Article Text

Abstract
AIM To investigate the diagnostic potential of herpes simplex virus (HSV) DNA in cerebrospinal fluid and serum; to correlate the findings with outcome in the child and with type of maternal infection.
METHODS Cerebrospinal fluid and serum specimens from 36 children with verified neonatal HSV infections, diagnosed between 1973 and 1996, were examined using the polymerase chain reaction technique (PCR).
RESULTS In 21 children for whom both cerebrospinal fluid and sera were available, HSV DNA was found in one or both specimens in 19 (90%). Overall, HSV DNA was found in the cerebrospinal fluid of 74% of 27 children, and in the sera of 20 out of 30 children (67%). In two children HSV DNA was not demonstrable in either serum or cerebrospinal fluid. In sequential specimens from four children, the persistence of HSV DNA after the end of intravenous treatment was associated with a poor prognosis.
CONCLUSIONS These findings indicate that HSV DNA detection in CSF and serum is highly sensitive for the diagnosis of neonatal HSV infections but does not replace the detection of virus in other locations using virus isolation and antigen detection.
- HSV DNA
- herpes simplex virus infections
- PCR
Statistics from Altmetric.com
Early recognition and treatment of neonatal herpes simplex virus infection are important to reduce the mortality and incidence of serious neurological sequelae in surviving children.1 The polymerase chain reaction technique (PCR), used to detect herpes simplex virus DNA in cerebrospinal fluid (CSF), has greatly contributed to rapid non-invasive diagnosis, particularly of HSV infections in the central nervous system of both adults and neonates. However, the diagnostic sensitivity of PCR analysis seems to be lower in neonatal herpes encephalitis2 than in adults,3 4emphasising the importance of additional diagnostic tools for the diagnosis of neonatal herpes. In this study, stored CSF and sera from children with previously verified diagnoses of neonatal herpes simplex virus infections were analysed retrospectively using highly sensitive nested PCR techniques for HSV-1/HSV-2 DNA. The results were correlated with the patients’ clinical data and with the type of maternal infection.
Methods
CSF and/or sera from 36 children with neonatal herpes infection diagnosed during 1973–96, were stored frozen and analysed for the presence of herpes simplex virus (HSV) DNA using the PCR technique. HSV infection was confirmed, as described before5 by viral antigen detection (immunofluorescence with HSV monoclonal antibodies) and/or cultivation of virus in GMK-AHI-cells; and/or serologically using enzyme linked immunoabsorbent assay (ELISA) technique for IgM/IgA/IgG class antibody response and persistence of herpes simplex virus antibodies common to the two types (type common) as well as type 2 specific glycoprotein G antigen.
The classification of the neonatal disease followed the criteria of the US multicentre study2: disseminated disease with generalised visceral involvement; central nervous system disease (CSF characterised by > 50 × 106 leucocytes and/or 1.2 g/l protein in premature babies and 20 × 106 leucocytes and/or 0.9 g/l protein in full term babies) and clinical signs of central nervous system—but no visceral—involvement; localised skin–eye–mouth disease (SEM) without visceral or central nervous system involvement.
Head ultrasound scan, and/or computed tomography (CT), and/or magnetic resonance imaging (MRI) were performed on 27 children from day 1 and/or later, once or several times, after initial clinical symptoms and at follow up. In one child only head ultrasound scanning was done. A wide range of central nervous system lesions was detected, such as ventricular enlargement, cerebral atrophy, cystic encephalomalaci and focal parenchymal lesions, in both cerebral hemispheres or predominantly in one. These are defined as abnormal CT/MRI/HUS in table1.
Virological, clinical, and neuroradiological data in 36 children with neonatal HSV infections
Twenty seven children were treated with intravenous aciclovir (range 4 to 22 days). Nine children were not treated (table 1).
At follow up, severe mental retardation was defined as an IQ <50, mild mental retardation (MMR) as an IQ of 50–70.5
Maternal infections were classified according to results obtained by analysis of sera sampled before or during early pregnancy, and those from onset of disease in their children: no infection in the mother (child infected from external source); primary HSV-1 or HSV-2 infection without previous HSV infection with either type; first time HSV-2 infection in a woman previously infected with HSV-1; secondary (previous infection with the same HSV type—recurrent or re-infection) HSV-1 or HSV-2 infection.6
Specimens of CSF (n=63) and sera (n=56) from 36 children were analysed using HSV-1 and HSV-2 specific PCR. Cerebrospinal fluid and serum during the acute stage of the disease were sampled from 21 children; CSF only from another six children and serum only from a further nine children. One or more follow up CSF specimens were available for analysis from 17 children.
Cerebrospinal fluid and serm samples were analysed using the nested PCR technique for HSV-1 and HSV-2 specific DNA with primers in the gD and gG2 gene, as described before,3 with minor modifications.7 The sensitivity of the test ensures the regular detection of 10–15 copies per 10 μl. Uncentrifuged cerebrospinal fluid was frozen and thawed at least once and heated for 10 minutes at 95°C before the PCR mix was added; 10 μl were analysed in duplicate. Serum samples of 50 μl were extracted using the glycogen–guanidium method, according to Casaset al. 8 Concordant results in duplicate analysis were taken as final. Equivocal results were verified by repeat analysis and positive results were confirmed in all cases. To increase the sensitivity of HSV DNA analysis, ⩾50 μl CSF was extracted according to the same procedure, the prepared DNA was suspended in 25 μl and reanalysed, as described before. However, retesting of two initially HSV DNA negative specimens from early stage disease still yielded negative results. Cerebrospinal fluid or serum inhibiting activity was tested by spiking a duplicate sample with around 50 HSV DNA copies before analysis. The type of HSV DNA coincided in all cases with the type of HSV isolated and/or the results of type specific serodiagnosis.
Results
Seven children had HSV-1 and 29 HSV-2 infection. Neonatal disease was classified as disseminated in six children, SEM in one, and central nervous system form in 29. One child with disseminated infection had congenital infection, and was born at 29 weeks of gestational age with vesicles all over the body at birth. Frontal lesions were detectable in the brain on ultrasound scan two days later. The incubation time in the other 35 children ranged from two to 44 days. Fourteen women had primary transmissible HSV infections. Eight had had no previous infection with either herpes virus type: three women had primary HSV-1, five HSV-2, six primary HSV-2 but with a previous HSV-1. Twenty women had secondary infection—they had been infected with the same type of HSV and may have had a recurrence or re-infection. Two of the 36 children had contracted their HSV-1 infection from an external source: the mothers were seronegative for HSV-1 and HSV-2 and remained so at follow up (table 1).
Six of the seven children with HSV-1 infections were normally developed at follow up (age range 1 to 14 years), although one had recurrent keratitis. The seventh child had mild mental retardation (IQ < 70). Four children with HSV-2 infections died between the ages of 1 week and 4 years. Eighteen children (age range and 1.5–18 years) were neurologically impaired: 11 had spastic tetraplegia and severe mental retardation, one had a spastic diplegia, and six had spastic hemiplegia, of whom one was also mildly mentally retarded. Seven children were normally developed at follow up (range 1–8 years); two of them had recurrent keratitis (table 1). Twenty children had regular reactivation of vesicles in skin; some of them had not had neonatal vesicular disease.
Virological diagnosis was confirmed in all children by isolation of virus, or by serological investigations, or both. At ages 1 to 15 years all children had persistent HSV specific antibodies, regardless of whether antiviral treatment was given during the acute phase of the disease. Antibodies specific for HSV-2 were not demonstrable in any child with neonatal herpesvirus type 1 infection, but in all type 2 infected children. However, the antibody response may be suppressed during long term oral aciclovir treatment as seen in case 29 (table 1). This child had clinical symptoms of encephalitis at 17 days of age and pleocytosis in the cerebrospinal fluid. HSV-2 DNA was demonstrable in cerebrospinal fluid the first day of symptoms, HSV-2 virus was isolated from the nasopharynx. Prominent lesions were subsequently seen on computed tomography and MRI and the boy has severe neurological impairment. He had been treated with intravenous aciclovir for three weeks and long term oral suppression was given for 2 years. His HSV antibody response (type common and type 2 specific) was not demonstrable until 4 years of age, when he had recurrent vesicles on his arm, from which HSV-2 was isolated.
POSITIVE PCR FINDINGS
Nineteen of 21 (90%) children (20 central nervous system form and one disseminated) with both acute stage CSF and serum available for analysis, had a positive PCR in one or both specimens. In the CSF available from 27 children in the acute stage of the disease, HSV DNA was demonstrable in 20 (74%). Virus isolation had been successful only in nine of 27 (33%) of such cases. If sera alone were analysed, HSV DNA was demonstrable in 20 of 30 available specimens (67%).
NEGATIVE PCR FINDINGS
In children with central nervous system disease HSV-DNA was demonstrable in acute stage cerebrospinal fluid in 18 of 23 (78%) (table 1).
Acute stage cerebrospinal fluid from two children with HSV-2 encephalitis, one with, and the other without, long term central nervous system sequelae, but with recurrent keratitis, were negative (cases 20 and 24) (table 1), but re-analyses were not possible. They received their aciclovir treatment the day cerebrospinal fluid specimens had been collected, five and four days after first symptoms, respectively. In two other children (cases 15 and 16), the amount of acute phase cerebrospinal fluid was sufficient for re-analyses, and HSV DNA remained negative in repeat analyses using PCR with increased sensitivity, and no inhibitory activity to the PCR was observed. Sera from these two children were also negative by PCR. In these cases both cerebrospinal fluid and sera were collected at days 6 and 5, respectively, after onset of symptoms in the infants. Case 15, born at term, had neonatal meningitis and received her aciclovir treatment the day cerebrospinal fluid was collected. She had skin vesicles and 43 × 106 leucocytes in cerebrospinal fluid, but no convulsions and a normal EEG (head ultrasound scan and computed tomography were not performed). The diagnosis was obtained by virus isolation of HSV-2, although not from the cerebrospinal fluid, and was later confirmed serologically. She was normally developed at 7 years of age, but still had recurrent vesicles. Case 16, who received intravenous aciclovir treatment two days after CSF had been collected, had neonatal encephalitis with vesicles, convulsions, 216 × 106leucocytes in cerebrospinal fluid, abnormal EEG, and prominent lesions on computed tomography scan. She developed severe neurological impairment with microcephaly, mental retardation, spastic tetraplegia and had recurrent vesicles at follow up when 11 years old. The fifth child (case 4) with negative PCR in cerebrospinal fluid had neonatal meningitis as a result of HSV-1 infection, and was healthy at follow up when 7 years old, but had recurrent vesicles. She received her antiviral treatment the same day as cerebrospinal fluid was collected, five days after initial symptoms. Case 10, with a rapidly fatal disseminated disease, born to a primary infected mother, had a negative PCR in cerebrospinal fluid the first day of the disease. A second specimen could not be obtained. The boy with congenital disease (case 12) had a negative PCR in cerebrospinal fluid, collected 13 days after birth and nine days after treatment had begun.
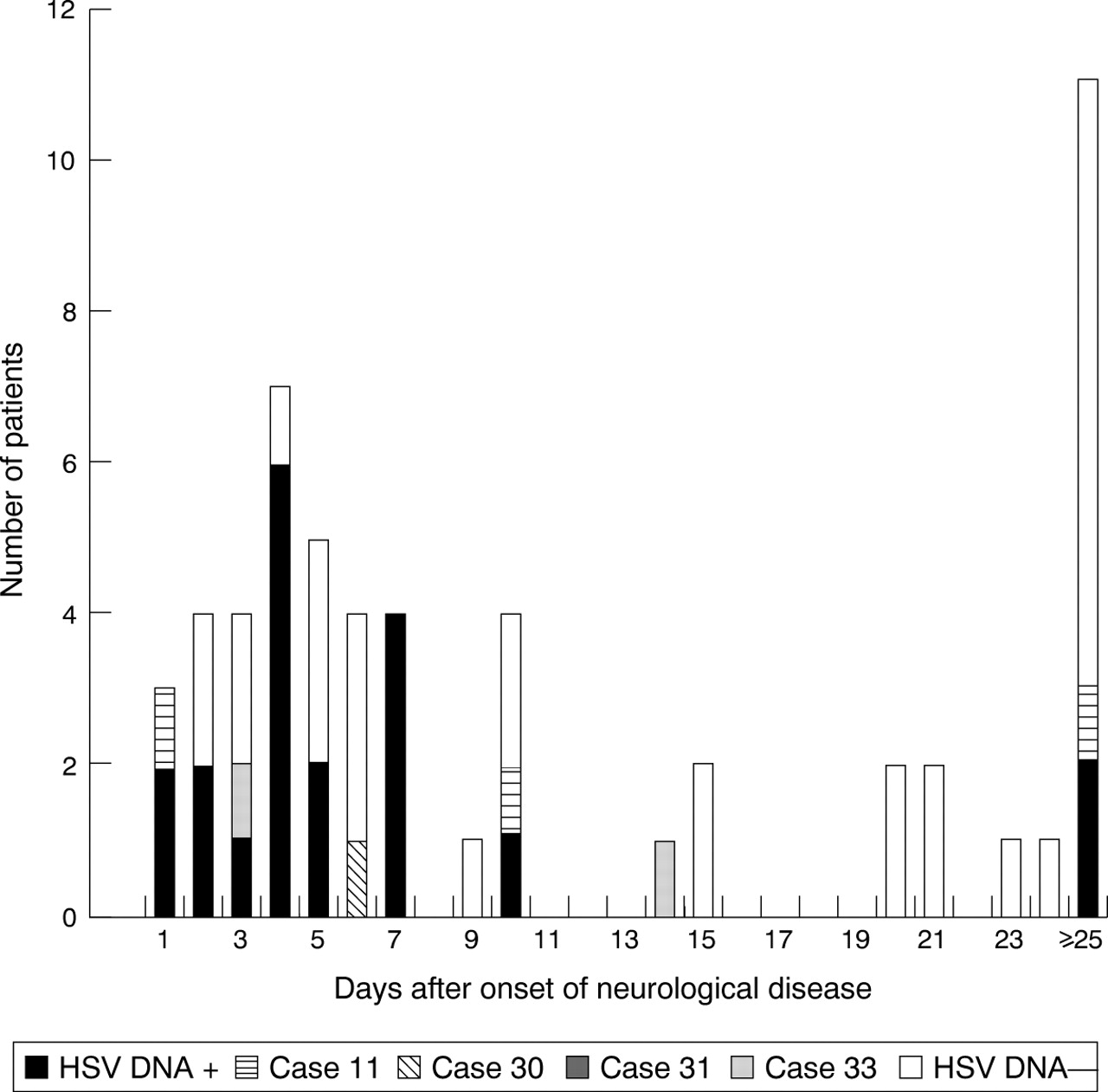
Figures 1 and 2 illustrate the relation between HSV DNA findings and day of collection of specimens in relation to onset of symptoms (neurological symptoms in central nervous system disease cases). The correlation between outcome in the children and the results of the HSV DNA analyses in available acute cerebrospinal fluid specimens is given in table 1. HSV DNA was demonstrable in cerebrospinal fluid in seven children, who were normal at follow up, whereas in two children (cases 16 and 20) with serious central nervous system damage the PCR analysis of acute phase CSF produced negative results.

HSV DNA in CSF in relation to days after onset of neurological disease in SEM and disseminated cases after onset of symptoms. Black, striped, or shaded pattern denotes positive HSV DNA. Acute and follow up specimens are included.

HSV DNA in serum in relation to days after onset of neurological disease in SEM and disseminated cases after onset of symptoms. Black, striped, or shaded pattern denotes positive HSV DNA. Acute and follow up specimens are included.
Among six children whose mothers had primary infections with no previous HSV infections (three had HSV-1 and three had HSV-2 infections) viral DNA could be demonstrated in acute serum from five. Viraemia was also found in two children infected with HSV-1 from an external source. There was no viraemia, however, in any of the five tested children of mothers with previous HSV-1 infection and primary HSV-2 infection. On the other hand, 13 of 17 children born to mothers with secondary infection, two HSV-1 and 15 HSV-2, had demonstrable viraemia measured as viral DNA.
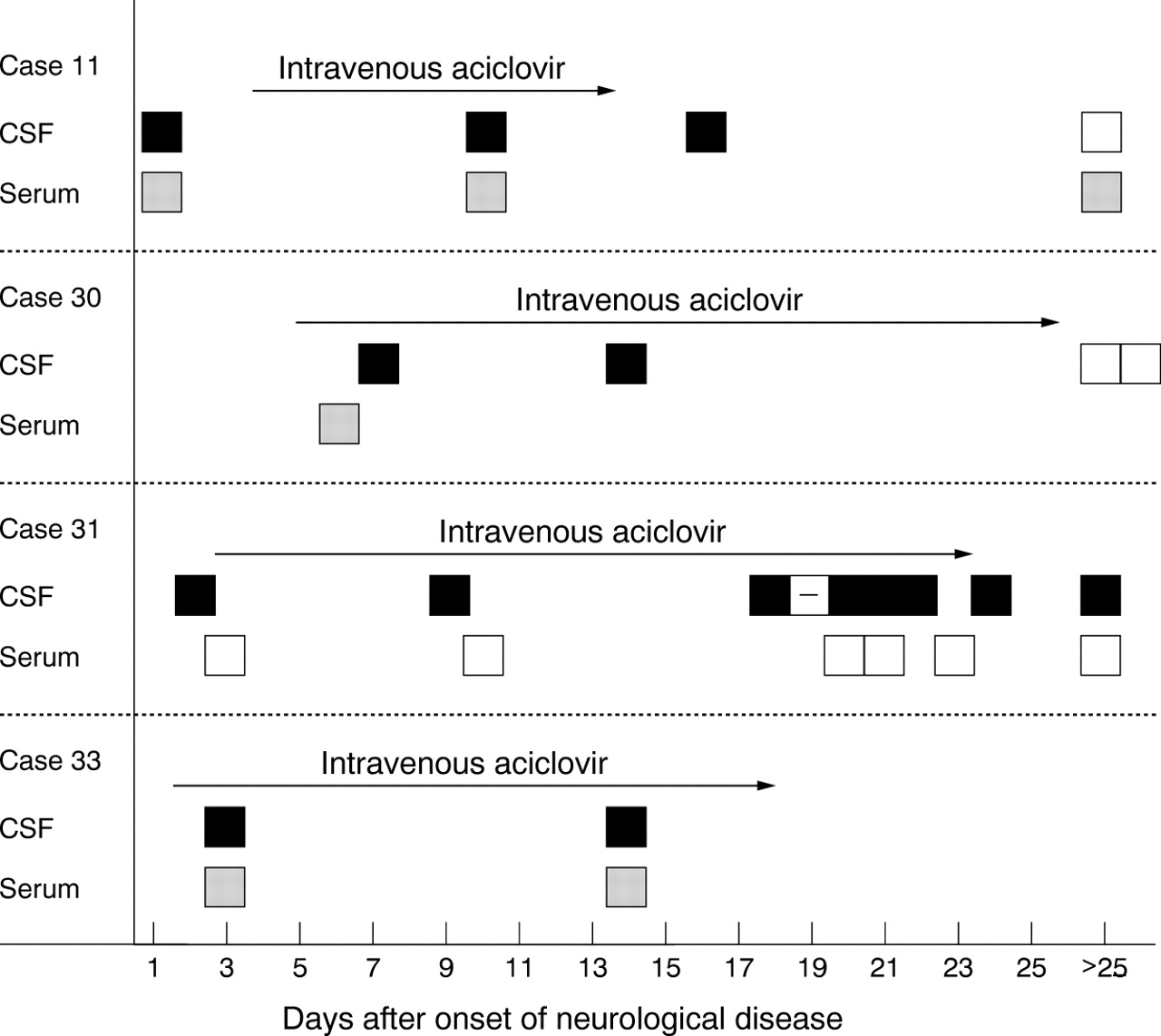
In 17 children sequential CSF (two up to nine samples) after initiation of intravenous aciclovir for 4–21 days (mean 16 days), were analysed using PCR. Cerebrospinal fluid samples beyond one week were positive in four severely impaired children (figs 1 and 3). In one child (case 11) with severe brain damage, leading to death at 4 years of age, HSV DNA was found during treatment and six days after a 10 day course of intravenous aciclovir, but not at the age of 4 months. However, serum was positive in all specimens even at 4 months (fig 3). The mother had primary type 2 infection two months before the birth of the child. In a second severely damaged child (case 30) cerebrospinal fluid was positive 7 and 14 days after onset of disease, but was negative at the age of 7 months. She was treated with intravenous aciclovir for 21 days, starting five days after onset of initial symptoms. The only serum available, drawn on day 7, contained HSV DNA (fig 3). In a third severely impaired child (case 31), the PCR was positive in all but one of many specimens (from ventricular drainage) during a 21 course of intravenous aciclovir (started two days after initial symptoms) as well as in the last available cerebrospinal fluid specimen drawn 24 days after the end of treatment. Viraemia was not found at any stage in this child (fig 3). A fourth child (case 33), severely impaired, had positive cerebrospinal fluid and serum three and 14 days after start of treatment for 16 days (fig 3). Cases 30, 31, and 33 were infected by a secondary infection in the mother. None of these children received long term oral aciclovir.
{kind=link}
{kind=link}
{kind=link}
HSV DNA findings in CSF and serum from four patients with persistent HSV DNA in CSF for 14 days or longer after onset of neurological symptoms. Timing and duration of aciclovir treatment (10 mg intravenously three times a day) is indicated by arrows. Positive HSV DNA finding is marked in black (CSF) or shaded (serum). Specimens with no demonstrable HSV DNA are indicated by open squares.
Discussion
The outcome for children with neonatal herpes virus infection depends on early treatment.1 Accurate and rapid aetiological diagnosis is required for adequate handling and evaluation of therapeutic strategies. Before the introduction of PCR the diagnosis of neonatal herpes simplex virus infections was based on virus isolation from peripheral lesions or brain9 and serological methods, together with the demonstration of characteristic or suggestive EEG changes5 10 11 and neuroradiological lesions in clinically suspected cases.12 13 However, EEG lesions do not develop until a few days after first symptoms of central nervous system involvement.5 10 11 The same is true for lesions visible on computed tomography.12 Lesions on MRI are seen earlier, but only after 1–3 days.13
Immediate virological diagnosis is often difficult. Diagnosis in children with apparent vesicles usually poses few problems; antigen detection in cell scrapings using immunofluorescence techniques allows a diagnosis to be made within a few hours or, using virus isolation, within a few days. In neonates with no visible vesicles—nearly half of the children with neonatal herpes encephalitis—the diagnosis has often been based on virus isolation or even serological investigation, confirming the diagnosis first in the late stages of the disease or retrospectively.6
The PCR technique for demonstration of viral DNA in CSF means that a diagnosis can be made within a day in clinically suspected neonatal herpes in cases both with and without vesicles. Demonstration of HSV DNA in CSF by PCR tests of high sensitivity (nested PCR) is now the most important and sensitive method for rapid non-invasive diagnosis of herpes simplex virus encephalitis. In adults the diagnostic sensitivity of the PCR procedure used in these studies is very high > 95%.3 In neonatal herpes encephalitis the sensitivity of demonstration of HSV DNA in cerebrospinal fluid has varied between 71 and 100% in different studies.2 14-16
Our study extends and confirms the results of the largest US study,2 in which HSV DNA was found in only 76% of children with neonatal central nervous system disease, compared with 78% in our study. Thus HSV DNA could not be demonstrated in all CSF samples from early phase disease with central nervous system involvement (table 1 and fig 1).
However, in this study just as in the US study, the specimens were retrospectively probed for HSV DNA, even if prospectively collected over more than a decade. Possible explanations for negative CSF and/or serum by PCR could be insufficient viral load, localised encephalitis without spread to the meninges, or inadequate sampling time during the very early or late stages of the disease. Technical explanations like degradation of DNA during freeze–thawing or prolonged storage of cerebrospinal fluid and sera, cannot be ruled out, although the very high sensitivity in corresponding retrospective probing of specimens from adults with herpes encephalitis does not make this a likely explanation.3 4
In the US study a positive CSF was evident in nearly all patients (93%) with disseminated disease.2 This may reflect different ways in which the virus spreads: in localised central nervous system disease the propagation of virus via neuronal transport to the brain may result in a localised infection before involvement of the meninges. In disseminated disease virus may have earlier access to CSF during a viraemic phase.6 9 However, in the few patients with disseminated disease included in our material, only one in three was positive.
Our material differs from the US material in the proportion of the different forms of neonatal diseases. Only one child out of 36 with localised skin–eye–mouth disease was included in our study compared with 42% in the US study,2 and in our study children with central nervous system diseases predominate. However, differences in classification despite the use of the same criteria cannot account for differences in the two studies. Rather, it is more likely that children with only localised vesicles in skin–eye–mouth disease were not clinically identified as having suspected herpes infection and thus escaped sampling and correct diagnosis. Only cases which subsequently progressed to central nervous system disease have been identified. Thus our Swedish data do not allow for any elucidation of the prognostic value of the finding of HSV DNA in cerebrospinal fluid in localised SEM disease.
Classification of the cases into central nervous system, disseminated, and SEM disease is not ideal, as far as we are concerned. This is shown by the fact that in the US study nearly 30% with SEM disease had positive cerebrospinal fluid by PCR, and thus involvement of the CSF.2 Furthermore, HSV-1 and HSV-2 infections behave differently even if the central nervous system is involved, as children with HSV-1 infections tend to have a milder, meningitis-like course compared with HSV-2 infections where there is a more serious clinical picture of encephalitis and convulsions.
The results of our study emphasise the importance of analysing both serum and CSF to both HSV-1 and HSV-2 DNA, to increase diagnostic sensitivity (table 1). These results agree with what has been published before, limited though the number of studies might be.14It is also important to keep in mind that although these new tools are of great value, a negative HSV DNA cerebrospinal fluid or serum, or both, by PCR does not exclude the diagnosis of neonatal herpes. A strong suspicion of neonatal herpes requires maximal efforts to obtain diagnosis, including the collection of supplementary samples for recovery of virus from the eye, nasopharynx, and urine, repeat cerebrospinal fluid samples for HSV DNA analysis, serological investigation of the child and his/her mother, in addition to EEG and neuroradiological investigations.
The use of HSV DNA detection in samples other than CSF or serum—such as from throat, nasopharynx and conjunctiva—is currently under investigation. Our retrospective study did not include this approach. A new intriguing idea to early demonstration of herpes DNA in children with suspected neonatal herpes may be the use of blood spots collected in Guthrie cards for phenyl ketonuria screening.17
HSV DNA in serum was shown in children born to mothers with not only primary but also secondary infections, although the rate in the secondary was not quite as high as in the primary infections. It is clear that viraemia occurs in spite of passively transferred maternal antibody. Viraemia was also found in the two children with generalised disease caused by HSV-1 from an external source. Against this background is the contrasting finding in children born to mothers with primary HSV-2 infection but with previous HSV-1 infections, for which there is no obvious explanation.
The demonstration of HSV DNA in cerebrospinal fluid in our study was not predictive of subsequent central nervous system damage (table1). However, persistence of HSV DNA in CSF after one week of neurological disease during or after completion of intravenous antiviral treatment was seen in four children with a very poor outcome (fig 1). In one of the children (infected from a mother with primary herpes type 2 infection some months before birth), serum HSV DNA also persisted during and after treatment (fig 2). Similar observations have been made in other studies.2 14
It seems possible that such long persistence of HSV DNA is a signal of a lack of host control over the infection in spite of drug treatment. However, further evaluation is required to assess whether monitoring of the HSV DNA titre in an individual case is a useful marker for evaluating therapeutic effect15; this is currently being done to assess the efficacy of antiviral drug treatment of HIV and hepatitis B and C. In adults the initial cerebrospinal fluid titre of HSV DNA has not been found to be of prognostic value,18whereas quantitative data from the US Collaborative Study19 have recently suggested that the initial CSF titre of HSV DNA may in fact be prognostic: HSV DNA concentrations of greater than 100 copies/μl seem to correlate with both reduced level of consciousness at presentation and with likelihood of future neurological impairment. Information on neonates is as yet scanty.15 Persistence or reappearance of HSV DNA may also reflect reactivation of virus in the central nervous system20 21 and demonstration and interpretation of HSV DNA in CSF in children with regularly reactivating skin lesion and central nervous system damage,5 requires further investigation.
In conclusion, the presence of HSV DNA in CSF and serum has increased the possibility of a rapid diagnosis and treatment of neonatal herpes virus central nervous system infections. The analysis of both specimens seems to enhance the diagnostic sensitivity. However, as the diagnosis in each child is of great importance for the treatment and future therapeutic possibilities it is important to keep in mind that for optimal diagnosis HSV DNA analysis in cerebrospinal fluid and serum does not replace the use of other diagnostic tools in a variety of specimens from throat, nasopharynx, eyes and urine when neonatal herpes is suspected.
Acknowledgments
This work is supported by grants from the following institutions: National Board of Health, Karolinska Institutet, and Samaritens foundation.
We thank Eva Skoog, Division of Clinical Virology, Huddinge Hospital, for excellent technical assistance.