Article Text

Abstract
AIM To determine whether abnormal transvascular protein flux can be measured with positron emission tomography (PET) in neonates with respiratory distress syndrome (RDS).
METHODS Fourteen infants with normal gas exchange (non-RDS group) underwent one PET measurement and 12 infants with RDS (the RDS group) underwent two measurements of protein flux, as determined by the pulmonary transcapillary escape rate for68Gallium labelled transferrin (PTCER).
RESULTS The mean PTCER for the RDS infants (132 ± 39 10-4/min) was significantly greater than that for infants without RDS (75 ± 27 10-4/min). PTCER did not change between measurements in the infants with RDS, including five who received and responded to surfactant replacement between the two scans.
CONCLUSIONS Increased transvascular flux of large molecular weight proteins complicates RDS in preterm infants. PET provides a tool with which to evaluate the processes that contribute to pulmonary dysfunction in neonates.
- respiratory distress syndrome
- positron emission tomography
- pulmonary vascular permeability
Statistics from Altmetric.com
Respiratory distress syndrome (RDS) in premature infants is caused by interacting pathophysiological processes which include alveolar collapse, ventilation–perfusion mismatch, and accumulation of extravasated proteins and water in the alveolar space.1Invasive studies in preterm lambs with RDS have shown enhanced protein flux through a disrupted endothelial–alveolar epithelial barrier.2 3 However, the lack of non-invasive, quantitative methods has limited the evaluation of protein flux in human neonates. The only in vivo study in neonates showed rapid clearance of an inhaled low molecular weight tracer, diethylene-triamine penta-acetate (DTPA, molecular weight 492 Daltons), from the lungs of infants with RDS, suggesting a disrupted alveolar epithelial barrier.4 None the less no in vivo human studies have estimated the flux of larger molecular weight proteins from the intravascular space into the extravascular space in preterm infants with RDS.
Using the nuclear medicine imaging technique of positron emission tomography (PET), the transvascular flux of transferrin, a protein with a molecular weight (79 550 Daltons) similar to albumin (69 000 Daltons), is increased in adults with the acute respiratory distress syndrome (ARDS).5-7 Furthermore,18[F]fluorodeoxyglucose uptake, a marker for neutrophil activity, was increased in PET studies of acute lung injury in newborn piglets undergoing high pressure ventilation.8 The success of PET in the assessment of pulmonary dysfunction in adults and the correlation between structure and function in animal studies prompted us to determine if PET could be used to detect increased protein flux in human neonates with RDS.9 10
Methods
Infants were recruited from the neonatal intensive care unit at St Louis Children’s Hospital. Two groups of infants were studied: non-RDS (n=14) comprising term or preterm infants with a normal respiratory rate, normal chest radiograph, and peripheral oxygen saturations >94% while breathing ambient air; and those with RDS (n=12), comprising preterm infants who required supplemental oxygen to maintain peripheral oxygen saturations >94%, and who had chest radiographs with diffuse granular infiltrates. No infants had positive blood cultures or a clinically detectable patent ductus arteriosus (PDA) at the time of the measurements. Two mothers received antenatal corticosteroids, one in the non-RDS group and one in the RDS group. The non-RDS infants underwent one PET scan within the first 4 days of life. In an effort to decrease the possible influences of longer term mechanical ventilation on the PET physiological measurements, all but two RDS infants underwent two PET scans at least 6 hours apart within the first 24 hours of life. Five infants received surfactant replacement between the two scans.
Informed consent was obtained from the parents, and permission was obtained from the bedside care providers. Historical and clinical data were obtained from the mothers’ and infants’ records. The protocol was approved by the Washington University Human Studies Committee and the Washington University Radioactive Drug Research Committee.
PET scans were performed at the Washington University Clinical PET Facility under medical and nursing supervision. A Siemens 953B/47 high resolution tomograph (6 mm in-plane resolution and 3 mm slice thickness) was used for all measurements. The infant was placed supine with the thorax positioned in the middle of the field of view. Attenuation correction was determined for each subject by obtaining a 10 minute transmission scan with an external ring source of68Germanium-68Gallium.
Permeability was measured after intravenous injection of 35 microCurie/kg of 68Gallium (68Ga) citrate. This dose provides an effective radiation dose equivalent (EDE) of 189 mrem. (For comparison, annual background radiation in St Louis is 300 mrem per year, a standard nuclear renal scan using 99mTechnetium provides an EDE of 230 mrem, and a computed tomogram of the chest provides an EDE of 1000 mrem). The 68Ga binds rapidly to native transferrin and has a molecular radius and permeability properties similar to that of albumin.11 Serial emission scans were obtained for 30 minutes, beginning 2 minutes after tracer injection. The tracer activity within the cardiac blood pool and the lungs was measured on each emission scan. Subsequently, time–activity curves were constructed from the blood and tissue measurements and were analysed with a two compartment mathematical model. From this model, a rate constant, k1, for flux of labelled transferrin from the intravascular to the extravascular compartment was calculated.12 Because protein flux is affected by surface area available for exchange, k1 was normalised for regional blood volume, which is an approximation of the microvascular surface area. Regional blood volume is calculated from the distribution of activity in the first minutes after tracer injection, when virtually all tracer activity is in the intravascular compartment.12 13 This volume normalised rate of protein flux is a measure of pulmonary vascular permeability, termed the pulmonary transcapillary escape rate (PTCER) for 68Ga-labelled transferrin, and is expressed in units of 10-4/min.
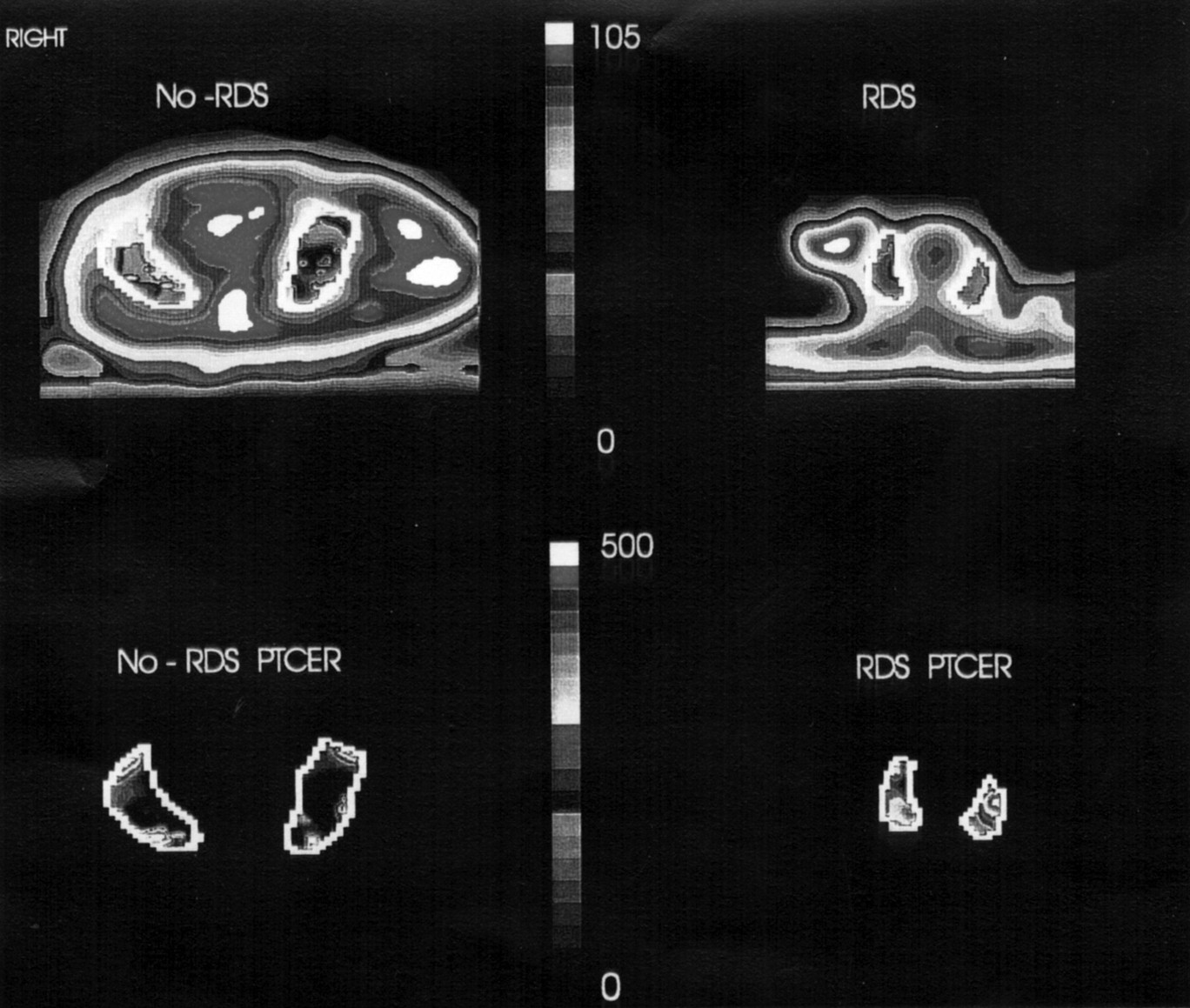
To analyse the PET data, regions of interest were defined within the lung fields on multiple tomographic slices of the transmission scan (fig 1). In defining the regions of interest, care was taken to avoid the heart, surrounding major vessels, and chest wall. The regions were then superimposed on the PTCER images. As no systematic slice to slice or side to side differences were present, a single mean value per subject was calculated. Representative tomographic images of PTCER from one non-RDS infant and one RDS infant are also shown.
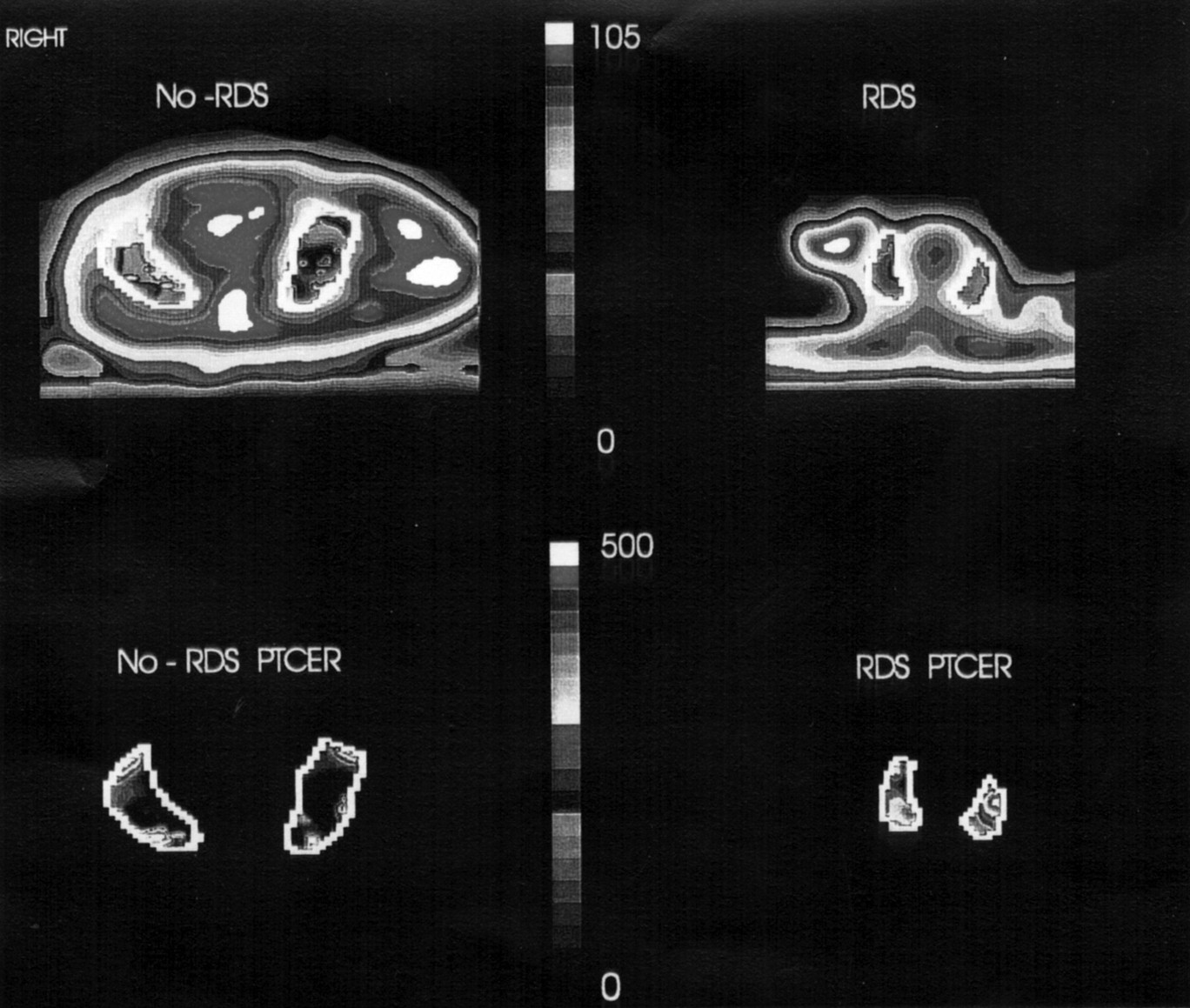
Representative transverse PET images of a transmission scan (top row) and pulmonary vascular permeability (PTCER, bottom row) in infant without RDS (left hand panels) and an infant with RDS (right hand panels). The infant is supine, with the right side on the left of the image. The difference in size between the two images reflects the smaller size of the preterm RDS infant. Brighter areas represent greater protein flux in the PTCER image. PTCER values on the right and left sides were 27 and 31 10-4/min for infant without RDS and 274 and 279 10-4/min for the RDS infant.
The in vivo binding of 68Ga to transferrin was measured in three infants. Two hundred microlitres of serum, obtained 10 minutes after injection of the tracer, were centrifuged at 1000 × g in a Centrifree micro-partition tube (Amicon Inc., Beverly, MA) with a 30 000 molecular weight cutoff filter. A gamma counter then measured the fraction of 68Ga which was bound to proteins with molecular weight > 30 000. For these three infants, 99.7 (0.3)% of the 68Ga was protein bound.
Repeated measures analysis of variance using the Statistical Analysis System for PC based systems (SAS, Inc., Cary, NC) was performed to evaluate differences between mean values. Results are expressed as mean (SD). Correlations between variables were analysed using standard linear regression methods, also with SAS. P ⩽ 0.05 was regarded as significant.
Results
The clinical and PTCER data for the infants without RDS are given in table 1. Their gestational ages ranged from 28 to 40 weeks and age at the time of PET scan ranged from 12 to 90 hours. Infants 11 and 12 were mechanically ventilated at the time of the scan. The mean (SD) PTCER for this group was 75 (27) 10-4/min (fig 2). To determine whether PTCER was influenced by gestational age or chronological age, we compared the PTCER measurements between non-RDS infants who were less than 37 weeks gestation with those who were 37 weeks gestation or greater. We also compared measurements between infants who were 24 hours of age or less with those who were greater than 24 hours of age (data not shown). No differences in PTCER were found with any of these comparisons.
Clinical and PET data for non-RDS infants

{kind=link}
{kind=link}
Plots of individual and mean (SD) PTCER values for non-RDS and RDS infants. * Mean PTCER for scan 1 for infants with RDS was significantly greater than that for those without (p=0.001), but not different from scan 2 (p=0.07). Open circles represent infants who received surfactant replacement between scans.
The clinical and PTCER data for the RDS infants are presented in table2. All infants with RDS were less than 37 weeks of gestation, 24 hours of age or less, and were receiving conventional mechanical ventilation (except one infant who was receiving nasal cannula oxygen). Infants did not require pharmacological support for blood pressure nor had they clinical evidence of a patent ductus arteriosus. One infant was extubated by the time of the second scan.
Clinical and PET data for infants with RDS
Individual PTCER data are presented in fig 2. The mean PTCER for the 12 RDS infants at the first measurement was 132 (39) 10-4/min, which was significantly greater than the mean PTCER for the non-RDS infants (p=0.001). PTCER for the RDS infants was also significantly greater than that for the nine non-RDS infants who were less than 37 weeks of gestation (p=0.003). Individual changes in PTCER occurred between the two scans, but as a group, these were not significant (p=0.07) (fig 2). The arterial:alveolar oxygen ratio did not change significantly (p=0.25). For the five infants who received surfactant, the a:A ratio increased by 70% (p=0.05), but the mean PTCER did not change between the two scans (149 (41) to 200 (18) 10-4/min; p=0.08 ).
In infants with RDS, PTCER did not correlate with gestational age, severity of disease on chest radiograph, mean airway pressure, or the a:A ratio. For individual infants, the change in PTCER did not correlate with the change in a:A ratio (data not shown). All study infants survived and none required supplemental oxygen at 28 days of life.
Discussion
This study represents the first application of PET to evaluate pulmonary vascular permeability in human neonates. Previous studies in adults and mature animals have demonstrated the structure–function correlations that support the PET measurement of PTCER.9 10 We were unable to make histological correlates in this current study, but the similarity of our PET physiological measurements to these previous studies suggests the feasibility of applying this technique to neonates.
Differences in pulmonary circulatory physiology between neonates and adults should not affect the PET measurement of PTCER. First, although pulmonary vascular permeability is influenced by the vascular surface area available for exchange, the PTCER is normalised for blood volume, a marker of surface area, thus taking into account the difference in vascular surface area between neonates and adults. Second, pulmonary blood flow and tracer delivery to the lungs may be different between neonates and adults. Under normal conditions, the vascular concentration of radioisotope is independent of pulmonary blood flow unless the perfusion is severely compromised.12 13 Under these conditions, which can be detected by examination of the individual time–activity curves, blood volume is underestimated, leading to an overestimation in PTCER. All time–activity curves suggested that the equilibrium state for tracer delivery was achieved by the start of the scans. For these same reasons, blood flow through a patent ductus arteriosus would not affect interpretation of the measurements. Thus methodological issues arising with performing PET measurements of pulmonary vascular permeability should not be affected by physiological differences between neonates and mature humans or animals.
The PTCER values for infants with RDS were comparable with those for adults with ARDS, pneumonia, and interstitial lung disease using similar techniques.6 7 14 In preterm infants with RDS, a quantitative deficiency of surfactant may lead to secondary disruption of the endothelial–epithelial barrier. The studies of Jefferieset al, mentioned previously, as well as the identification of surfactant protein-A (molecular weight 35 000 Daltons) in the blood of premature infants with RDS provide evidence for loss of integrity of the alveolar epithelial–endothelial barrier and net flux from alveolus to vascular space.4 15 In addition, studies in preterm lambs with RDS have shown a bidirectional leak of radiolabelled albumin.2 Indirectly, the presence of hyaline membranes, on histological examination of lung tissue, suggests a vascular–alveolar protein leak. To our knowledge, our PET studies are the first in vivo measurements in humans which demonstrate net protein flux from the vascular to the extravascular space.
Those infants with RDS who received surfactant showed an improvement in oxygenation following treatment that was not reflected by a decrease in the PTCER. However, previous studies in which premature lambs treated early with surfactant had lower pulmonary vascular permeability than untreated lambs suggested that surfactant treatment may have a direct influence on pulmonary vascular permeability.16 17 These observations taken together suggest that surfactant treatment may prevent the endothelial or epithelial injury which initiates the protein leak, but surfactant does not attenuate the leak once it has occurred, perhaps explaining the failure of surfactant treatment in some infants with RDS.18
The PET measurement of PTCER provides a non-invasive method for evaluating lung injury that may be associated with increased pulmonary vascular permeability. Animal studies have suggested a correlation between PTCER and histological or ultrastructural indices of lung injury.9 10 However, human studies, ours included, have not shown a correlation between PTCER and clinical indices of disease severity. These clinical indices are a reflection of the degree and duration of vascular leak, the presence of atelectasis, and ventilation–perfusion relations, among others. Thus the development of additional metabolic tracers should permit a comprehensive in vivo evaluation of other physiological processes that may contribute to newborn pulmonary dysfunction and will help delineate mechanisms of lung injury and response to treatment.
Acknowledgments
An abstract based on these data was presented at the Society for Pediatric Research Meeting, 2-5 May 1994 (Pediatr Res1994;35:346A).
This work was supported in part by a grant from the American Lung Association of Eastern Missouri (AH).
We thank Drs Daniel P Schuster and F Sessions Cole for their thoughtful comments, Dr Barry Siegel for access to the clinical PET facility, and Dawn Rouse for secretarial assistance.