Article Text

Abstract
AIM To measure changes in cerebral haemodynamics over the first three days of life in very preterm infants with normal brains.
METHODS Eleven mechanically ventilated infants (median gestational age 26 weeks) without evidence of major abnormalities on cranial ultrasound examination were studied. Cerebral blood flow (CBF) and cerebral blood volume (CBV) were measured using near infrared spectroscopy at least twice over the first three days of life.
RESULTS Cerebral blood flow increased significantly with time (p=0.02; stepwise linear regression) and this was independent of mean arterial blood pressure, PaCO2, and haematocrit.
CONCLUSION This change is likely to represent a normal adaptive response of the cerebral circulation to postnatal life.
- cerebral blood flow
- cerebral haemodynamics
- near infrared spectroscopy
- extremely preterm
Statistics from Altmetric.com
Periventricular haemorrhage and hypoxia–ischaemia are the most common causes of disabling brain injury in very preterm infants, and the pathogenesis of both types of injury is likely to be associated with abnormalities of cerebral perfusion in the critical first few days after delivery. An early study by Lou et al 1showed an increased risk of neurodevelopmental abnormalities in infants with cerebral blood flow (CBF) of less than 20 ml/100 g/min measured a few hours after birth. More recent studies have shown that intact survival is possible despite CBF measurements lower than 10 ml/kg/min,2 3 and the critical minimum level of CBF required to maintain cellular integrity has not yet been defined. Improvements in neonatal intensive care, leading to a reduction in cerebral injury, will depend on a better understanding of the normal adaptive changes of the cerebral circulation during the most vulnerable period, the first three days of life.4
The aim of this study was to define normal changes in global CBF and cerebral blood volume (CBV) by making repeated measurements with near infrared spectroscopy in a group of very preterm infants with apparently normal brains, during the first three days of life. The infants selected for study were undergoing intensive care, but were of appropriate weight for gestational age and had no evidence of significant antenatal or perinatal brain injury on the basis of cranial ultrasound appearances.
Methods
Eleven very preterm infants undergoing intensive care in the neonatal unit at University College London Hospitals Trust were studied. Their median gestational age was 26 (range 24–31) weeks and the median birthweight was 825 (range 637–1460) g. All infants were appropriately grown for gestational age (birthweight above the 10th centile). Seven had normal cranial ultrasound imaging at the time of study and on subsequent examination, three had small intraventricular haemorrhages which were first observed on the second day of life and which subsequently resolved, and one had mild ventricular dilatation by term with no evidence of preceding haemorrhage. Clinical details of the study infants are given in table 1. Each infant was intubated for resuscitation shortly after birth, and ventilated with supplementary oxygen. When studied, all infants were receiving conventional mechanical ventilation via an endotracheal tube, and physiological variables including mean arterial blood pressure (MABP) and transcutaneous carbon dioxide tension were monitored continuously during each study. Small transient fluctuations in FIO2were induced by the research staff (JM and LT) for the measurement of CBF and CBV, but the ventilator settings and the clinical management of each infant was the responsibility of the attending clinicians in the neonatal unit. Each infant was studied on two or more occasions during the first three days of life, and none of the studies started within an hour of the administration of surfactant. The study was approved by the hospital research ethics committee and informed consent was obtained from one or both parents of each infant before enrolment.
Clinical details of study infants
Simultaneous measurements of arterial saturation (SaO2) were obtained, using a pulse oximeter (Nellcor N200), and of MABP, using a transducer in an indwelling umbilical or peripheral arterial catheter (HP 78834A, Hewlett Packard), or by an oscillometric technique using an inflatable cuff (Dinamap 1846SX, Critikon). Continuous estimates of arterial oxygen tension (PaO2) and carbon dioxide tension (PaCO2) were obtained using a transcutaneous monitor (Hewlett Packard 3428G03410) calibrated with arterial blood gas samples. The arterial haemoglobin concentration and haematocrit of each infant were measured on the day of each study. Cranial ultrasound scans (Ultramark 4, Advanced Technical Laboratories, Letchworth, UK) were performed daily for the first week of life and then weekly until term or discharge from hospital.
The theory of near infrared spectroscopy has been described in detail elsewhere.5 In brief, it depends on the relative transparency of biological tissue to near infrared light, and the absorption of light by oxyhaemoglobin (HbO2) and deoxyhaemoglobin. A modification of the Beer Lambert law is used to convert measured changes in optical density to changes in chromophore concentration. In this study measurements were obtained using a commercial spectrophotometer (NIRO500 or NIR1000, Hamamatsu Photonics KK, Japan). Near infrared light from four (NIRO500) or six (NIR1000) laser diodes was transmitted via a fibre optic bundle to an “optode” on the tempero-parietal or frontal region of the infant’s head. A detecting optode placed 4–5 cm away on the opposite side of the head was connected to a second fibre optic bundle which conveyed the emerging light to the spectrophotometer. A controlling computer converted the changes in optical density into changes in cerebral [HbO2] and [Hb] while simultaneously recording SaO2, MABP, PaCO2 and heart rate.
Cerebral blood flow was determined from the Fick principle, using HbO2 as an intravascular tracer.6 A rapid rise (over 2 to 5 seconds) in SaO2 was induced by a step increase in FIO2. Cerebral blood flow in ml/100 g/min was then calculated from the integral of the saturation rise and the rate of rise of tracer concentration using the equation:
Cerebral blood volume was measured using the indicator dilution technique with a slow small change (over 1 to 2 minutes) in arterial oxygen saturation within the range 92% to 98% by manipulation of the FIO2 and determining the resulting change in [HbO2] concentration. CBV was then obtained from the equation: CBV=κ.Δ[HbO2]/(ΔSaO2×H×R)7 where R (0.69) is the large vessel:cerebral haematocrit ratio. As it was not possible to induce a suitable change in SaO2 in infants who were ventilated either in air or in 100% oxygen, no measurements were attempted in these infants.
On each day of the study six measurements of CBF were attempted. Only those measurements were accepted that met previously established criteria for the stability of parameters such as the PaCO2, MABP, and [Hb + HbO2] during the measurement, and the stability of the SaO2 before the measurement.8The mean value of all the measurements which met the acceptance criteria was calculated on each day. Similarly, six measurements of CBV were attempted each day. The number of successful measurements of both CBF and CBV on each day ranged between two and six, although one infant had no acceptable CBV measurements on day 2.
As part of ongoing follow up, infants were assessed between 12 and 18 months of corrected age. The assessment included both medical and structured neurological examinations9 and were carried out by a paediatrician blind to the results of the near infrared spectroscopy studies. Particular attention was paid to hearing and visual responses. Infants were categorised according to the presence or absence of neurological impairments from the results of these examinations. The impaired infants were further subdivided into those with and those without functional disability. Impairments without disability between 12 and 18 months of corrected age were usually subtle abnormalities of tone, posture, or reflexes.10
As the distributions of CBF each day were positively skewed, the logarithm of the values was used for further analysis. The dependence of log CBF and CBV on time, PaCO2, MABP, haematocrit, infant number and gestational age were tested using stepwise multiple linear regression analysis (Sigmastat version 2.0, Jandel, California, USA).
Results
Six out of 11 infants had satisfactory measurements on each day of the study, and the remainder were studied on two out of the three days. Figure 1 shows CBF for each infant compared with postnatal age. Stepwise multiple linear regression analysis (using a dummy variable for each infant) demonstrated the dependence of log CBF on time (p=0.02) and gestational age (p<0.001), but not on PaCO2, MABP, haematocrit or infant number.

Variation in CBF with postnatal age: symbols indicate individual infants.
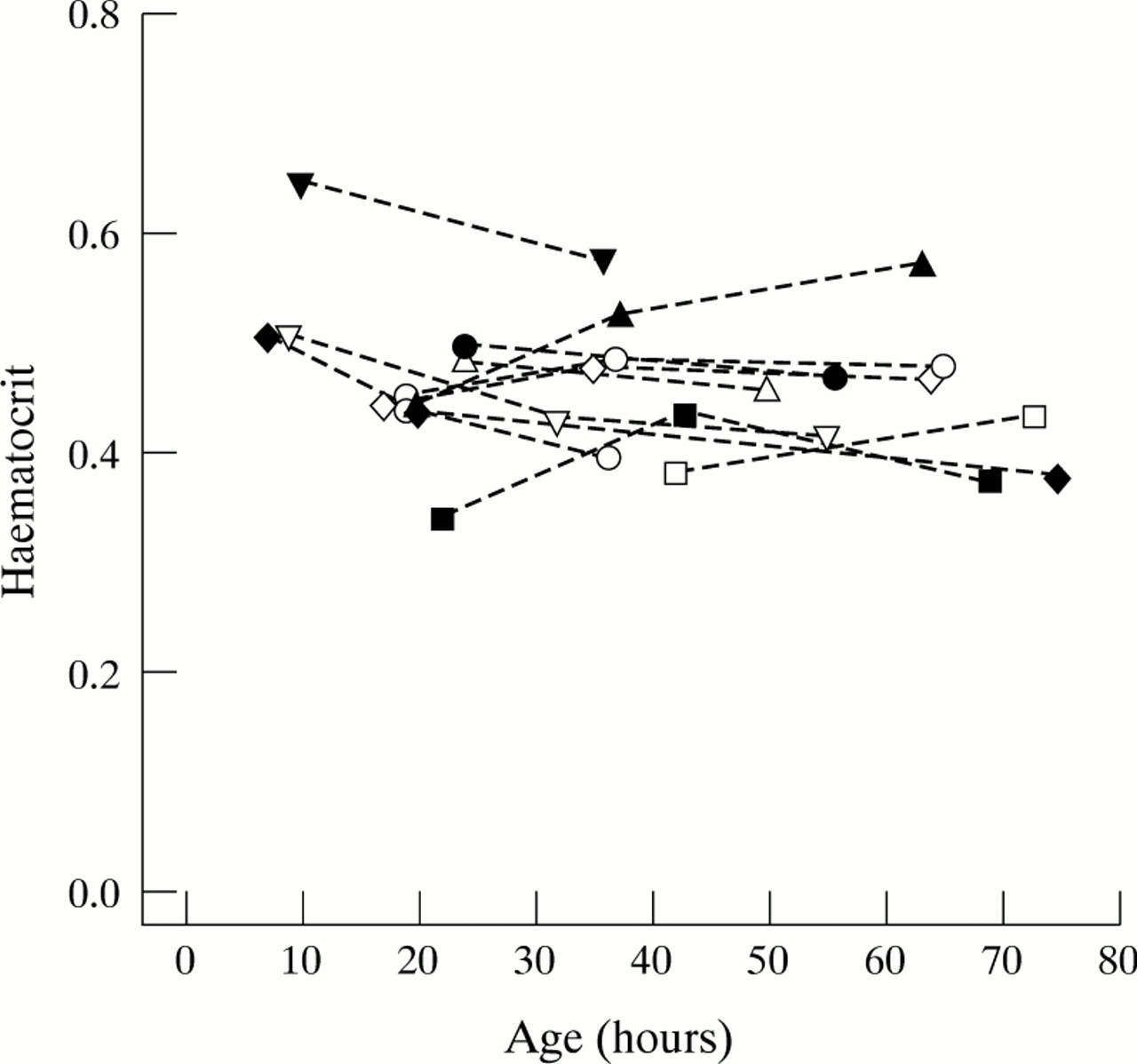
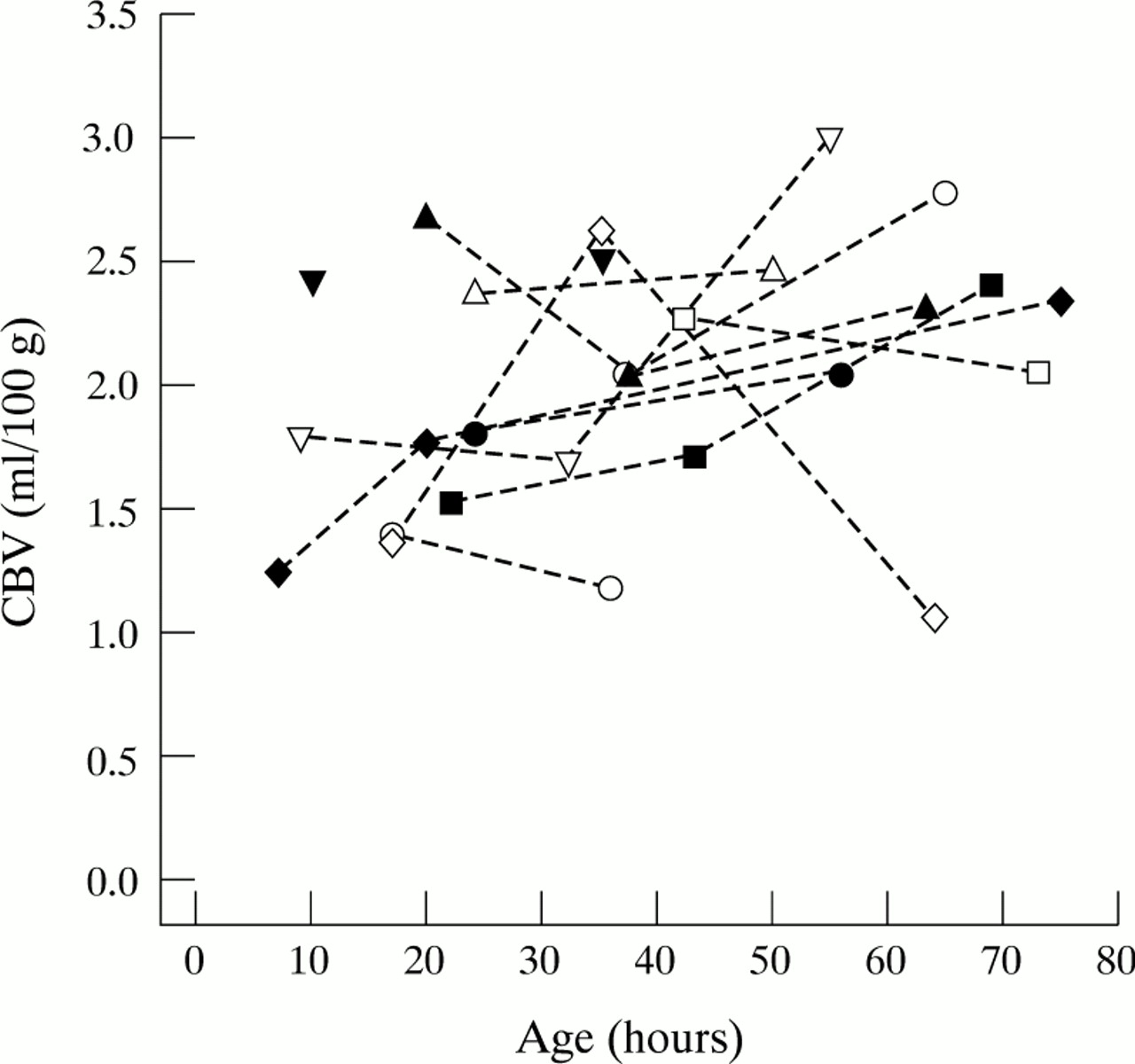
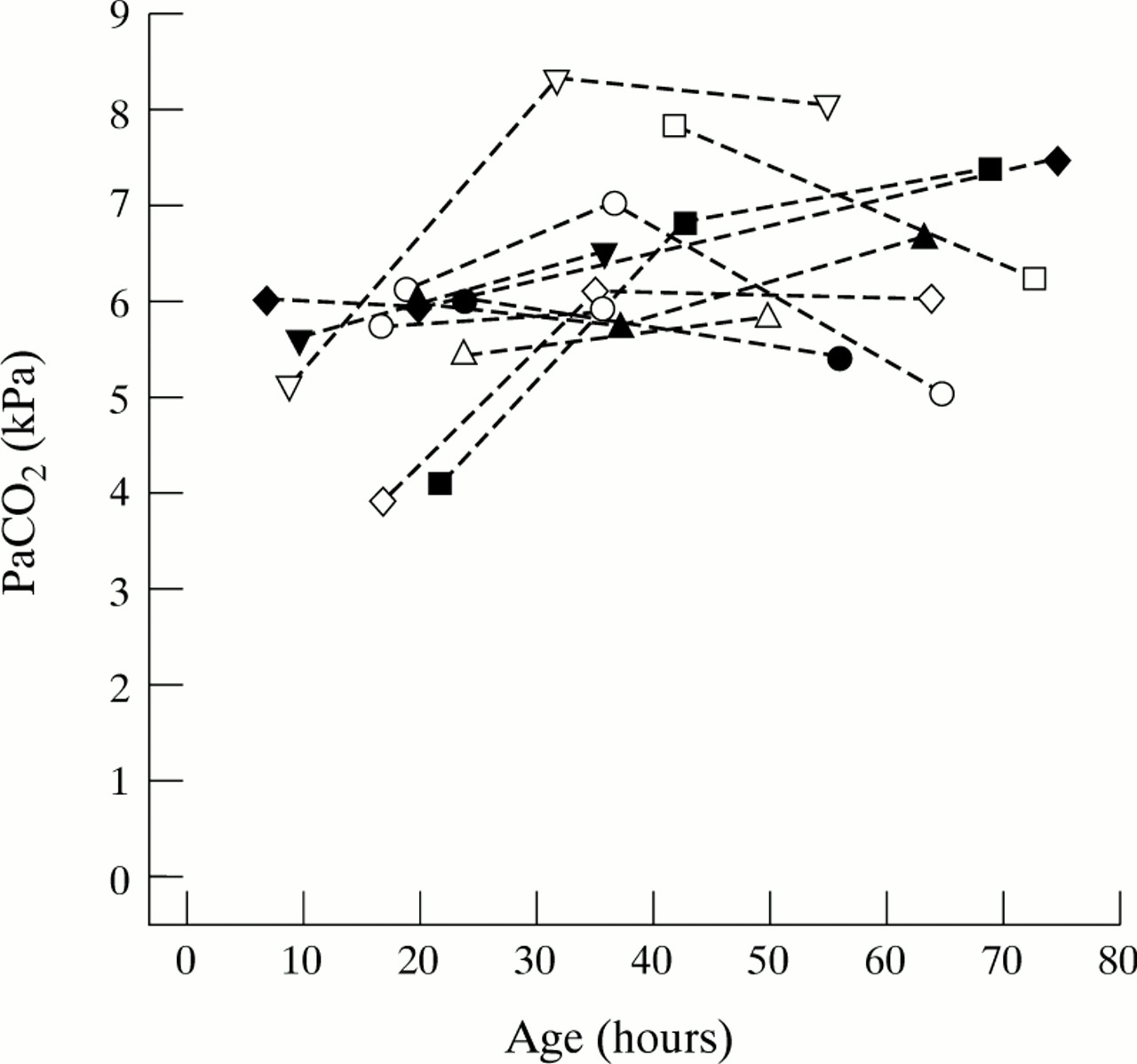
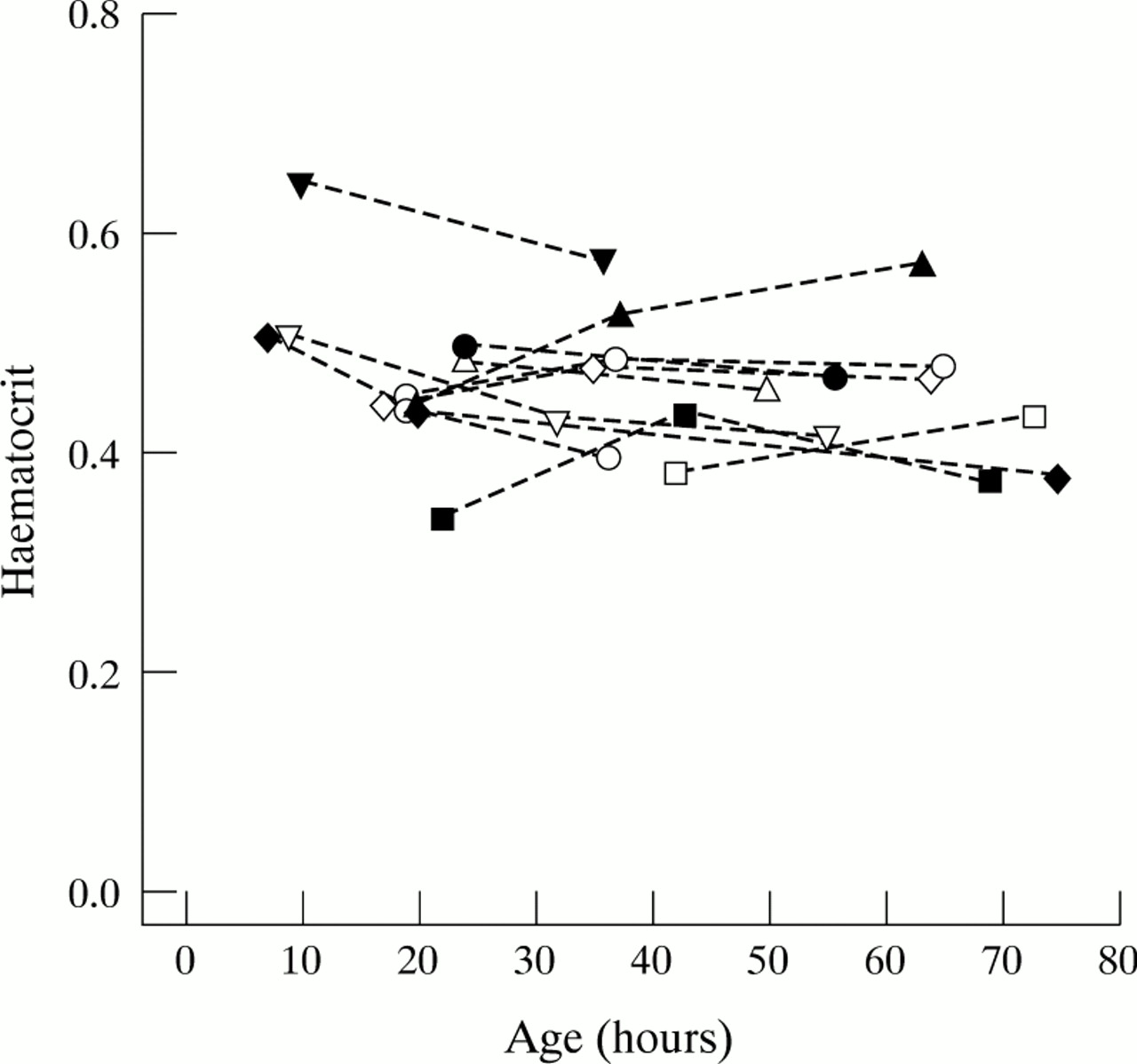
Five out of 11 infants had satisfactory measurements of CBV on each day of the study, five on two days, and one on a single occasion. The variation of CBV with time is shown in fig 2. There was no relation of log CBV with time or any physiological variable. Figs 3-5 show the variation of PaCO2, MABP, and haematocrit with time. The ventilator settings (mean airway pressure and FIO2) were not significantly different over each of the three days.

Variation in CBV with postnatal age.
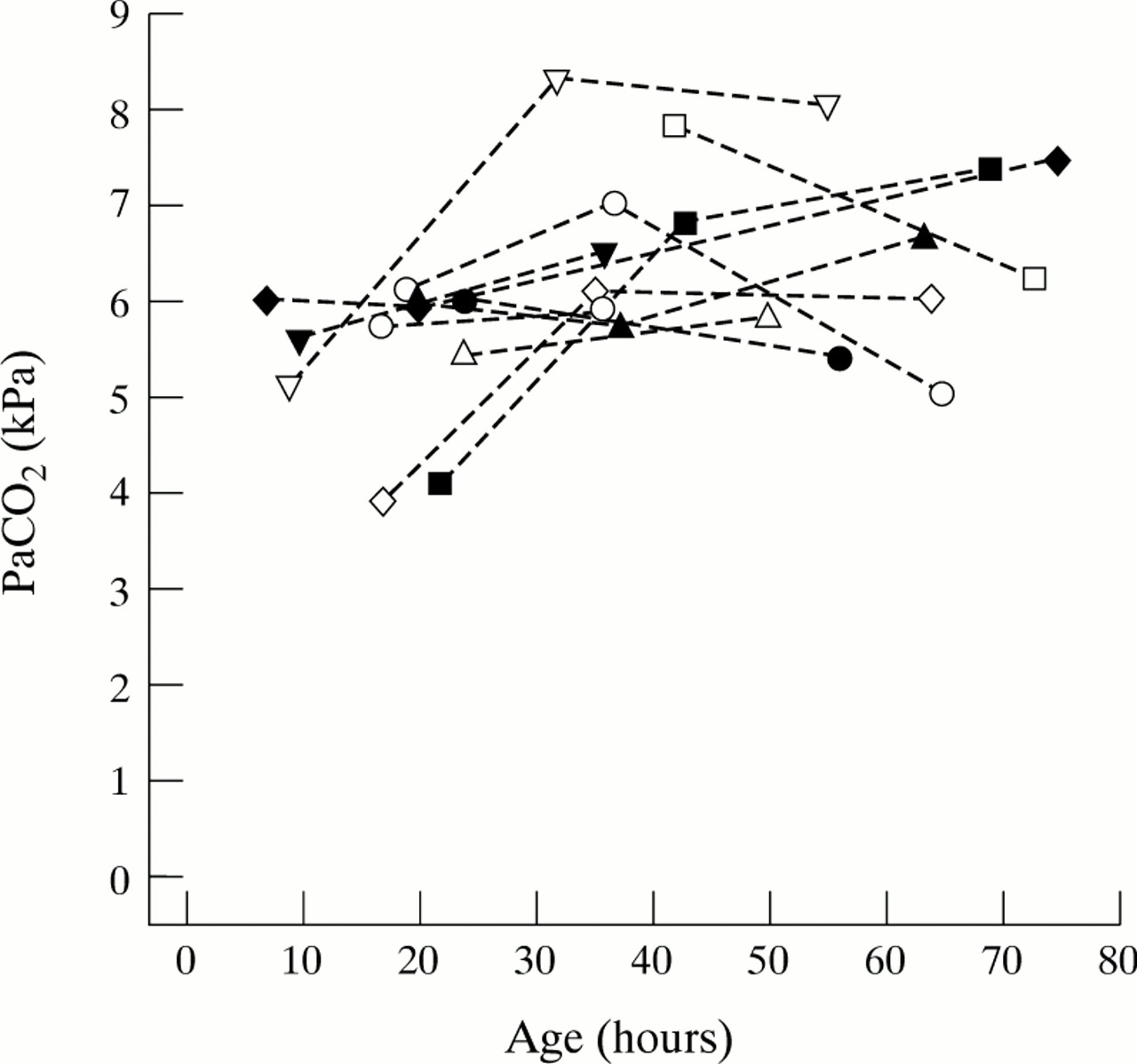
Variation in PaCO2 with postnatal age.

Variation in MABP with postnatal age.
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Variation in haematocrit with postnatal age.
All infants had normal brains on cranial ultrasound examination at a corrected age of term, or before discharge from the neonatal unit, except case 9, who had mild ventricular dilatation. This infant had an unusually high CBF and CBV on day 2.
Nine out of 11 infants were examined between 12 and 18 months of age (corrected for prematurity) and no disabling neurodevelopmental abnormalities were detected, although three infants displayed subtle abnormalities of tone. One infant died of necrotising enterocolitis and one was lost to follow up. The outcome data are summarised in table 1.
Discussion
The range of CBF we observed during the first 24 hours was wide (6.3–15.2 ml/100 g/min), comparable with values measured by Pryds in the first 2 hours of life using the Xenon clearance technique (5.2–18.7 ml/100g/min).11 Altman obtained a range of 4.7–17 ml/100 g/min using positron emission tomography (PET) in preterm neonates 1 to 6 days old.2 The coefficients of variation among subjects were of 34%, 41%, and 31% on the three consecutive days, comparable with that of 34% measured in adults using near infrared spectroscopy.12
There is no gold standard method of measuring CBF in human neonates. The near infrared spectroscopy technique has been compared with the intravenous 133Xenon clearance method in human neonates undergoing intensive care.13 14 Good correlations were observed between the two methods except at high values of CBF where the near infrared spectroscopy estimate of CBF was slightly lower than that obtained by the Xenon method. Near infrared spectroscopy is non-invasive and repeatable, but cannot be used to measure CBF when infants are ventilated either in air or 100% O2, when it is not possible to make small changes in SaO2 by adjusting the FIO2. This resulted in some infants being studied only on two out of the three days.
The technique of measuring CBV has not been validated independently in human newborns, but the values of CBV we obtained are similar to those observed using PET.2 Although some discrepancies have been observed in CBV measurements following a change in PaCO2, 15 there is no evidence of systematic errors which would invalidate the measurements we obtained.
We have shown a significant rise in CBF over the first three days of life in very preterm infants undergoing intensive care, consistent with measurements using the Xenon clearance method.16 Doppler ultrasound measurements of cerebral artery velocities have demonstrated an initial decrease over the first 5 hours of life, followed by a gradual increase.17 18 However, these velocity measurements are hard to interpret because of the possibility of alterations in the diameter of the insonated vessels.
Our results strongly suggest that the increase in CBF represents a normal adaptive response of the cerebral circulation to postnatal life rather than being a direct result of changes in MABP, PaCO2, or haematocrit. Measurements of CBF using the Xenon technique have suggested that the increase with postnatal age is correlated with changes in PaCO2 and is inversely correlated with blood haemoglobin concentration.16 Other studies have suggested that CBF is also determined by the oxygen affinity of the circulating haemoglobin19 and by the oxygen tension achieved at resuscitation after delivery.20In this study haemoglobin concentration was not used as an independent variable, being part of the denominator of the equations used to calculate CBF and CBV. Therefore, the haematocrit was used as a physiological variable related to CBF. We found no independent association between CBF and haematocrit. The viscosity of blood is generally thought to vary inversely with haematocrit. Linderkampet al 21 have measured the viscosity of blood samples from newborn infants with gestational ages between 24 weeks and term, using glass tubes of varying diameters. They showed that for a given haematocrit the viscosity varies with both the tube size and the gestational age of the neonate. Therefore, the expected contribution of changes in haematocrit to the increase of CBF with time in a group of neonates of different gestational ages is uncertain. CBF was inversely related to gestational age, but the importance of this finding in a small group of subjects is doubtful. MABP in the group did not increase with postnatal age, contrary to trends noted in other studies.16 This may have been a reflection both of the small sample size, and of the policy in our unit of tolerating relatively low blood pressures in infants who are clinically well perfused. CBF was independent of MABP, suggesting that autoregulation of the cerebral circulation was intact in this group of infants. The rise in CBF with time was not associated with an increase in CBV, indicating a reduction in transit time.
The increase in cerebral perfusion with time is likely to be due to an increase in left ventricular output, coupled with a reduction in cerebrovascular resistance. An increase in left ventricular output has been observed in term neonates studied over the first few days of life by Doppler echocardiography,22 23 although there is evidence that the presence of lung disease can affect the time course of this change.24 Increasing left and right ventricular outputs have also been seen in premature ventilated infants,25 with low cardiac outputs related to higher mean airway pressures and larger ductal shunts. The rise in cardiac output may be a consequence of lowered peripheral vascular resistance in several organs including the brain.
The resulting increase in CBF is seen in infants with normal brains, and further studies are under way to investigate whether deviations from this response are associated with an increased risk of perinatal brain injury.
Acknowledgments
This work was supported by a grant from the United Kingdom Medical Research Council.
We thank Professor David Edwards, Ms Jan Townsend, and Drs Ann Stewart, Simon Roth, David McCormick and Vincent Kirkbride for their contribution to this work.