suggestive of vitamin K deficiency bleeding in the first seven days of life. Four documented cases of late vitamin K deficiency bleeding occurred to babies born during this time. All had been fully breastfed. Two of these babies bled despite receiving fortnightly oral prophylaxis and were later found to have α1- antitrypsin deficiency. One was admitted with haematuria, bruising, and continuing low grade jaundice at 25 days; the other was already under investigation for continued jaundice when admitted with irritability and vomiting at 40 days. The following day oozing was seen from venepuncture sites and there were signs of raised intracranial pressure as a result of a posterior fossa bleed. Both babies made a complete recovery, although the second had transient posthaemorrhagic hydrocephalus.
Two otherwise healthy breastfed babies developed late vitamin K deficiency bleeding because unit staff did not give the parents any capsules, nor recommend further prophylaxis, at discharge. One baby, who received only a single prophylactic dose of oral vitamin K at birth, was admitted with blood streaked vomiting at 46 days. A second, who never received any prophylaxis, was admitted with irritability and vomiting at 39 days. Both had seizures within a day of admission. Signs of raised intracranial pressure developed, and scans showed evidence of intracerebral bleeding. Bleeding from venepuncture sites led to hypoprothrombinaemia being diagnosed, which responded promptly to intramuscular vitamin K. The second had also bled during circumcision, but there had been no other “warning bleeds” before admission. One made a complete recovery and the other was making normal developmental progress at 21 months, although there were signs of residual epilepsy.
Seven hundred and fifty breast feeding mothers from one centre were sent a questionnaire, and a further 173 randomly selected breast feeding mothers delivering in any of five centres were approached by health visitors, 6–9 weeks after delivery. Four hundred and fifty eight mothers (61%) responded to the postal survey and all the 173 mothers approached by health visitors responded. All responders in both samples confirmed that they had been given further supplies of vitamin K to administer to their babies. Parents seemed well informed of the reasons for prophylaxis, and happy to have been given the responsibility for giving their baby the recommended vitamin supplement. Although only 61% of the mothers responded to the postal questionnaire, the proportion of those still breast feeding who had given all the further doses, as advised, was the same as in the smaller study where reporting bias was eliminated by getting the health visitor to speak to each family. Data from both studies suggested that 93% of the babies still being breastfed had had all four doses as recommended, and that 98% had had at least three doses.
Discussion
The concern generated by the 1992 report, suggesting that intramuscular vitamin K might be associated with a greater incidence of childhood leukaemia,7 has generated much uncertainty. The Chief Medical Officer made no specific recommendation,8even though guidance on neonatal vitamin needs had been included in earlier departmental reports.9 The former British Paediatric Association decided to recommend the use of a licensed product by an unlicensed route (giving the intramuscular preparation by mouth),10 but the Health Visitors' Association expressed reluctance, on legal advice, to support such a move,11while Roche (the drug company involved) did not apply to license the oral formulation they had on sale in Europe for use in the UK. The Department of Health could have developed a nutritional supplement (similar to the non-commercial multi-vitamin drops that have been available from child health clinics to prevent rickets since 1940),12 ,13 but did not. Roche have since been given a license for a new, concentrated, and more expensive micellar product, suitable for intravenous, intramuscular, or oral use,14but no good, large scale, population based study of this product's ability to prevent late vitamin K deficiency bleeding has yet appeared, and the product only has a license for oral use in babies of 36 weeks of gestation or more.
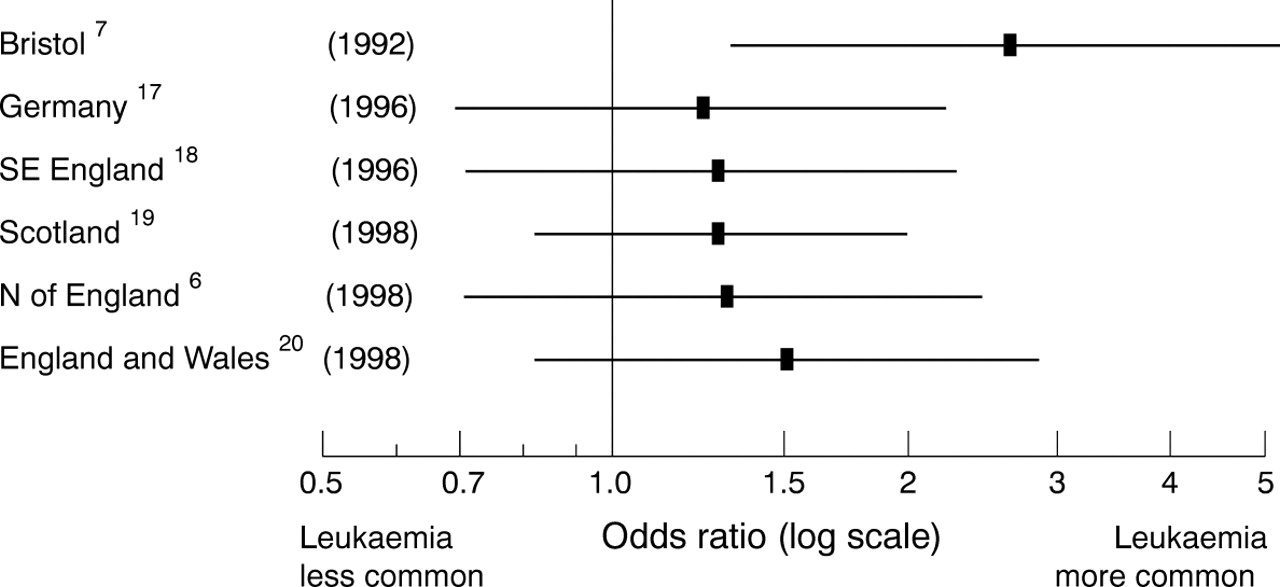
Five replications of the 1992 case control study, suggesting that intramuscular prophylaxis could be carcinogenic,7 have since appeared, but the situation is still unclear,15 and saying that there is no proof of any link is not the same thing as proving that no link exists. While none of the new studies taken in isolation has shown a difference in the incidence of childhood leukaemia that is large enough to be significant, the proportion subsequently developing leukaemia was higher among those given intramuscular vitamin K at birth in all the studies where cases and controls were matched for both date and place of birth. The anonymous expert working party convened by the Department of Health, the Medicines Control Agency, and the Committee on Safety of Medicines in October 1997 concluded that “the findings of epidemiological studies, some of which suggest the possibility of an increased risk [of leukaemia], are inconsistent,”16 but that is not how many will interpret the data. In fact, they all suggest an increased risk (fig 1), and the magnitude of the suggested increase is remarkably consistent.
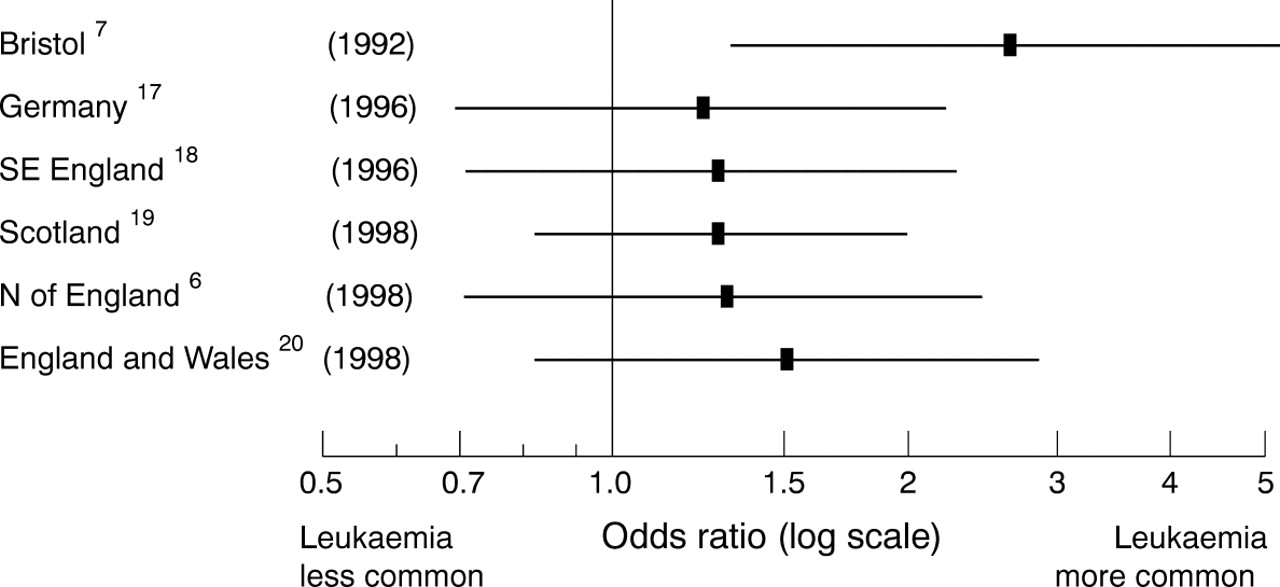
Odds ratios and 95% CI for all cases of leukaemia in children under 15 given intramuscular vitamin K compared with those given no treatment in all six published case–control studies where children have been matched for date and place of birth. The previously unpublished OR for the 148 babies in the North of England study born in units where clear documentation made “imputation” of treatment from a knowledge of hospital policy unnecessary is 1.32 (95% CI: 0.71–2.47).There were 47 discordant case sets.
Unfortunately, no randomised trial was ever attempted before universal prophylaxis became commonplace. Hospitals with a history of selective prophylaxis usually targeted babies having an operative delivery (on the dubious assumption that these were the babies most at risk of “birth trauma”).21 As a result, it is impossible to tell whether the apparent 20–50% increase in the incidence of subsequent leukaemia was actually caused by the treatment given at birth, or whether some other factor, which rendered these babies more liable to operative delivery, also rendered them more liable to develop leukaemia later in childhood.20
The continuing uncertainty will be difficult to resolve: case note destruction makes information on past practice increasingly difficult to obtain,6 ,18 ,20 and few babies born now avoid some form of prophylaxis.3 Furthermore, because childhood cancer is relatively common, while life threatening vitamin K deficiency bleeding is now very rare, even a 10% increase in the incidence of childhood cancer, were it causally related, might result in a policy of universal intramuscular prophylaxis doing more harm than good.20 A randomised trial would be needed to answer this question unequivocally but, to rule out a 10% difference in the incidence of subsequent cancer, it would have to be very large indeed. Many clinicians would, therefore, support a policy of oral prophylaxis if a regimen could be found that abolishes late symptomatic deficiency as effectively as the long established policy of giving all babies intramuscular vitamin K at birth.
Those who first introduced routine prophylaxis 60 years ago gave vitamin K by mouth.22 This route was also endorsed by the American Academy of Pediatrics,23 and encouraged by those who believed that nobody wants an injection on their birthday!24 Indeed it would seem that intramuscular treatment only became the norm in the UK and North America because no commercial company made an oral product available. However, studies have now shown that although a single 1 mg oral dose of the standard preparation at birth is enough to prevent symptomatic deficiency in the first 2 weeks of life, it does little to reduce the incidence of subsequent vitamin K deficiency bleeding (fig 2). Late bleeding is reduced by three 1 mg doses, but is still seen even in some babies without liver disease. Four well spaced doses abolished all symptomatic deficiency in healthy babies in the present study, but was not enough for babies with unrecognised liver disease. A weekly dose does seem to offer complete protection.30 The relative efficacy of the various policies can only be assessed with limited precision because late symptomatic deficiency is only seen in breastfed babies, and the proportion so fed was not the same in each study.

{kind=link}
{kind=link}
Incidence of late vitamin K deficiency bleeding in various population studies, excluding cases where bleeding occurred because prophylactic vitamin K was not given, as recommended, with 95% CI. Konakion was used in all studies except the 1995 Swiss study, where Konakion MM was used, and the current study, where Orakay was used. A small, but poorly defined minority of “ill” babies received intramuscular prophylaxis in all the studies of multidose oral prophylaxis.
Giving a modest oral dose at regular intervals seems more effective than giving just one or two large doses before discharge—an observation consistent with the suggestion that intramuscular prophylaxis may work, not because it bypasses poor intestinal uptake (a problem the new micellar product was designed to address), but because it establishes a slowly released “depot” of vitamin K within muscle tissue.32 Two 2 mg oral doses of the new micellar product are certainly not enough to abolish all risk of late symptomatic deficiency,31 ,33 although further postdischarge doses may achieve this.34 However, because this product is better absorbed when taken by mouth,35 a 2 mg dose produces a transient peak serum concentration similar to that associated with the 1 mg injection and about 100 times the plasma concentration of the vitamin K sufficient adult.36 Policies that require a health care professional to administer every dose have not always worked well in practice,31 ,37 ,38 but devolving responsibility to the parents worked well in the present study. While mothers may have overstated the consistency with which they gave the further oral doses as advised, the only healthy babies for whom the present regional policy failed were the two babies where health professionals, rather than parents, failed to follow local policy guidelines.
A small daily supplement has attractions, and would mimic what happens to the bottle fed baby (because all formula milks are artificially fortified). Late symptomatic vitamin K deficiency is not seen in these babies, and there is no evidence that they are at increased risk of childhood cancer.39 Unfortunately no low dose formulation is currently available in the UK. Daily prophylaxis has worked well in the Netherlands,31 but the 25 μg dose does not seem to be enough for some babies with occult liver disease (fig2).40 Oral prophylaxis is at risk of being discredited41 merely because the dose and, more importantly, dose frequency has not yet been optimised. Maternal prophylaxis during breast feeding provides an alternative, rather more complex, strategy.42-44
Certainly, if there is to be any genuine commitment to the prevention of vitamin K deficiency bleeding, and to offering families genuine choice, hospitals need to make sustained oral prophylaxis available, and like intramuscular prophylaxis, it should also be free of charge.
Acknowledgments
We are grateful to our colleagues in the Northern Neonatal Network for their collaboration , without which this study would not have been possible, to Drs McNinch and Tripp, and the British Paediatric Surveillance Unit for cross validating the reported episodes of vitamin K deficiency bleeding in 1993 and 1994, to Dr Nørgaard Hansen for information on symptomatic vitamin K deficiency bleeding in Denmark30 in 1996–8, and to Dr Laughnan and the Australian Paediatric Surveillance Unit for information from the study of all births in Victoria and New South Wales in 1993–98 which modifies and augments the information published in 1997.31Deborah Magor set up the postal study designed to assess attitudes to oral prophylaxis while working as a student pharmacy technician in Middlesbrough. Health visitors in Northumberland made the other parental interview study possible.