Article Text

Presented in part at the annual meeting of the European Society for Pediatric Research, Rotterdam, The Netherlands, July 3–6 1994.
Abstract
AIM To investigate the pharmacokinetics, metabolism, and dose–response relation of a single rectal dose of paracetamol in preterm infants in two different age groups. Methods—Preterm infants stratified by gestational age groups 28–32 weeks (group 1) and 32–36 weeks (group 2) undergoing painful procedures were included in this study. Pain was assessed using a modified facies pain score. Results—Twenty one infants in group 1 and seven in group 2 were given a single rectal dose of 20 mg/kg body weight. Therapeutic concentrations were reached in 16/21 and 1/7 infants in groups 1 and 2, respectively. Peak serum concentrations were significantly higher in group 1. Median time to reach peak concentrations was similar in the two groups. As serum concentration was still in the therapeutic range for some infants in group 1, elimination half life (T½) could not be determined in all infants: T½ was 11.0 ± 5.7 in 11 infants in group 1 and 4.8 ± 1.2 hours in group 2. Urinary excretion was mainly as paracetamol sulphate. The glucuronide:sulphate ratio was 0.12 ± 0.09 (group 1) and 0.28 ± 0.35 (group 2). The pain score did not correlate with therapeutic concentrations.
CONCLUSIONS A 20 mg/kg single dose of paracetamol can be safely given to preterm infants in whom sulphation is the major pathway of excretion. Multiple doses in 28–32 week old neonates would require an interval of more than 8 hours to prevent progressively increasing serum concentrations.
- paracetamol
- pharmacokinetics
- pain score
- metabolism
Statistics from Altmetric.com
Presented in part at the annual meeting of the European Society for Pediatric Research, Rotterdam, The Netherlands, July 3–6 1994.
Even preterm neonates feel pain.1 Soon after birth, many painful procedures may be required for routine neonatal intensive care, and there are few data on the use of analgesics in preterm infants.2 In contrast to the use of paracetamol (acetaminophen, APAP) in term neonates,3 4 the use of APAP in the first weeks of life in preterm neonates is controversial, because its pharmacokinetics, pharmacodynamics, and metabolism in this age group remain unknown. Safety concerns may prevent its use in critically ill preterm neonates.
This study aimed to investigate pharmacokinetic variables after a single dose of rectally administered APAP in preterm infants, and to investigate whether there are any age dependent differences and any dose–response correlations between serum APAP concentrations and responses to pain during painful procedures.
Methods
Twenty eight inborn neonates who were admitted to the neonatal intensive care unit were included in the study. Entry criteria were the need for insertion of arterial and venous catheters or other painful procedures, such as insertion of a chest drain. The study protocol was approved by the ethical review committee and informed parental consent was obtained. As pharmacokinetics and drug metabolism change during the last three months of gestation,5-6 and pain sensitivity may be altered after 32 weeks,7 the neonates were stratified into two gestational age groups: 28–32 weeks (group 1) and 32–36 weeks (group 2). The gestational age of the neonates was estimated from maternal menstrual history, by routine ultrasound examination during pregnancy, and from postnatal physical characteristics (Farr score).8 Patients were excluded if they had congenital anomalies, if the mother received tocolysis with indomethacin, or if she had been given analgesics (other than local analgesia) within 24 hours before delivery. None of the infants had sepsis or other congenital infections, or documented periods of shock.
The infants were studied on the first two days after birth. Nasal intubation, if necessary, was performed in the delivery room and the patient was transported to intensive care. In each patient heart rate, respiratory rate, arterial blood pressure and oxygen saturation were monitored continuously, together with rectal and peripheral temperatures. According to standard procedures in intensive care, umbilical venous and arterial access was obtained, and parenteral nutrition was started within 24 hours of birth.
All patients were given APAP rectally after arrival in intensive care, within one hour of birth, the dose used being as close to 20 mg/kg as the available strengths of suppository (20 mg for birthweights 750–1249 g, 30 mg for 1250–1749 g, and 40 mg for 1750–2250 g) would allow. The nurses ensured that the suppository was retained. Suppositories contained 20, 30, or 40 mg APAP (particle size < 45 μm), and hard fat (Witepsol H 15), a synthetic mixture of mono-, di-, and triglycerides of the saturated fatty acids C10-C18. The suppositories were prepared and analysed for APAP content and content uniformity by the quality assurance laboratory of the hospital pharmacy.
Before APAP was administered a 0.1 ml blood sample was taken from the arterial catheter. Subsequently samples were taken at 30, 60, 120 minutes, 4, 6, and 8 hours in the first 10 neonates, with an additional sample at 12 hours in 18 neonates. After collection serum was separated and frozen at −200C, until assayed. Urine was collected for 48 hours using a plastic bag, and frozen in separate (3 hours) aliquots until analysis.
The assay was performed within a month of sample collection, using a modified high performance liquid chromatography (HPLC) method.9 Serum samples were extracted with perchloric acid and after centrifugation the supernatant fluid was injected into the HPLC column. Urine samples were diluted with distilled water (1:9) before injection into the column. Standards for serum APAP, urine APAP, APAP–glucuronide (APAP–G) and APAP–sulphate (APAP–S) were injected at the start and the end of each run. HPLC conditions, retention times, and ultraviolet detection were as described before.9 Limit of detection for serum APAP was 0.2 mg/l, recovery was 96%, and precision 2%. Detection limits in urine were 0.3, 2.3, and 6.3 mg/l for APAP, APAP–G, and APAP–S, respectively; recovery for APAP was 100%, for APAP–G and APAP–S 95%; and precision for APAP was 7%, for APAP–G and APAP–S 3%.
The values for each metabolite were converted to the equivalent weight of APAP, from which the metabolite was derived by correction for molecular weight. Standard metabolites were a generous gift from Sterling Health, Haarlem, The Netherlands. The calibration curves were linear over the range 0.5–40 mg/l (APAP) and 5–1000 mg/l (metabolites).
Pharmacokinetic data and variables were calculated from standard equations using the KINFIT program (Mediware, Groningen, The Netherlands). Concentration time curves were constructed to determine peak serum concentration (Cmax), time to reach Cmax, time to reach therapeutic concentrations (adult values 10–20 mg/l),4 10 and serum half life of the drug (t½). For t ½,, a minimum of two time points in the elimination phase was used. Kinetic constants for APAP elimination were calculated according to the two compartment model as used by Miller.11 For calculations a bio-availability of 90% was assumed.
Because all infants were nursed in incubators with a relative ambient humidity of 60–70% and temperature settings that aimed at a neutral temperature between 36.5–37.2°C, the anti-pyretic effects could not be measured.
Pain was assessed by nurse pairs or nurse/doctor pairs with a modified five facies pain score, showing increasing levels of discomfort from 0 (no pain) to 4 (clearly/obviously in pain).12 13
Data were analysed using the Statistical Package for the Social Sciences, SSPS Inc., Chicago, Ill, USA.14 Student’st tests were used for normally distributed data and Mann-Whitney U tests for non-parametric data to compare the two groups. Least squares regression was used to evaluate linear correlation between variables. P values of < 0.05 (two tailed) were considered significant.
Results
Of the 28 infants studied, 21 were in the 28–32 week group and seven in the 32–36 week group. Demographic data are shown in table 1. Serum APAP concentrations are shown in figs1A–C.
Demographic data of study participants

(A) APAP serum concentrations after a single dose of 20 mg/kg, after 30 minutes to 8 hours in 10 infants (group 1); (B) after 30 minutes to 12 hours in 11 infants (group 1); and (C) after 30 minutes to 12 hours in seven infants (group 2).
Analgesic therapeutic concentrations (adult values 10–20 mg/l)4 10 were reached in 17 infants, in 16 out of 21 in group 1 (76.2%), and in one out of 7 (14.3%) in group 2. Therapeutic concentrations persisted for 8 hours in 13 infants (12 in group 1 and one in group 2) and for 12 hours in one infant. Cmax was mean 11.2 (SD 3.8) mg/l for all infants studied; data for groups 1 and 2 are shown in table 2; Cmax was significantly higher in group 1. For individual values there was a significant negative correlation between Cmax and gestational age (r -0.50, p=0.007). There was a significant inverse linear regression between APAP concentrations at t60 (p<0.05), t120 (p=0.008), and t240 (p<0.05) with gestational age (fig 2) and no significant correlation between Tmax and gestational age. As serum concentrations were still in the therapeutic range after 8 hours, T½ could not be measured in 10 infants in group 1 because elimination of APAP was not yet apparent (fig 1A). Therefore, T½ could only be measured in 11 infants in group 1 but it was measured in all infants in group 2 (table 2). In two infants only two pieces of data were available to calculate T½; in the other 16 infants three or more time points were available. The area under the serum concentration time curve (AUC) was determined by the trapezoidal rule. The mean (SD) value in group 1 (95.1 (28.0) in 11 infants) was significantly higher than in group 2 (71.7 (41.7); p=0.046). Clearance increased with gestational age, showing a significant positive correlation (r=0.52, p=0.008)(table2).
Pharmacokinetic parameters of paracetamol in preterm neonates after rectal single dose

Linear regression analysis of gestational age on APAP concentrations at t120 minutes: r−0.49, p 0.008; dashed lines indicate confidence limits.
Due to the available strengths of the suppositories, individual doses ranged from 16.6–26.6 mg/kg in group 1, and from 17.1–22.1 mg/kg in group 2; the relation between APAP dose and Cmax is shown in fig 3. All doses of more than 18 mg/kg resulted in therapeutic concentrations in group 1, but not in group 2. There was a significant correlation between the rectal temperature and time to reach therapeutic concentrations (r -0.54, p<0.03), and no correlation between rectal temperature and Cmax.
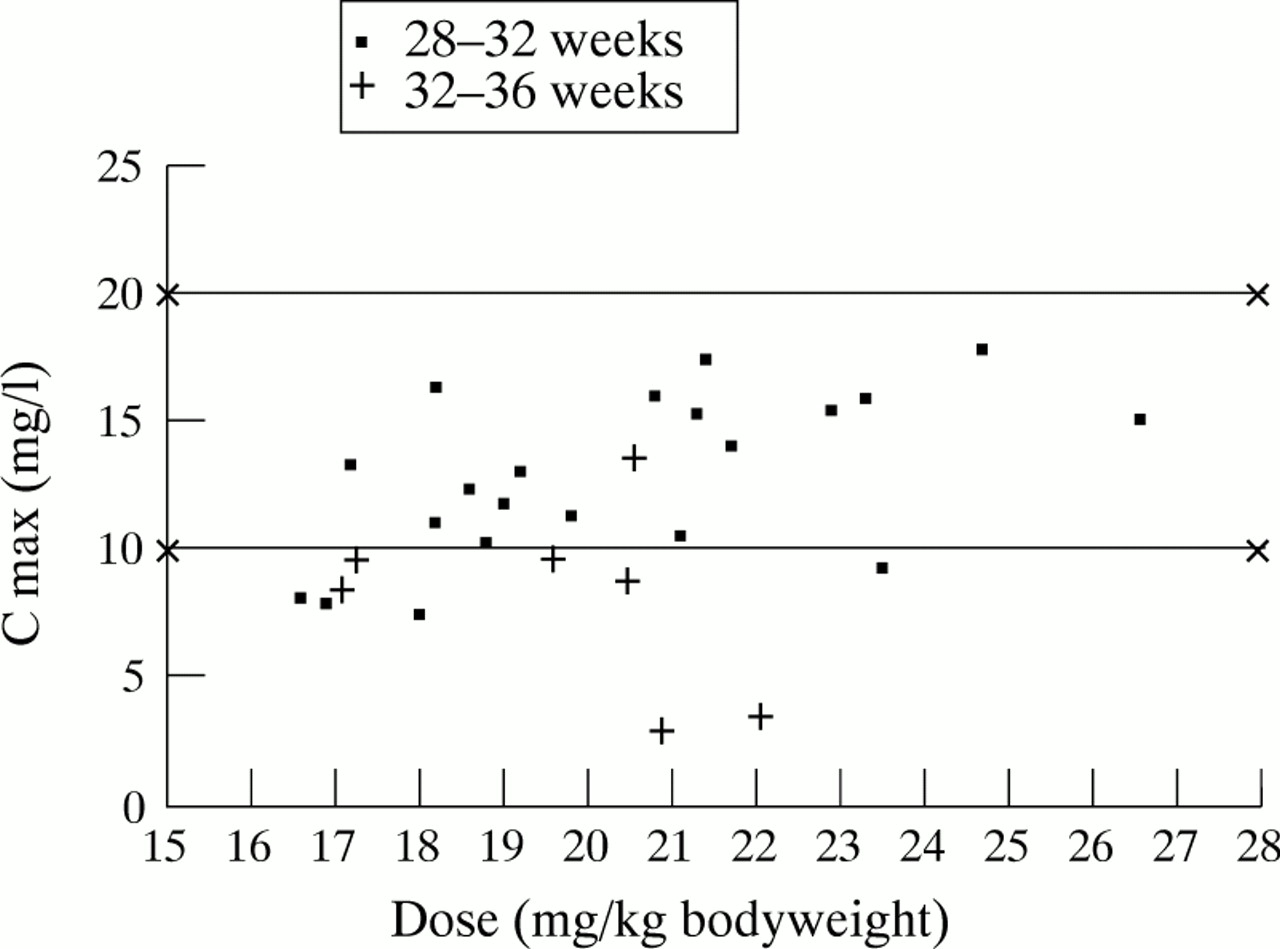
APAP peak serum concentrations in preterm infants in relation to dose, in two different age groups: group 1 28 to 32 weeks (n=21), group 2 32 to 36 weeks (n =7). Therapeutic concentrations represent adult values.
No significant losses occurred during urine collection. Of the rectal dose, 63.2 (24.4)% was recovered in the urine; 61.0 (24.4)% in group 1 and 74.2 (24.8)% in group 2 (NS; p=0.2). APAP was excreted mainly as APAP–S and to a lesser extent as APAP–G. Very small amounts of free APAP, and APAP–cysteine (APAP–C) were excreted and APAP–mercapturic acid (APAP–M) was not detected. The glucuronide:sulphate ratio (G:S ratio) was 0.12 (0.09) and 0.28 (0.35) for groups 1 and 2, respectively (fig 4).

{kind=link}
{kind=link}
{kind=link}
{kind=link}
Facies pain score reflecting the infants’ responses was scored at the time of blood sampling. Pain scores from 0 to 2 were obtained in all infants and did not correlate with therapeutic concentrations. The reliability of the pain score was high; weighted Cohen’s κ=0.74.
Discussion
As far as we are aware this is the first study to provide data on the pharmacokinetics and metabolism of APAP in preterm infants. As the rectal mode of delivery results in less efficient absorption than the oral route, higher doses are needed in infants and in older children. After rectal doses of 16–26 mg/kg none of our infants reached concentrations above 20 mg/l, while toxic concentrations occur above 120 mg/l four hours after ingestion.15 In infants whose mothers ingested an overdose of APAP prenatally, high concentrations of APAP (75.5 and 260 mg/l) were documented in neonates with no apparent hepatic or renal toxicity.16 17 The high therapeutic ratio in neonates may be related to reduced rates of metabolism by the cytochrome p 450 system in neonatal liver and neonates’ increased ability to synthesise gluthathione relative to adults.18 19 Young mice have a fourfold greater gluthatione turnover and increased activity in the gluthatione peroxidase/reductase system than older mice.18 19 Renal toxicity is also prevented by the increased solubility of APAP–S as compared to APAP-G, the major metabolite in adults.We speculate that multiple doses of APAP would also be safe in the preterm infants studied.
Peak serum concentrations were reached later in preterm infants in our study than in term infants and adults,4 20 but most 28–32 week old infants did achieve therapeutic concentrations. All the infants in our study were under 1 hour of age, and absorption may increase with gestational and postnatal age. Individual differences in rectal temperature (range 34.7oC–38.4oC) at the time of administration of the suppository may alter the time needed for melting and absorption. A significant correlation occurred between rectal temperature and the time to reach therapeutic concentrations. Rectal temperature ranged from 34.8 to 36.8 in 10 infants who did not achieve therapeutic concentrations (> 10 mg/l). Although no suppositories were expelled, differences in Cmax and Tmax in individual patients may be due to the variability of venous drainage from the rectum. Drugs administered into the proximal rectum will be subject to the hepatic first pass effect, whereas drugs in the distal rectum will bypass the liver.5The inverse linear regression between APAP concentrations and gestational age may be due to the larger extracellular space and thus greater volume of distribution (Vd) with lower gestational age.21 Although our sampling time was two to four times greater than the T½ in adults and term neonates,17 22-24 serum concentrations remained above therapeutic concentrations for more than 8 hours, which made it impossible to assess T½ in 10 preterm infants. In infants where assessment was possible, the values indicated slow elimination, subsequent to a lower clearance and increased Vd.
Miller et al found shorter T½ in three term infants and one preterm infant than in older children and adults after oral APAP.11 Other studies found longer T½ after rectal APAP in infants compared with oral doses in adults.4 22 23 Our T½values were 11 hours in infants 28–32 weeks of gestation and 4.8 hours in infants 32–36 weeks of gestation and were inversely related to gestational age. This agrees with the published findings, with values of 2.7 to 4.9 hours in term infants in the first month of life and of 1.0 to 2.4 hours up to the age of 1 year.10 Doses of 18 mg/kg or more produced therapeutic concentrations in the 28 to 32 week gestation group, and doses up to 26.6 mg/kg were given without any adverse effects. Because of the long T½ we recommend that multiple doses should be given every 8 to 12 hours.
The pain scores we used12 13 did not correlate with the concentrations of APAP, probably because most of the infants scored low on the pain score indicating minimal or no pain. It may be that this pain score is not particularly suitable for measuring pain in preterm infants or that it is only suited for the assessment of acute severe pain. In the original study this pain score was used for older infants,12 and later modified for use in younger infants.13 Manne et al showed that in older children simultaneous assessment of pain by patients, nurses, and parents showed comparable results.25 Postgestational age seems to be important when considering the pain response of infants of less than 32 weeks of age.26
In several double blind cross over studies in healthy volunteers given normal therapeutic doses, analgesic effects occurred with concentrations < 10 mg/l.20 If the same applies for the infants in our study, they were having suitable pain management and the pain score was appropriate.
Exaggerated concerns for overdosing and hepatotoxicity, or increased bilirubin concentrations have been the main reasons for withholding APAP from neonates. Neonates are capable of metabolising APAP, not by glucuronidation but also by sulphation,11 22 27 and there is no correlation with plasma bilirubin concentration.22
Limited data show that even when APAP reaches toxic concentrations in preterm neonates, detoxification by the mixed function oxidase system is sufficient, without any adverse effects.16 17 Even when glucuronide and sulphate conjugation (phase II reaction) have reached their maximum capacity, this normally minor pathway metabolises APAP as long as glutathione is not depleted. Part of the APAP is not metabolised and excreted unchanged in the urine.
Our findings that urinary excretion was primarily as APAP–S, resulting in a low glucuronide to sulphate ratio, agree with the results of earlier studies.11 16 22 The values in our groups show a considerable decrease in G:S ratio with earlier gestational age. Fig 4shows the comparison of G:S ratio in our study with two other studies in older infants, children, and adults.11 22 Our results are supported by several studies showing decreased fetal and neonatal UDPG-T activity,28-30 and by the presence of a well developed sulphation pathway both in vivo21 in term neonates and in vitro31 in fetal liver at 19–22 weeks of age. Furthermore, two other studies showed even higher sulphation rates than those of glucuronidation in children aged 7–10 years, compared with adults.11 32 Our results differ from those of a recent study in which 2 to 6 day old term infants ingested paracetamol in their mothers’ breast milk in amounts of 0.3–18.5 mg/kg, and excreted it mainly as APAP–G.33 However, in this study urine sampling only took place for 3 hours; in other words with the longer T½ in infants a substantial part was not yet excreted and maximal recovery of the ingested dose was 4.4%.33
We found only minute amounts of APAP–C and no APAP–M in the urine. As APAP–M was found in urine of a preterm infant after maternal overdose,17 it might be that in preterm infants APAP–M is only formed after doses higher than our dose or after prolonged multiple doses, or that it is merely a reflection of their mothers’ excretion pattern.
We conclude that rectally administered APAP is safe in preterm infants as single dose treatment. As prolonged rectal absorption from this dose is evident, a higher dose might be needed to shorten the interval to reach therapeutic concentrations. Prolonged rectal absorption and plasma clearance subsequent to developmental immaturity in the phase I and phase II pathways which govern APAP clearance were evident. Rectal APAP was apparently tolerated without any overt evidence of adverse effects.
Sulphation is the major metabolic pathway, while the G:S ratio is positively related with post conceptional age. Furthermore, our study provides new ways of using APAP: in preterm infants the choice is no longer strong analgesics or no analgesic, but an intermediate analgesic for moderate pain.
Acknowledgments
We gratefully acknowledge the contribution by the nurses from intensive care to the collection of the data, and Willem Grol for his statistical advice.