Article Text

Abstract
AIM To examine the reproducibility of crown–heel length measurement; the precision and reproducibility of knee–heel length measurement; and the association between the two in healthy preterm infants.
METHODS Paired crown–heel and knee–heel lengths were measured on 172 occasions by three observers in 43 preterm infants between 205 and 458 days of postconceptional age.
RESULTS Crown–heel length (CHL) measurement was highly reproducible, with a coefficient of variation (CV) of 0.41%. Knee–heel length (KHL) measurement was relatively precise (CV 0.78%), but less reproducible (intra-observer CV 1.77%, intra-observer CV 2.11%), especially in larger infants. The association between KHL and CHL was not consistent and varied with age. KHL was a poor predictor of CHL, with a 95% predictive interval of ± 27.5 mm.
CONCLUSIONS KHL was less reproducible than CHL, especially in larger infants, and a poor predictor of CHL.
- crown–heel length
- knee–heel length
- knemometry
- linear growth
Statistics from Altmetric.com
Accurate assessment of growth is an important component of the care of preterm infants. The most commonly used measures of growth in preterm infants are weight and head circumference, but these have limitations. Weight measurements can be significantly affected by changes in hydration,1 and give little information on the compositional nature of growth.2 Weight gain may continue during periods of nutritional inadequacy at the expense of body composition.3 Although head circumference is a generally good measure of brain growth,3 it is confounded by the effect of “brain sparing” during nutritional stress,4the dolichocephalic head shape seen in preterm infants.5
Measurement of linear growth is considered to be the best indicator of dietary adequacy and it most closely relates to lean body mass.1 6 Linear growth in preterm infants is usually assessed by measuring crown–heel length. This is the most common, and often the only, measure of linear growth in interventional studies in preterm infants. Although crown–heel length can be measured early in the neonatal period,7 it can be difficult. It involves considerable handling of the infant, which may be poorly tolerated, and the risk of endotracheal tube or intravenous catheter displacement. Other measures of linear growth in preterm infants, such as foot length,8 elbow–wrist length,9 10 or knee–heel length have therefore been investigated. Knee–heel length can be measured precisely and reproducibly using Vernier calipers,9-11 or various electronic knemometers.12-14 Although “one assumption that must be made in knemometry is that growth of the isolated limb is representative of growth of the whole body,”13 no data are currently available which compare knee–heel length and crown–heel length in preterm infants, but the need to compare changes in knee–heel length and total body length has been noted elsewhere.11
This study aimed to examine the precision and reproducibility of knee–heel length measurements, and to compare knee–heel length and crown–heel length in growing preterm infants over a wide age range; and to test the hypothesis that knee–heel length is a precise and reproducible measure and an accurate reflection of total body length (crown–heel length).
Methods
Preterm (gestational age <244 days), low birthweight (<1750 g) babies were recruited on the special care baby unit and the neonatal follow up clinic of the Royal Victoria Infirmary, Newcastle-upon-Tyne. Paired measurements of crown–heel and knee–heel length were made during the initial hospital stay, and up to 6 months of corrected age. The study received local ethical approval from the Newcastle and Northumbria Health Authorities Joint Ethics Committee, and informed parental consent was obtained. All infants were clinically stable and had normal weight gain (>15 g/day). No infants received corticosteroids or diuretics during or within two weeks of the start of the study.
CROWN–HEEL LENGTH MEASUREMENT TECHNIQUE
Crown–heel length was measured, as described before.15-16 The naked infant was placed supine on a preterm infant length board (Ellard Instruments, Seattle, WA.). One observer gently held the infant against the fixed head board so that the eyes faced directly upwards, and the lower margin of the orbit was in the same vertical plane as the external auditory meatus. A second observer gently pressed the infant’s knees down, and held the feet vertically, at 90° to the length board. This observer then moved the foot board against the infant’s sole, with just sufficient pressure to cause the soles to blanch. The length (to the nearest millimetre) was noted, but not revealed. The two observers changed positions and the procedure was repeated. If the two readings agreed to within 2 mm the average was taken (rounded up to the next millimetre), otherwise the procedure was repeated until sufficient agreement was reached.
KNEE–HEEL LENGTH MEASUREMENT TECHNIQUE
Knee–heel length was measured using a neonatal knemometer (Force Institute, Copenhagen, Denmark) which is an electronic caliper with one fixed and one movable arm, with a measurement resolution of 0.01 mm.17
The infant’s right knee was placed in the fixed arm of the caliper and the knee and ankle were gently flexed at an angle of 90°, so that the lower leg was parallel to the body of the knemometer. The movable arm was advanced against the foot until a pre-set pressure was reached and the reading transferred to a printer out of sight of the observer. The movable arm was withdrawn from the foot then re-advanced and a further reading taken. A series of eight readings was made by each observer. The first three readings in a series were discarded, and the remaining five averaged to produce a final measurement, as described before.13 The knemometer was then removed and passed to a second observer who made a series of eight readings. Finally, the first observer took a further series of eight readings. In each case the final recorded measurement of knee–heel length was the average of the last five readings in a series.
Intra-observer reproducibility was estimated from the difference between the first and third measurements (which were made by the same observer). Interobserver variability was calculated from the difference between the first and second measurements (which were made by different observers).
REPRODUCIBILITY OF CROWN–HEEL LENGTH MEASUREMENT
Reproducibility was estimated for 50 consecutive measurements made on similar subjects, and by the same observers, as described above, using the method of Bland and Altman.18 The difference between the estimate of crown–heel length made by the first and second observer was calculated and plotted against the mean of the two estimates. The mean (x) and standard deviation (SD) of the differences were calculated, and used to estimate bias and reproducibility, respectively. The 95% confidence interval, which describes the range which includes duplicate measurements 95% of the time, is given by the interval between (x +1.96 SD) and (x −1.96SD). If there is no systematic difference (bias) between the first and second estimate the mean difference will not be significantly different from zero, and the 95% confidence interval reduces to ±1.96 SD. The coefficient of variation (CV) was calculated from the ratio of the SD of the differences, to the mean crown–heel length.
PRECISION OF KNEE–HEEL LENGTH MEASUREMENTS
The last five readings in a series were averaged to produce the final measurement, and the SD of these five readings was calculated as an estimate of measurement precision.19
The effect of infant’s size and age on measurement precision was assessed by comparing the SD for the lowest and highest weight quartiles, and youngest and oldest postconceptional age quartiles. The effect of learning was assessed by comparing the SD for the first and last 50 measurements made.
The five readings that were averaged to produce the final measurement were regressed against their order in the series (1 to 5) to see if there was an order of measurement effect.
REPRODUCIBILITY OF KNEE–HEEL LENGTH MEASUREMENTS.
The reproducibility of knee–heel length measurements was assessed using the SD of the differences, as described previously for crown–heel length. To assess intra-observer reproducibility, the difference between the first and second measurement made by a single observer at any given time was calculated. To assess inter-observer reproducibility, the difference between measurements made by different observers was calculated.
The different measurements made at any one time were regressed against their order (1, 2, or 3) to see if there was any order of measurement effect.
The effect of infant’s size and age was assessed, as described above. The effect of learning was assessed by comparing the reproducibility of the first and last 25 measurements.
RELATION BETWEEN CROWN–HEEL AND KNEE–HEEL LENGTH
Crown–heel length and knee–heel length were compared by simple regression analysis. The SD of the crown–heel length residuals was calculated. The 95% predictive interval (± 1.96 multiples of the SD) was calculated. For any given knee–heel length there is a 95% chance that the true crown–heel length lies within this range. The ratio of knee–heel to crown–heel length was calculated and the change in this ratio with increasing postconceptional age was assessed by regression analysis.
Incremental changes in crown–heel and knee–heel length were assessed by calculating length velocities for all subjects with sequential measurements, at least 10 days apart:
Only the first measurement of knee–heel length made by the most experienced observer (NP) was used in this part of the analysis.
Statistical analysis was carried out using the statistical package StatView version 4.51 (Abacus Concepts, Berkeley, CA.). Results were considered significant at a level of p < 0.05. Ninety five per cent confidence intervals were expressed as absolute values (mm), and in multiples of the average growth rate.
Results
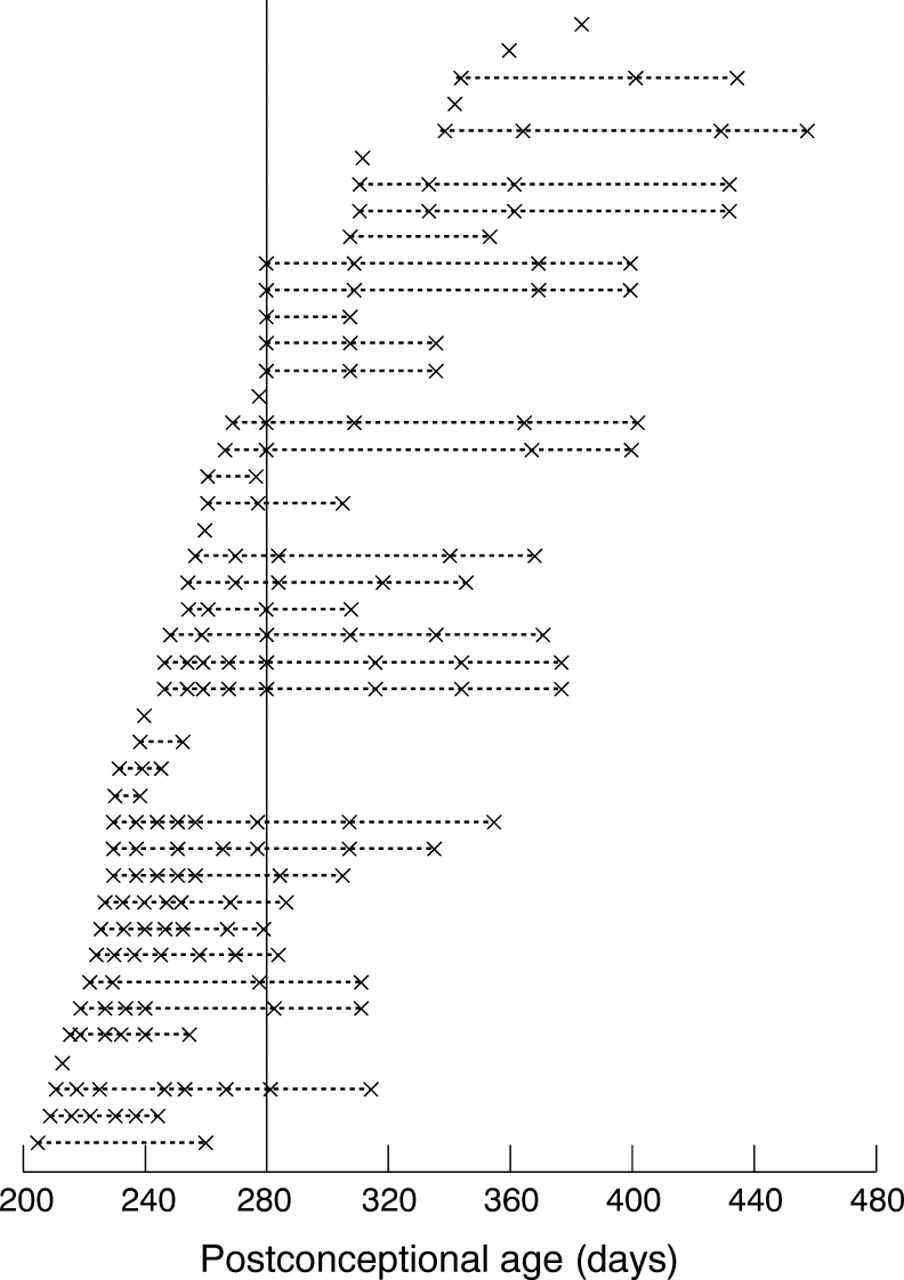
Paired measurements of knee–heel and crown–heel length were made in 43 subjects (19 boys, 24 girls) of mean birthweight 1.37 kg (SD 0.24) and mean gestational age 214 days (SD 13). The infants were studied on 172 occasions and a total of 429 knee–heel length measurements were made by three observers: NP (n=238), IG (n=128), and JP (n=63). Measurements were made at a mean of 285 days postconceptional age (range 205–458 days), and at a mean weight of 3.20 kg (range 0.99–8.26 kg). Each infant was studied on a median of four separate occasions (range 1–8) (fig 1).

Representation of the 43 infants studied. Each line represents one infant; crosses indicate times at which CHL and KHL were measured. Solid vertical line represents expected date of delivery (280 days of postconceptional age).
Knee–heel length increased as an approximately linear function of postconceptional age (y = 28 + 0.33 x, r = +0.92; p value < 0.0001), at a rate of 0.33 mm/day. Crown–heel length increased similarly (y = 156 + 1.14 x, r = +0.95; p value < 0.0001), at a rate of 1.14 mm/day.
REPRODUCIBILITY OF MEASUREMENTS
Crown–heel
Fifty subjects were studied, of mean birthweight 1.38 kg (SD 0.31) and mean gestational age 214 days (SD 14). The mean weight at the time of measurement was 4.91 kg (SD 0.20, range 1.79–8.97) and the mean postconceptional age was 349 days (SD 72, range 254–465).
The absolute difference between the value obtained by the two observers ranged from 0 mm to 8 mm, with a median of 1 mm. The SD of the differences was 2.28 mm (CV 0.41%), with 95% confidence interval of ± 4.47 mm or ± 3.9 days of crown–heel length growth.
Knee–heel length measurements
When more than one measurement of knee–heel length was made at a given time, no trend was seen between successive measurements (p = 0.59).
Bland–Altman plots of intra-observer reproducibility for NP, and interobserver reproducibility between NP and IG, and between NP and JP, are shown in fig 2. In no case did the mean difference between observers differ significantly from zero, showing that there was no systematic bias between different observers.
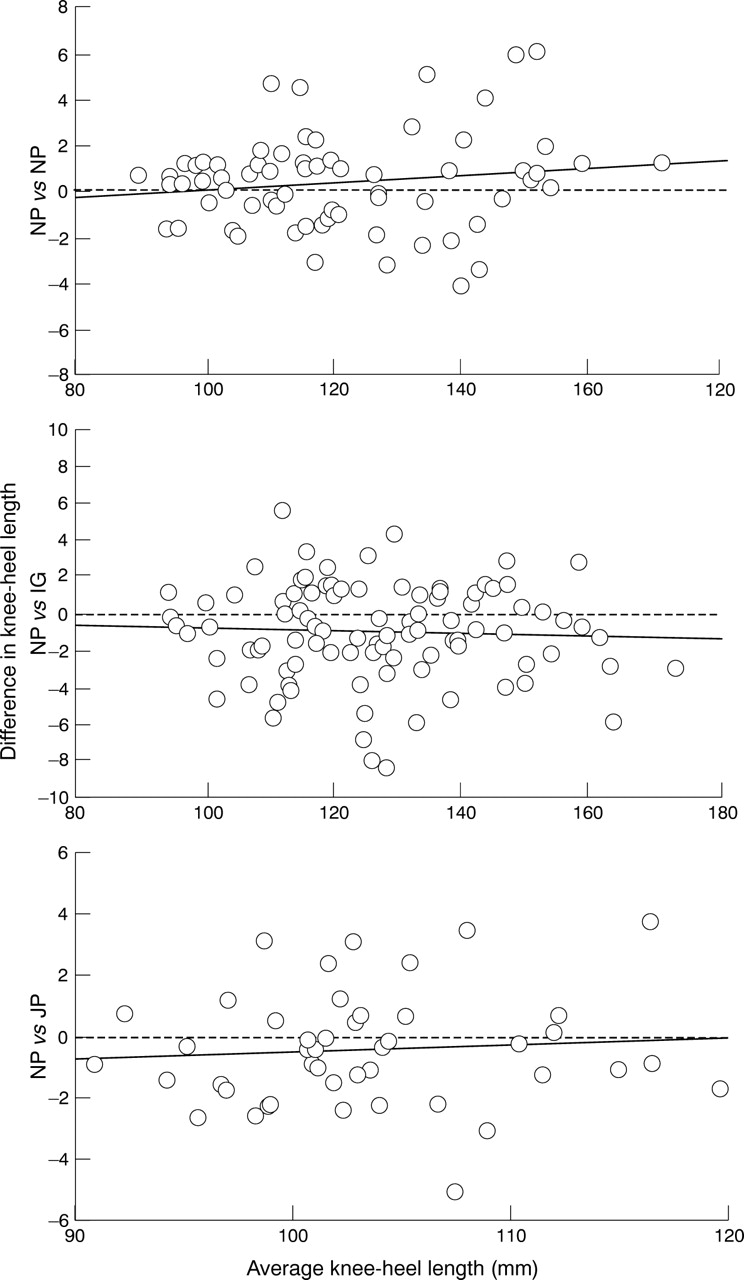
Representative Bland–Altman plots for intra- and interobserver reproducibility. Upper panel shows intra-observer reproducibility for observer NP; middle panel interobserver reproducibility between NP and IG; lower panel interobserver reproducibility between NP and JP.
Intra-observer reproducibility was assessed in 115 instances. The SD was 2.13 mm (CV 1.77%) and was similar for the three observers (NP n=70, CV 1.46%; IG n=27, CV 1.69%; JP n=18, CV 1.92%). The average 95% confidence interval was ± 4.18 mm (± 12.7 days knee–heel length growth).
The SD of the differences was similar for the first 25 measurements made by NP (1.85 mm, CV 1.66%) and the last 25 (2.10 mm, CV 1.65%). Reproducibility was poorer in the heaviest quartile (weight >4.3 kg, SD 2.71 mm, CV 1.03%) than for the lightest quartile (weight 1.75 kg, SD 1.02 mm, CV 1.82%), and for the oldest age quartile (postconceptional age 309 days, SD 2.48 mm, CV 1.68%) than for the youngest age quartile (postconceptional age 239 days, SD 1.07 mm, CV 1.08%).
The interobserver reproducibility was assessed in 166 instances. The SD of the differences was 2.57 mm (CV 2.18%) and was similar for all pairs of observers, varying from a coefficient of variation of 2.05% to 2.11%. The 95% confidence interval was ± 5.03 mm or ± 15.2 days knee–heel growth.
Precision of knee–heel length measurements
When the five readings used to calculate a measurement were regressed against their order in the series (3 to 8), no trend was seen (p = 0.76).
The average SD of the five readings used to estimate knee–heel length was 0.95 mm (CV 0.79%). The CV ranged from 0.43% to 1.07% for different observers.
The most experienced observer (NP) made 238 measurements of knee–heel length. Precision was 0.36 mm in the lowest weight quartile (weight <1.825 kg), and 1.24 mm in the highest weight quartile (weight >4.5 kg). In the youngest age quartile (postconceptional age <240 days) the precision was 0.34 mm, and 1.19 in the oldest age quartile (postconceptional age >311 days). Precision also improved with experience, with the SD falling from 1.33 mm for the first 50 measurements to 0.76 for the last 50 measurements.
Relation between crown–heel and knee–heel length
The relation between knee–heel length and crown–heel length is shown in fig 3. The two were significantly related (r = +0.98, p <0.001). The residuals around the line were normally distributed with a mean (SD) of 0.0 (14.0) mm. The 95% predictive interval is ± 27.5 mm or ± 24.1 days crown–heel length growth.

Scattergram of knee–heel length against crown–heel length. Solid line represents line of best fit (y = 78.73 = 3.30x; R2 = 0.96); two dotted lines show 95% CI, ± 27.48 mm around line of best fit.
The ratio of knee–heel length to crown–heel length averaged 0.25 (SD 0.1), but varied with postconceptional age, as shown in fig 4.
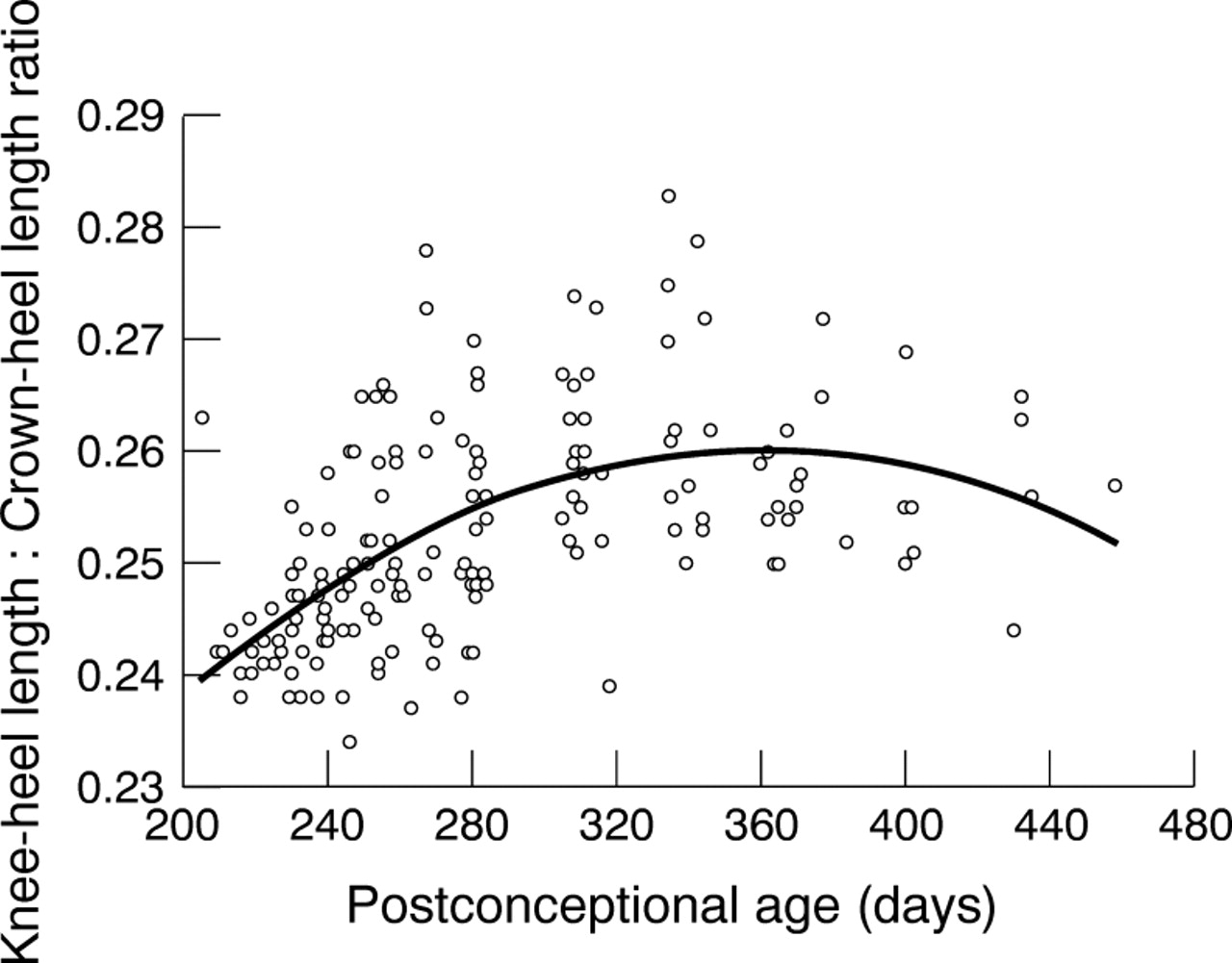
Scattergram of knee–heel:crown–heel length ratio against postconceptional age. Solid line represents line of best fit (y=0.15 + 6.2E-4 x − 8.6E-7x2; R2 = 0.32).
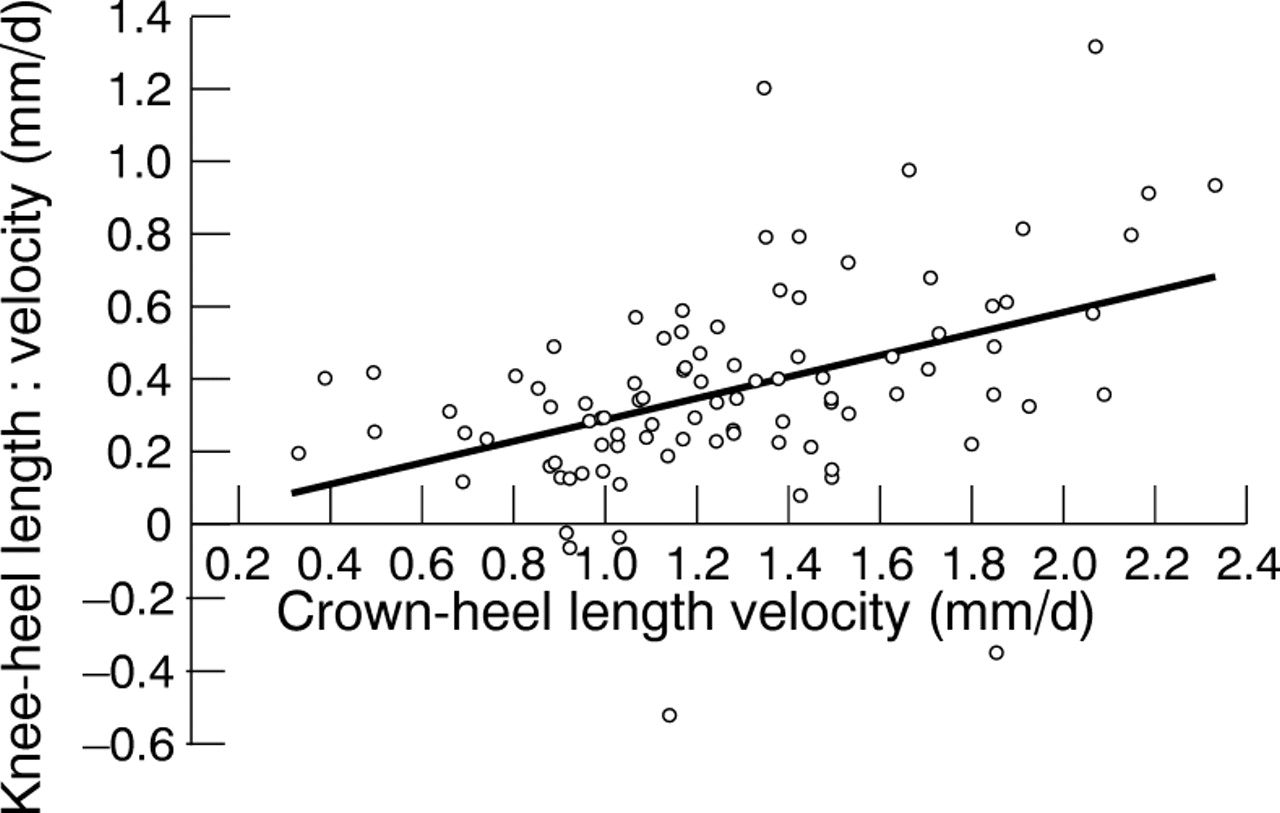
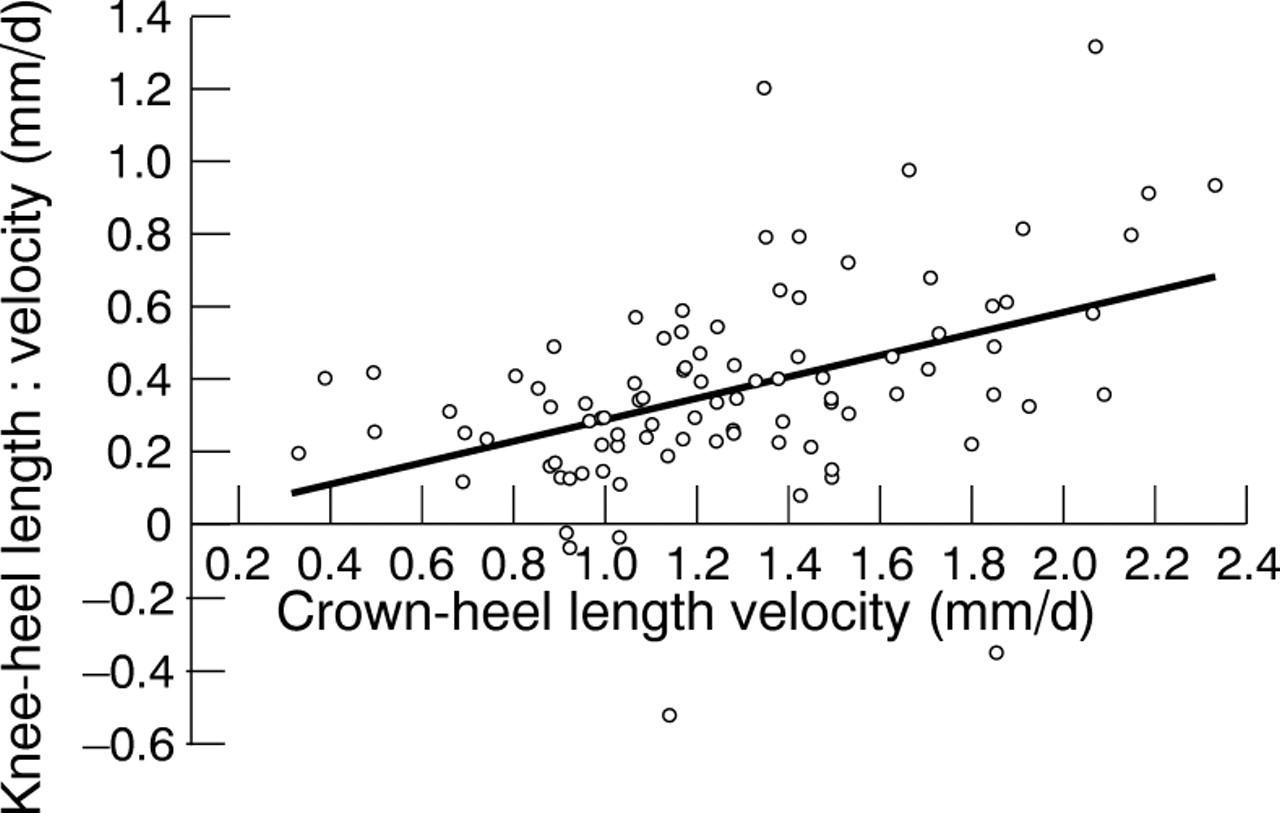
Crown–heel and knee–heel length velocity were calculated in 94 instances in 34 subjects. The average time period over which velocity was calculated was 16.5 days (SD 1.7), with a range of 12 to 89 days (median 26). Fig 5 shows the highly significant correlation (p < 0.001) between knee–heel and crown–heel length velocity. In five instances knee–heel length velocity was negative, but in no cases was crown–heel length velocity negative
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Scattergram of knee–heel length velocity against crown–heel length velocity. Solid line represents line of best fit (y = 0.294 x −0.006, R2 = 0.201).
Discussion
Measurement of crown–heel length remains the gold standard measure of linear growth in preterm infants, and in this study was highly reproducible, with a coefficient of variation of only 0.41%. This is only slightly higher than that reported for height measurements in older children,19 and similar to previously published data for length measurement in infants.13 16
Two previous studies have used electronic knemometers to estimate measurement precision. Michaelsen et al 17 quote an average SD of 0.82 mm, while Gibsonet al 13 found values of 0.59 mm at the beginning, and 0.34 mm at the end, of their study. In our study the average SD of the five readings was 0.94 mm. However, both previous studies only examined smaller infants, while we studied a wide range of subjects. We found that precision was much better in younger (SD 0.31 mm), smaller infants (SD 0.34 mm), and comparable with the best values quoted by Gibson et al.13 The poorer precision in larger infants probably reflects the increased difficulty of maintaining the leg in a constant position during the measurement process, due to the larger size of the leg and increased activity of the infant. We, like others,13 saw a significant learning effect, with precision improving with time from an average SD of 1.73 mm to 0.88 mm.
One study examined the reproducibility of knemometry in preterm infants, quoting an intra-observer variation from 0.34% to 0.48%, and interobserver variation for different observers ranging from −4.8% to +3.6%.13 In our study the intra-observer coefficient of variation was 1.77%, and interobserver coefficient of variation 2.18%. Again, comparison between studies is difficult because of differences in the patient populations, as we found reproducibility was better in smaller infants. Unlike other investigators,11 13 we found no systematic differences between observers.
The 95% confidence interval for crown–heel length measurement was equal to ± 3.9 days crown–heel length growth. This is more reproducible than knee–heel length measurement with values of ± 12.7 days and ± 15.2 days knee–heel length growth (for intra- and interobserver reproducibility, respectively). Even in the youngest quartile of infants intra-observer 95% confidence interval for knee–heel length was ± 6.1 days of growth. In our hands, therefore, crown–heel length measurement was more reproducible than knee–heel length.
The principal aim of our study was to compare knee–heel and crown–heel lengths in preterm infants. James et al 8 showed an excellent statistical correlation between foot length and crown–heel length, with a 95% confidence interval for crown–heel length of ± 2.5 cm. This is very similar to the result in our study: 95% predictive intervals of ± 27.5 mm. Although the statistical correlation for the population as a whole is good, the 95% predictive interval is equivalent to ± 24.1 days crown–heel length growth. Knee–heel length is, therefore, poorly predictive of crown–heel length in this population.
Crown–heel and knee–heel length velocities were highly statistically correlated (p < 0.0001), but again the scatter around the line of best fit is too great to be clinically useful. In five instances calculated knee–heel length velocity was negative, but crown–heel length velocity was positive. Negative growth does occur during acute illnesses in children,20 and during dexamethasone treatment in preterm infants,21 but our study population was healthy and not receiving steroids. The negative knee–heel length velocities in these infants did not, we believe, reflect a truly negative linear growth, as crown–heel length velocity was positive. Instead, they may be explained by the poor precision of knee–heel length measurement. This was not unexpected as small errors in measurements are compounded when incremental (velocity) data are calculated.16 This problem is worsened if the measurement technique is poorly reproducible, or if velocities are calculated over a short time period.16
Brooke et al measured crown–heel and knee–heel lengths in infants born at term.22 They found the mean knee–heel length at 40 weeks gestation was 12.3 cm (SD 0.5) for boys and 12.1 cm (SD 0.5) for girls, comparable with the data in our study (12.0 cm). However, in our study mean crown–heel length at 40 weeks gestation was 47.5 cm, lower than Brooke’s data for comparable males (51.0 cm, SD 1.8) and girls (50.1 cm, SD 1.7).22 If knee–heel length had been the only measure of linear growth used we could have assumed that this population of preterm infants had largely “caught-up” with term infants by their expected date of delivery. However, as crown–heel length measurements show, linear growth in our subjects was significantly poorer than infants born at term. Catch-up growth in knee–heel length might have occurred earlier than in crown–heel length. Although this may lead to an overestimate of the degree of catch-up, it also raises the possibility that knee–heel length measurement may be a more sensitive indicator of the early stages of catch-up growth than is crown–heel length. Further studies are needed to examine this.
The relation between knee–heel length and crown–heel length changed with postconceptional age, and axial growth (knee–heel length) made a variable contribution to total linear growth (crown–heel length).
In summary we found that knee–heel length is less reproducible than previously described, especially in larger infants, and less reproducible than crown–heel length measurement. The relation between knee–heel and crown–heel length varies as a function of postconceptional age, and knee–heel length is a poor predictor of crown–heel length.
Although knee–heel length does not accurately reflect crown–heel length, it may be a useful research tool in preterm infants if it can be shown to accurately reflect lean body mass, or other estimates of nutritional adequacy. Its use in the clinical setting, however, seems to be limited.
Acknowledgments
We thank Dr E O’Brian Smith (Children’s Nutrition Research Center, Baylor College of Medicine/ Texas Children’s Hospital, Houston, Texas) for advice on the statistical analysis. We also thank Dr Alan C Fenton, Dr Kenneth PB McCormick (Special Care Unit, Royal Victoria Infirmary, Newcastle-upon-Tyne) for critically reviewing this manuscript; and Marjorie Henderson and Jacqui Smith for their help with data collection.