Article Text

Abstract
AIM To define the normal range of systolic blood pressure in a non-selective population based sample of babies of low gestation throughout early infancy.
METHODS Daily measurements of systolic blood pressure were made in all the babies of less than 32 weeks gestation born in the North of England in 1990 and 1991 during the first 10 days of life. Additional measurements were obtained from 135 of these babies throughout the first year of life. Systolic pressure was measured by sensing arterial flow with a Doppler ultrasound probe. It was assumed that blood pressure had never been pathologically abnormal in the neonatal period if the child was alive and free from severe disability two years later. Data of adequate quality were available from 398 such children. Additional data were collected, for comparative purposes, from 123 babies of 32, 36, or 40 weeks of gestation.
RESULTS Systolic pressure correlated with weight and gestation at birth, and rose progressively during the first 10 days of life. The coefficient of variation did not vary with gestational or postnatal age (mean value 17%), the relation with gestation being closer than with birthweight. Systolic pressure rose 20% during the first 10 days from an initial mean of 42 mm Hg in babies of 24 weeks gestation, and by 42% from an initial mean of 48 mm Hg in babies of 31 weeks gestation. These findings were not altered by the exclusion of data from 14 babies who had inotropic support during this time. Simultaneous measurements in three centres using an oscillometric technique revealed that this technique tended to overestimate systolic pressure when this was below average. Systolic pressure finally stabilised at a mean of 92 (95% CI 72-112) mm Hg at a postconceptional age of 44–48 weeks irrespective of gestation at birth.
CONCLUSION Systolic blood pressure 4–24 hours after birth was less than gestational age (in weeks) in only 3% of non-disabled long term survivors. Systolic pressure rose with increasing gestation and increasing postnatal age, but stabilised some six weeks after term, regardless of gestation at birth.
- systolic blood pressure
- early infancy
- gestation
- birthweight
Statistics from Altmetric.com
Blood pressure is now widely monitored in preterm babies needing neonatal intensive care, but normative data remain sparse. Several studies have reported normal ranges for small selected groups of babies in the first 12 hours of life,1-5 but less is known about the precise way pressure changes during the next few weeks of life.6-11
During a collaborative regional study of every baby born before 32 weeks of gestation, the opportunity was taken to measure systolic blood pressure daily for the first 10 days of life. Non-invasive measurements were obtained using a Doppler ultrasound device to sense arterial flow distal to a pressure cuff on the arm, because this made it ethically possible to obtain data using a well validated technique on babies who were healthy as well as on babies who were ill. In deriving the ranges for blood pressure cited in this report measurements from babies who died, or who had a clinically significant disability on follow up two years later, were excluded from consideration. No other exclusions were made. The results can, therefore, be treated as coming from an unbiased population based sample of children.
Methods
A prospective region wide collaborative study was undertaken of every pregnancy to a mother normally resident in the northern region ending in delivery at 22 to 31 weeks of gestation in 1990 and 1991, and this study included a formal, independent neurodevelopmental assessment of all the 566 survivors at the age of 2 years.12 To make the most of the opportunity several observational studies and two collaborative trials of early nursing management were factored into this study. The studies were approved by each of the 16 research ethics committees in the region. Recruitment and documentation was then co-ordinated by senior nursing or midwifery staff in each of the 19 maternity units serving the region.
This report summarises the result of the prospective study of systolic blood pressure. Except in two centres, where 47 babies had aortic pressure measured directly in the first few days of life, systolic pressure was measured using an inflatable cuff that more than surrounded the arm, with a width that was between 40% and 65% of the arm’s circumference.13 14 Flow distal to the cuff was then sensed using a Doppler ultrasound flow device.15-19The results presented here relate to routine once daily nursing measurements taken at a fixed time each day (9 am in two centres and 8 am in the remainder) with a mercury column while the baby was supine and quiet or asleep. Pressure was usually read to the nearest 2 mm, but a minimum of three readings were usually taken and averaged (the initial reading being ignored if it caused a noticeable startle response). Measurements taken on babies less than 4 hours old were excluded from consideration. In three centres simultaneous measurements were also made in some babies using an oscillometric technique,14 and in one centre similar measurements were made using pulse oximetry.20
The results presented here relate to all the 398 babies who had reliable daily measurements of systolic pressure recorded, and who were alive and free from any severe disability two years later.21 In 135 of these babies further measurements on systolic blood pressure were made at approximately three weekly intervals until the babies reached a postconceptional (gestational plus postnatal) age of 44 weeks. Further measurements were made on the latter six and 12 months after birth. None was receiving treatment for hypertension at the time of study.
Additional studies were undertaken in one unit between 1990 and 1993 to determine how these blood pressure findings compared with those found in babies of more than 31 weeks of gestation. For this supplementary study 123 babies of 32, 36, or 40 weeks of gestation had measurements of resting systolic pressure taken 0, 1.5, three, five and eight weeks after birth. A further final measurement was made when the babies were 1 year old.
The lines linking the mean values shown in figs 1 and 2 were drawn by eye to avoid imposing any a priori mathematical relation on the data. None of the data points used to construct fig 2, and only four of the 88 data points used to construct fig 1, were more than 1.5 mm Hg from the resultant line.

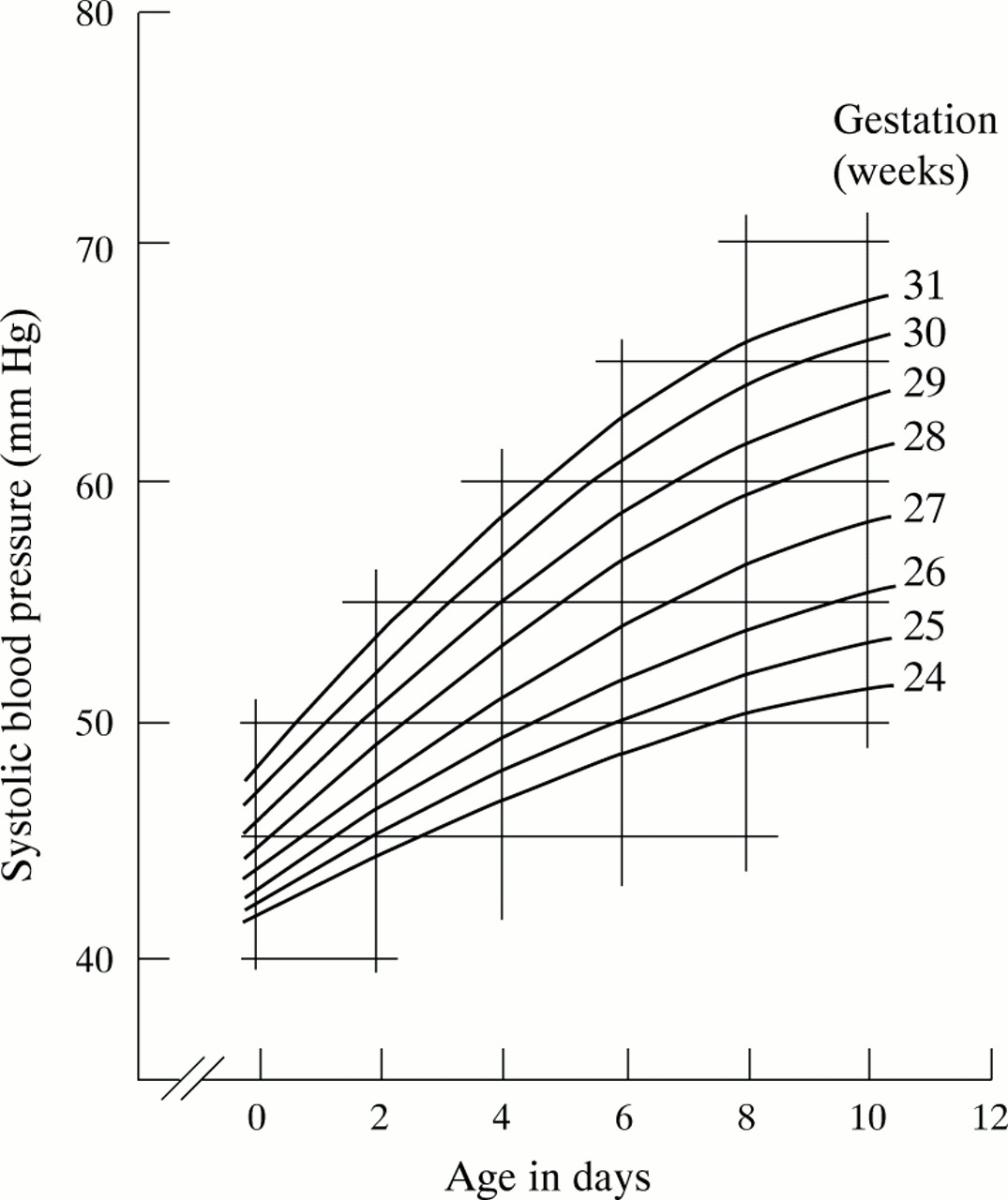
Relation between mean systolic blood pressure and gestational age in babies of 24 to 31 weeks gestation in the first 10 days of life. To calculate the 3rd and 97th centiles subtract or add 35% from the mean value shown.

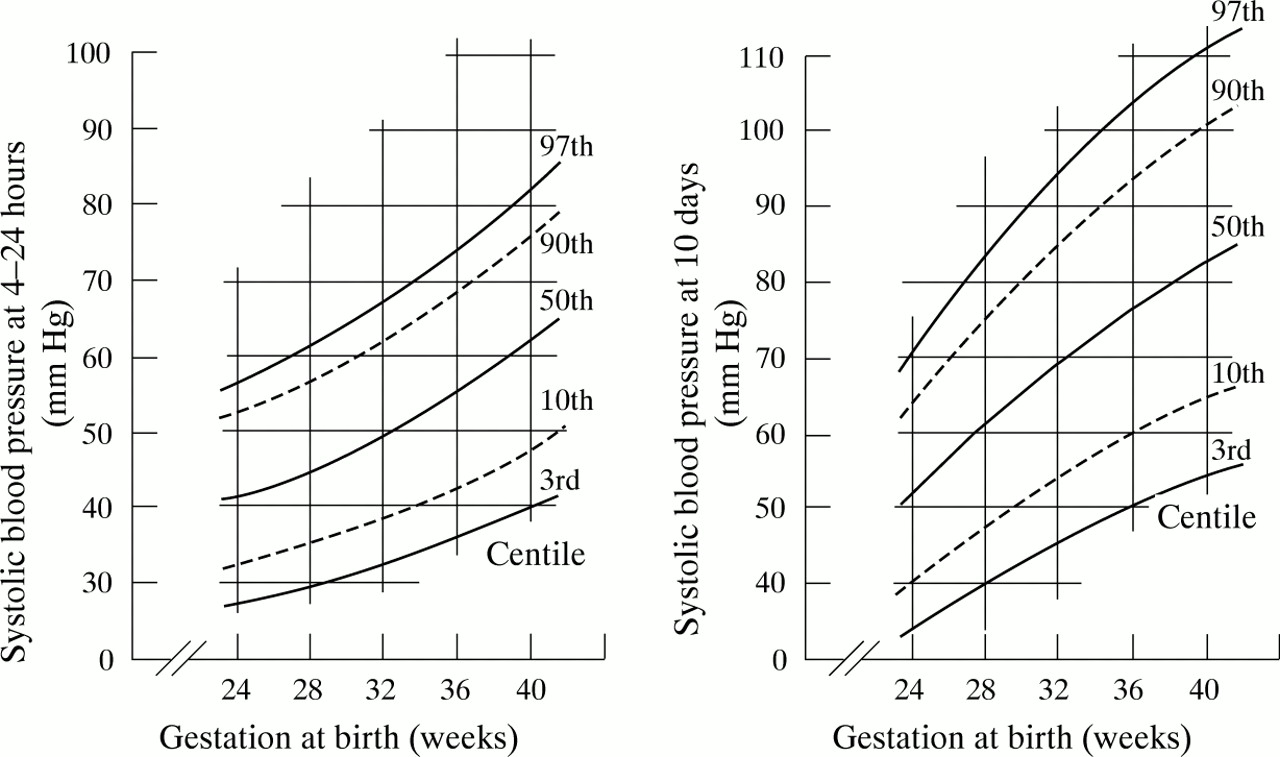
Range of systolic blood pressure seen in babies of 24 to 40 weeks of gestation when (A) 4 to 24 hours old and (B) 10 days old.
Results
The way in which mean systolic pressure rose in the non-disabled survivors during the first 10 days of life is shown in fig 1. The results are shown in relation to gestational age, because the variation of pressure with gestation was marginally less than the variation of pressure with birthweight throughout this time. Blood pressure seemed to be normally distributed with a coefficient of variation (17%) that was not influenced by gestational or postnatal age. Centile lines for systolic pressure in these babies, and in the babies of 32, 36, and 40 weeks gestation, on the first and tenth day of life are shown in fig 2. The difference in the shape of the two curves is caused by differences in the rate at which pressure rises during the first two weeks of life in babies of differing gestation.
Almost all the babies of less than 32 weeks gestation in this study were included in a trial comparing three approaches to early nursing care in the first 2 hours of life.12 In one arm of this study babies were given 20 ml/kg of fresh frozen plasma intravenously over 15 minutes immediately after randomisation, while those in a second arm received a comparable volume of a gelatin based plasma substitute. Those in the third arm merely received a control infusion of between 60 and 120 ml/kg per day of 10% dextrose or dextrose–saline. The babies who received elective volume expansion in this way had a mean systolic pressure that was 2.8 mm Hg higher than those in the control group on the day of birth. The difference was not significant, and no difference was detectable on subsequent days.12 Trial guidelines required resident staff to obtain consultant approval before giving further blood or colloid, or starting inotropic support in these babies. Babies had to have had a systolic blood pressure below the fifth centile using Versmold’s data3 for at least one hour and evidence of poor peripheral perfusion (a capillary filling time of > 5 seconds).22 Only 21 of the non-disabled survivors had further colloid, and only 14 had inotropic support in the first week of life. Excluding the data from these children did not alter the relation shown in fig 2. No baby received steroid treatment.
Blood pressure continued to rise slowly in preterm babies more than 10 days old. In the sample of children who continued to be monitored, blood pressure seemed to stabilise by a postconceptional age of 44 to 48 weeks. No further significant rise in resting blood pressure was seen during the first year of life (fig 3). Since none of the babies whose data were used to define the pressure relation after the second week of life had ever had an aortic catheter in situ, or postnatal steroid treatment, the values quoted can be taken to indicate the usual upper limit for systolic blood pressure in infancy not influenced by medical treatment other than respiratory support.

Relation between mean systolic blood pressure and postconceptional age in babies of 24 to 25 (o) and 31 (•) weeks of gestation at birth during the first year of life. The coefficient of variance of the means ranged between 9 and 14%. Data on term babies from de Swiet.29
Babies with a systolic pressure above or below average on any given day also tended to have similar values on other days in the first 2 weeks of life. There was, nevertheless, a one in five chance that blood pressure would differ by 20% or more on consecutive days. The centile position for systolic blood pressure in the first week of life bore no relation to its position 3 to 12 months later.
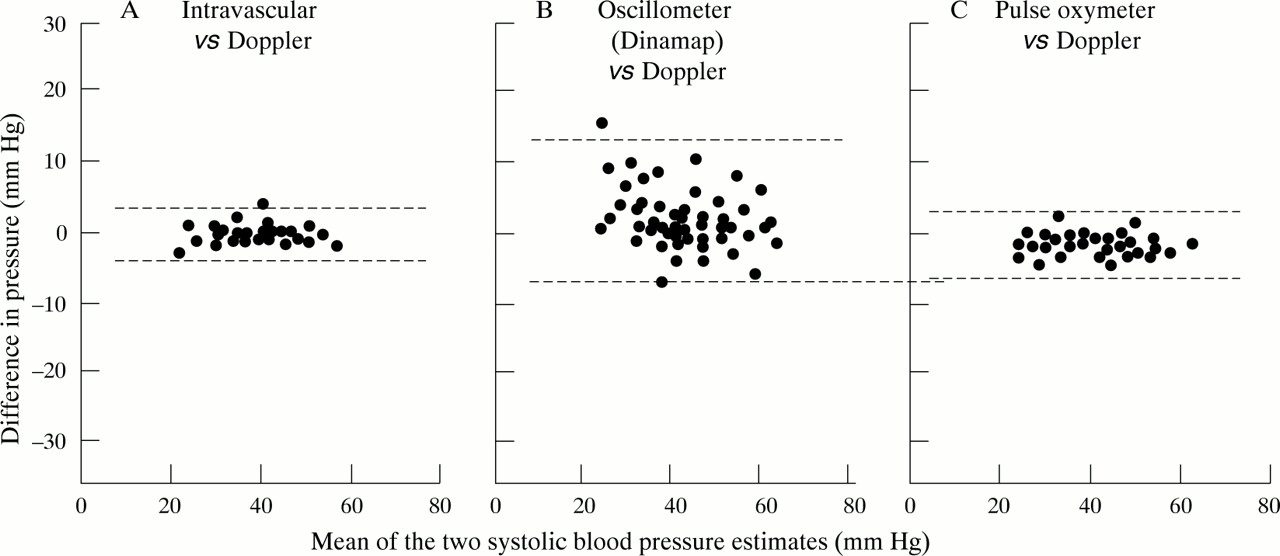
There was good agreement between direct intravascular and indirect Doppler measures of systolic pressure, and between Doppler and pulse oximeter measures throughout the blood pressure range. Oscillometric measures showed greater scatter, and frequently exceeded Doppler measures when systolic pressure was low (fig 4).

{kind=link}
{kind=link}
{kind=link}
{kind=link}
Relation between (A) intravascular, (B) oscillometric, and (C) oximeter measures of systolic blood pressure and Doppler measures in babies of 26 to 29 weeks of gestation when 1 to 5 days old. Note the greater variability of the oscillometric readings. Dotted lines represent 95% confidence interests.
Discussion
Systolic blood pressure often changes rapidly in the period immediately after birth. Pressure in term babies is nearly always high in the first 2–3 hours of life,23-25 even after delivery by caesarean section,24 and pressure is particularly high in babies showing signs of moderate asphyxia.24 Blood pressure in the quiescent baby is lower after that. Small preterm babies, conversely, often have a very low pressure immediately after birth that rises spontaneously before stabilising by about 6 hours,4 and blood pressure in the preterm baby with a low Apgar score can be particularly low in the first few hours of life.5 For these reasons it is important to exclude such early readings when presenting data on the range to be expected once pressure has finally stabilised. This has not been done in most previous studies.1-3 The statistical validity of the published ranges is further compromised by the inclusion of multiple readings from each of a small number of babies. The most widely used reference range3 used 9 to 12 observations collected within 12 hours of birth from each of just 61 carefully selected babies weighing between 610 and 4220 g at delivery. The resultant range reflects intra- not interpatient variability.
Many studies have documented the subsequent rise in systolic pressure in babies born at term during the first week of life,26-28 but de Swiet was the first to report the way that systolic pressure changed in a population based sample of babies born at term both throughout the first year of life,29 and subsequently.30 This is the first study to report such changes in a population based sample of preterm babies. It is also the first to use the same reliable technique for measuring blood pressure as in the study by de Swiet. We believe that the utility of this normative data is enhanced by a knowledge that the results have not been influenced by the use of postnatal steroids,31 32inotropes, or antihypertensive drugs. The findings are further enhanced by a knowledge that all the children were developmentally normal two years later.
The range of systolic pressure seen in our study was substantially wider than the erroneously narrow limits quoted by Versmold,3 but less than in some recent studies using oscillometric methods.7 8 10 Systolic pressure is known to fall by about 8% during sleep,7 27 29 33 and undocumented differences in the sleep state almost certainly account for part of the wide variance reported in the younger babies in the present study. Very few of the older children seen for further assessment after discharge were asleep when assessed (although all were quiescent), which could account for the lower variance seen (11%). Whether this is the explanation, the ranges cited here can be taken as reflecting those commonly seen during routine clinical care.
Often, too little attention is paid to the accurate measurement of blood pressure. Although oscillometric methods of measuring blood pressure14 34-45 are now widely used, neonatal readings are of limited accuracy. Errors of 10 mm Hg are not uncommon,40 42 43 and bias develops when pressure is low (fig 4). The technique becomes least reliable precisely when it needs to be at its most reliable—in babies with clinically significant hypo tension.42 45 The tendency to overestimate systolic (and mean) blood pressure can also be seen in other studies that make no mention of this measurement bias.34 38 39The technique should not be used in neonates merely because it is easy and convenient to use when other cheaper and more reliable non-invasive methods are available, as this study again shows. While the technique seems to work reasonably well in older children,34 44 it may not always reliably recognise hypertension.40 The Doppler technique used in our study has been found reliable by others,15 17-19 38 but automated devices that use a sensor placed under the pressure cuff46-48 seem less reliable.49 The pulse oximetry technique, as independently described by Langbaum and Eyal,20 deserves to be a more widely used alternative, because it often disturbs the baby less than a Doppler probe.
No technique of indirect measurement will deliver a reliable result if an inappropriate cuff is selected. Erroneously high readings will be obtained if the cuff’s functional width does not exceed 40% of limb circumference.13 14 40 It is less widely recognised that high readings will also be obtained if the cuff is excessively wide,14 50 51 or the cuff’s inflatable bladder does not almost completely surround the arm.13 29 38
The relation between weight, gestation, and blood pressure at birth has been reported before.10 A progressive rise in systolic pressure during the first week of live in the very preterm baby has also been documented in some,6 10 but not all,52 previous studies. Two other studies, only ever reported in abstract, reported the same rise.53 54 There is a suggestion that the slower rate of rise in the least mature babies may be linked, in some way, to the high incidence of patent ductus in these babies in the first week of life.55 56 The stability of blood pressure in term babies more than six weeks old has also been reported,29 as has the continued slow rise in blood pressure in preterm babies,10 57 58 but the realisation that blood pressure stabilises at much the same level in preterm babies as in term babies at a similar postconceptional age is new. Sex was reported to have an influence on blood pressure in two recent studies.59 60 No such effect was seen in this, or earlier, studies. Nor was there any relation between blood pressure in early infancy and blood pressure at one year, although such trends do become apparent in later childhood.30 61 62
For the past 20 years, mean pressure has been the yardstick by which the normality of blood pressure has been most often assessed. Unfortunately, little is known about the way this varies with postnatal age, because catheterisation can not be justified to obtain normative data in healthy children. Most63-68 of the available data sets show trends for mean pressure that are similar to those for systolic pressure reported here, but this is not universally true.53 Mean pressure, rather than systolic pressure, is often used when judging the normality of data taken from an arterial line because it is thought to be free of the artefacts caused by resonance, thrombi, and air bubbles, but this may not always be true either.69 There are no other good reasons for monitoring mean pressure rather than systolic pressure.
What this study makes available for the first time is reliable information on the range of systolic pressure that may be considered physiologically normal in babies of any gestational and any postnatal age throughout the first year of life. Even then it needs to be remembered that values that are statistically abnormal are not necessarily pathological: oxygen delivery to the tissues is influenced by cardiac output and blood flow, more than blood pressure, and that there is little direct correlation between pressure and volume,70 or pressure and cardiac output,71or pressure and cerebral perfusion.71
Acknowledgments
Recruitment and data collection for this study were coordinated by the following senior neonatal nurses in each maternity unit in the North of England:
L McCoy (Ashington), L Atkinson (Barrow), S Leak (Bishop Auckland), L Ellis and S Whyte-Earl (Carlisle), S Richardson (Consett), D Tunstall and S Turner (Darlington), G Barritt and M Harrison (Durham), H Asl (Gateshead), H McKinnell (Hartlepool), J Harbottle (Hexham), K Swailes (Lancaster and Kendal), A Lampson and D Greensitt (Middlesbrough), B Watson and S Cook (Newcastle), S Golder (North Tyneside), L Malcolm (South Shields), B Harrison (Stockton), S Shilling and J Martin (Sunderland), and H Tedford (Whitehaven). Resident medical staff helped with recruitment and data collection in Newcastle.
This study was planned for the Northern Neonatal Network by Drs Adrian Grant, Edmund Hey, David Milligan, Sam Richmond and Sunil Sinha. Data coordination and follow up were organised by Susan Fritz (Newcastle), and every survivor seen and assessed individually at two years by Dr Win Tin (Middlesbrough). The data on blood pressure were analysed by Mr Angus McNay (regional statistician) and the final report drafted for the coordinating group by Dr E Hey (Newcastle).
We thank all the families for their help and cooperation, and the paediatric staff of the region for their unwavering support of their nursing colleagues. We are also grateful to Dr MI Ellis for her measurements of blood pressure in babies of more than 31 weeks of gestation. Regional Health Authority Maternity Survey staff provided free office facilities.