Article Text

Abstract
BACKGROUND The increased incidence of neurological deviations in preterm infants with chronic lung disease (CLD) has been linked to severe brain haemorrhage (intraventricular haemorrhage (IVH)) and periventricular leucomalacia (PVL) rather than to CLD per se.
AIM To evaluate whether CLD without concomitant brain lesions constitutes a risk factor for adverse developmental outcome.
METHOD Forty three very low birthweight infants with CLD, but without IVH or PVL, and 43 very low birthweight infants without CLD, IVH, or PVL were evaluated at 5 and 10 months of corrected age using the movement assessment of infants (MAI) scale. The Griffiths' developmental test was carried out at 10 months of age.
RESULTS The overall motor assessments (MAI) in infants with CLD and controls were not significantly different. However, differences were observed in the execution of volitional movements (MAI), the total sum, hand and eye coordination, and perception and intelligence (measured by the performance scale of the Griffiths' test).
CONCLUSIONS CLD has a deleterious effect on the control of hand and eye coordination and on perception and intelligence. These results thus re-emphasise the necessity for careful neurodevelopmental follow up of infants with CLD whether or not they suffered IVH or PVL.
- chronic lung disease
- neurodevelopment
- motor assessment of infancy (MAI)
- Griffiths' test
- preterm
Statistics from Altmetric.com
About 30% of very preterm infants suffer from chronic lung disease (CLD). The incidence of neurological sequelae in infants with CLD has recently been reported to be much higher than among very low birthweight infants without chronic lung complications (40% compared with 6% respectively).1 However, the impaired development of infants with CLD has been linked to intraventricular haemorrhage (IVH) and/or periventricular leucomalacia (PVL) rather than to lung disease per se.2-5 Infants with CLD experience frequent episodes of hypoxaemia in association with periods of desaturation6-9 as well as suboptimal respiratory mechanics.10 It can be assumed that such hypoxaemic episodes can impair the development of motor and mental functions.11 ,12 It has been recently shown that CLD per se has an unfavourable effect on motor performance at 3 years of age, and neurological neonatal risk factors and social class have a negative effect on mental development.13
The objective of this study was to determine whether CLD per se is associated with suboptimal development during the first year of postnatal life. We also examined the possibility that development of a particular skill(s) may be impaired by CLD.
Methods
SUBJECTS
The study population was extracted from 291 very low birthweight infants who were born in Stockholm County and required neonatal intensive care at the Karolinska Hospital during the period September 1988 to March 1993. Seventy of these infants suffered from CLD and were thus eligible for the study. Seven of these died during the neonatal period. Of the 63 survivors with CLD, 12 also suffered from severe IVH and PVL. Eight infants could not be examined because of other medical problems including congenital cardiac malformation (one), hepatitis C (one), immobilisation of the legs (pes adductor; one), a severe visual defect (one), and severe cerebral infarction (one). The final study group thus contained 43 infants. These infants were evaluated by movement assessment of infancy (MAI). Five infants from the CLD group could not be tested by the Griffiths' test because of various medical and/or social problems. Thus the Griffiths' test was performed on 38 of the 43 infants with CLD.
Selection procedure for the control group
A list of eligible control infants (excluding those with CLD, IVH > grade 2, and PVL) from the same population of 291 very low birthweight infants was arranged in ascending order of gestation. For each index case, a control infant was sequentially selected as the closest gestational age match. Pairwise matching was impossible because the infants with CLD were the least mature. As a result of this selection procedure, the gestational ages at birth and birth weights were similar in the two groups. Table 1 presents the neonatal characteristics of the study and control groups.
Data on the infant population and the prevalence of risk factors
As the Griffiths' developmental test was performed on 38 of the 43 very low birthweight infants with CLD, the control group consisted of 38 of the 43 control infants.
RISK FACTORS
CLD: diagnostic criteria
A diagnosis of CLD was based on the following criteria: (a) acute lung injury during the first week of postnatal life; (b) clinical signs of chronic respiratory disease; (c) a requirement for supplemental oxygen treatment for more than 28 days to maintain a Pao 2 of > 50 mm Hg; (d) a chest radiograph showing persistent strands of density in both lungs.14 ,15 CLD was divided into stages according to the criteria described by Toceet al.16 Four infants were diagnosed as having CLD of grade I, 16 as having CLD grade II, and 23 had CLD grade III.
IVH/PVL: diagnostic criteria (neonatal cranial ultrasonography)
During the neonatal period, the infants were examined by cranial ultrasonography at least three times: days 1–3, days 5–7, and more than two weeks after birth. Haemorrhages of the brain (IVH) were classified according to Papile's first three grades.17Changes in periventricular white matter echogenicity (W) were classified into four grades: W1, “flaire”, indicating subtle white matter echodensities; W2, distinct white matter echodensities; W3, cyst formation; W4, large intense echodensity (see Hesser et al 18 for details).
Infants with IVH and/or PVL grade > 2 were excluded from the study.
Maternal factors
Clinical chorioamnionitis: diagnosis based on the presence of fever and uterine tenderness and/or malodorous amniotic fluid and/or maternal/fetal tachycardia, elevated white blood cell count, and/or C reactive protein
Rupture of the membranes before the onset of labour.
Factors associated with the infant
Gestational age at birth
Birth weight
Apgar score at five minutes after birth
Growth retardation (small for gestational age); birth weight ⩽ −2SD
IVH grades 1–2 and PVL grades 1–2 (according to Papileet al 17)
Patent ductus arteriosus requiring ligation
Number of infections before the assessment.
MOTOR ASSESSMENT AT 5 AND 10 MONTHS OF CORRECTED AGE
Motor behaviour was evaluated by using a modified version of MAI.19 The original number of items was reduced to include only those reported to be the most valid as predictors of cerebral palsy.20 ,21 In addition, three other variables were examined: pull to sit (arms and legs), slip through, and Collis horizontal. The latter items are often used in clinical practice and are regarded as being a good measure of postural muscle activation.
Within the MAI scale, the items are grouped into four categories: muscle tone, primitive reflexes, automatic reactions, and volitional movements.
In the original version of the MAI scale, muscle tone items are rated from 1 to 6 (3 representing normal muscle tone, 1 and 2 representing hypotonicity, 4 and 5 representing hypertonicity, and 6 representing fluctuating tone), while the other items are scored from 1 to 4. To be able to include muscle tone more easily in the total score for each individual infant, the original grades were transformed here so that grade 3 became 0, original grades 2 and 4 were assigned a value of 1, and grades 1 and 5 were set equal to 2.
The examination was performed in accordance with the MAI manual by three experienced physiotherapists who were unaware of the group to which the infants belonged. The physiotherapists took turns with either physical examinations or gradings so that each of them performed a similar proportion of the tasks.
In the MAI scale, deviations are indicated by points: the higher the score, the worse the motor performance.
PSYCHOMOTOR DEVELOPMENT AT 10 MONTHS OF CORRECTED AGE
Psychomotor development was evaluated according to the Griffiths' development scale, and the results expressed in raw points. The Griffiths' test is widely used in Sweden and has been standardised for Swedish infants.22 It consists of five subscales as follows:
Locomotor function (A scale): crawling, sitting, raising oneself to an upright position, and walking
Personal-social competence (B scale): level of independence in daily life and general social competence
Hearing and speech (C scale): vocalisation, numbers and combinations of syllables, words used consistently with the same meaning
Hand and eye coordination (D scale): fine motor grasping
Performance (a perception and intelligence scale; E scale): the infant is given toys and instructions on how to use them.
Generally in this test, the higher the sum of the points, the better the overall performance.
ANALYSIS OF DATA
(a) The initial analysis involved testing for differences between infants with CLD and the control group with respect to: prevalence of small for gestational age infants, IVH grades 1–2, and patent ductus arteriosus requiring ligation (analysed using the χ2 test); and gestational age at birth, birth weight, Apgar score ⩽ 5 at five minutes after birth, and incidence of post discharge infections (analysed using one way analysis of variance). (b) The only statistically significant differences between the study and control group were with respect to the Apgar score (table 1). The possible influence of Apgar score ⩽ 5 at five minutes and the psychomotor score was thus examined using one way analysis of variance. (c) The difference in performance between infants with different grades of CLD was analysed using one way analysis of variance (Fisher's least significant difference procedure). (d) Consistency in motor performance was assessed as follows: at 5 and 10 months of corrected age the infants were grouped according to the total sum of scores from the MAI scale. Infants who performed below 25 percentiles were assigned to group 1, those who performed between 25 and 75 percentiles to group 2, and those above 75 percentiles to group 3. The analysis was based on the calculation of how many infants improved/deteriorated with age. Improvement was defined as “advancement” of the infant's performance from group 1 (the performance below 25 percentiles) at 5 months of age to group 2 or 3 (the performance between 25 and 75 percentiles or above 75 percentiles) or from group 1 to group 3 at 10 months of age. Deterioration was defined to have occurred when the infant's performance at 5 months of age was assigned to a higher group than at 10 months of age. (e) Possible differences between assessments performed by different examiners of each item and the sum of all items were tested by one way analysis of variance, in which all judgments by a specific physiotherapist were assigned to the same category.
Results
RISK FACTORS
Infants with CLD had significantly lower Apgar scores five minutes after birth than did those in the control group (p = 0.01; table 1). No other statistically significant differences in the prevalence of the risk factors between these two groups of infants were observed. Therefore subsequent analysis focused on the influence of the Apgar score and CLD on psychomotor development.
THE APGAR SCORE AND DEVELOPMENT
At 5 months of corrected age, infants with an Apgar score ⩽ 5 showed poorer performance of volitional movements (mean (SD) 3.73 (2)) than those with a higher Apgar score (2.3 (2)) (p = 0.01). However, these differences were no longer present at 10 months of corrected age (Apgar score ⩽ 5 −25.7 (6), Apgar score ⩾ 5 −22.7 (5), p = 0.11).
CLD AND MOTOR PERFORMANCE AT 5 AND 10 MONTHS OF CORRECTED AGE AS EVALUATED BY THE MAI SCALE
The overall motor performance, indicated by the sum of scores for all variables for infants with CLD and controls at 5 and 10 months of corrected age, was not significantly different at any age (p = 0.28 and p = 0.15 at 5 and 10 months respectively). At 5 months, the sum of grades were 38.5 (4), 39.2 (5), and 37.2 (5) for the infants with CLD I–II, CLD III and the control group respectively. At 10 months, the corresponding results were 62.6 (1), 64.4 (1) and 58.8 (7).
When the different categories of motor performance—that is, muscle tone, primitive reflexes, automatic reactions, and volitional movements—were analysed separately, CLD was found to be associated with a deviant volitional movement at 10 months of corrected age (23.8 (7), 25 (6), and 21.8 (3) for the infants with CLD I–II, CLD III and the control group respectively; p = 0.04). The most pronounced impairment in this respect was observed in infants with grade III CLD.
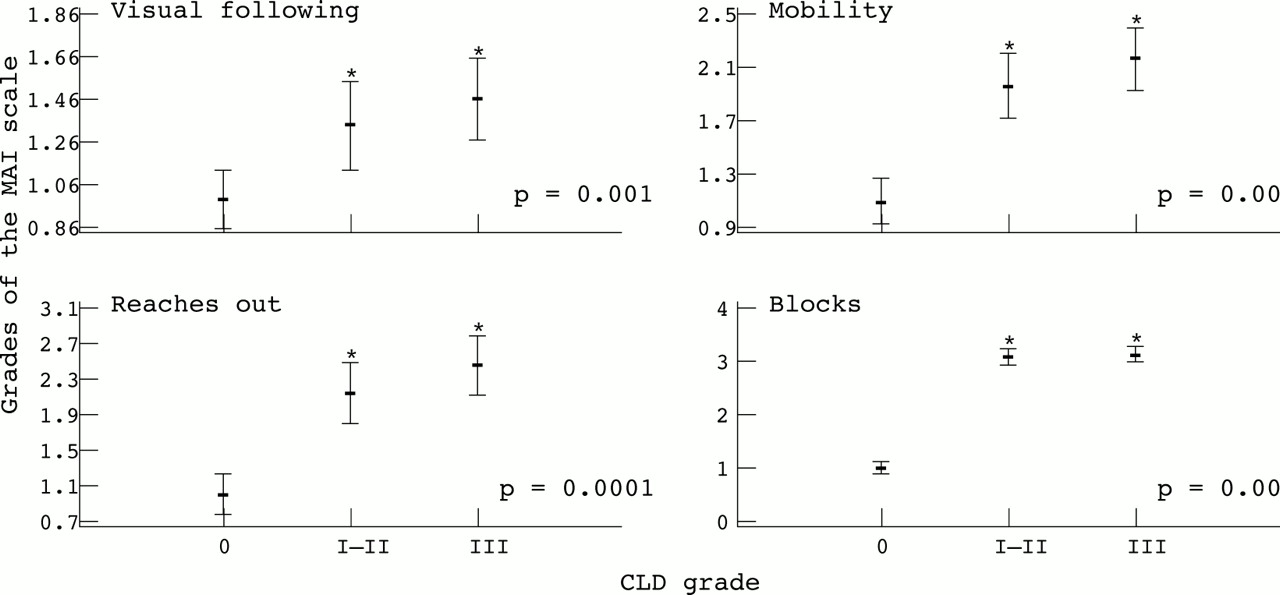
Of the 20 items belonging to the category of volitional movements, four in particular indicated impairment in infants with CLD (fig 1), but the degree of impairment was unrelated to the severity of the CLD—that is, there were no statistically significant differences between infants with CLD of different grades.
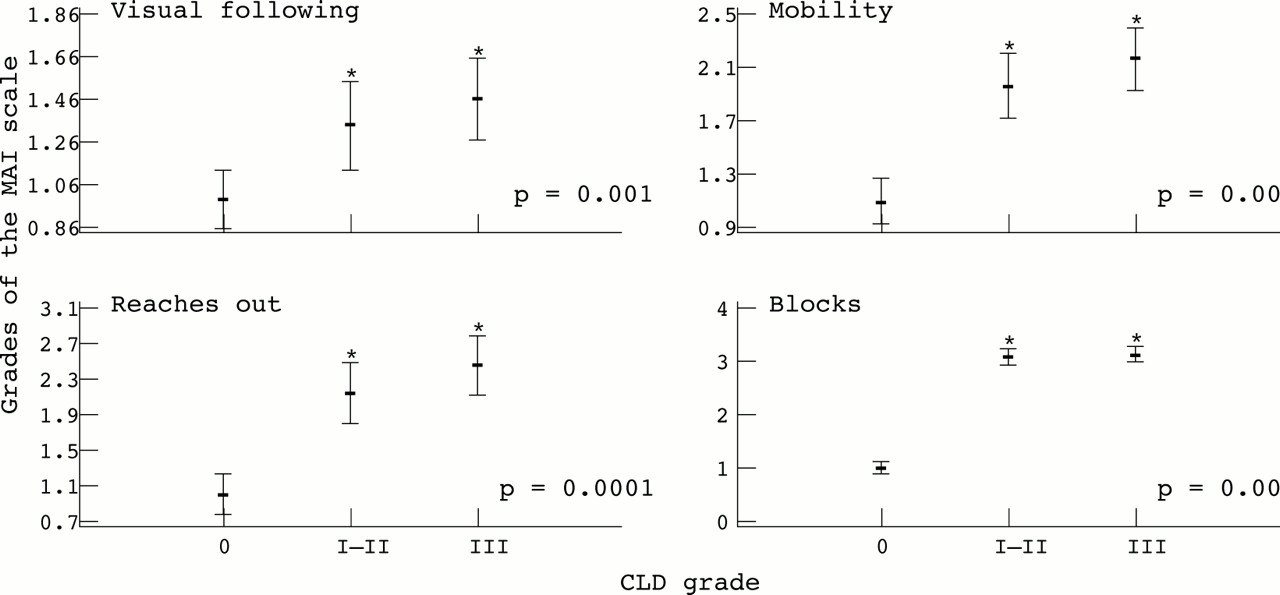
Differences in outcome of four items within the category of volitional movements in the movement assessment of infants (MAI) scale as related to severity of chronic lung disease (CLD). Asterisks denote significant differences between the control group and infants with CLD, and the p values indicate the level of significance. The bars indicate mean value and standard deviation.
APGAR SCORE, POST-NEONATAL INFECTIONS, AND MOTOR PERFORMANCE
Apgar score ⩽ 5 at five minutes was associated with poorer performance of volitional movements (p = 0.04) and contributed to 6.76% of variability at 5 months of age. This effect was not seen at 10 months. The number of infections did not have any impact on motor development (p = 0.15 and 0.09) at 5 or 10 months.
DEVELOPMENTAL CHANGES
In both infant groups, motor ability, expressed as the sum of grades, at 5 months was mirrored by the results at 10 months (correlation coefficients and significance levels for CLD and controls were r = 0.51, p = 0.001 andr = 0.44, p = 0.003 respectively). This may suggest that infants who performed in the upper or lower percentile range at 5 months of age continued to do so at 10 months. However, a closer analysis of this correlation disclosed that only 23 of 43 infants in each group performed within the same range at both ages, while no less than one quarter of the CLD and control infants deteriorated or improved their motor performance with age (fig 2).

Age related changes in motor performance between 5 and 10 months of corrected age. Improvement was defined as the “advancement” of an infant's performance from group 1 (the performance below 25 percentiles) at 5 months of age to group 2 or 3 (the performance between 25 and 75 percentiles or above 75 percentiles) or from group 1 to group 3 at 10 months of age. Deterioration was defined as occurring when the infant's performance at 5 months of age was assigned to a higher group than at 10 months of age.
When the different categories of motor performance were analysed separately, the most pronounced discrepancy between the infants with CLD and those in the control group was seen in the category of volitional movements. Whereas improvement in the execution of volitional movements was seen in 16 control infants, the corresponding amount of motor improvement was observed in only eight infants with CLD. In the remaining categories, the proportions of infants who improved/deteriorated were similar.
DIFFERENCE BETWEEN EXAMINERS IN ASSESSING MOTOR PERFORMANCE
The assessments of the general motor performance (sum of items) as well as judgments of the specific items made by the three examiners did not differ (analysis of variance, p = 0.42). Thus the examiner involved did not influence the evaluation of motor behaviour.
EVALUATION ACCORDING TO THE GRIFFITHS' DEVELOPMENTAL SCALE AT 10 MONTHS OF CORRECTED AGE
Unlike the results from MAI assessments, the Apgar score had no impact on psychomotor development at 10 months of age according to the Griffiths' scale. Furthermore, CLD was the only factor that significantly affected the results (fig 3). As shown, the outcome from the hand and eye coordination scale (scale D) and the performance and intelligence scale (scale E), as well as from the total sum, was significantly worse in the CLD group. The severity of CLD was particularly linked to deterioration in hand and eye coordination and the sum of all scales.

{kind=link}
{kind=link}
{kind=link}
Relation between the outcome with respect to the subscales of the Griffiths' developmental test and the severity of chronic lung disease (CLD). Asterisks denote significant differences between the control group and infants with CLD, and the p values indicate the level of significance. The bars indicate mean value and standard deviation.
There was a highly significant correlation between psychomotor accomplishment, as indicated by the total sum in the Griffiths' test, and the sum of scores describing motor performance according to the MAI scale (linear regression analysis p < 0.0005, correlation coefficient r = −0.63).
Discussion
Our study shows that, in the absence of IVH/PVL, CLD has a deleterious effect on early development. The disparity in the motor performance of infants with CLD and controls was restricted to specific functions—that is, tasks requiring visually guided arm movements, as shown by blocks and reaches out in the MAI and by the hand and eye coordination scale in the Griffiths' developmental test. These results are supported by other studies that found impairments in control of hand and eye coordination in infants born very prematurely, which persisted into later years. Bowen et al 23 have documented significant weakness in eye and hand coordination in neurologically normal extremely low birthweight infants at the age of 3 years.
This impairment in hand and eye coordination may reflect a particular sensitivity to subcortical damage and/or may reflect enhanced susceptibility of neural pathways involved in visual control of arm movements. The impaired control of voluntary goal directed movements of the arm and hand could be due to damage in both corticospinal motor pathways (centrum semiovale) and visual pathways (central occipital white matter).24
The aetiology of such presumptive lesions in the central nervous system of infants with CLD may involve diffuse prenatal or postnatal insults. Lesions in the central nervous system and CLD itself may have the same cause—that is, perinatal infection leading to cytokine mediated inflammatory processes.25 Damage caused by a prenatal insult could be aggravated postnatally, when infants with CLD suffer recurrent episodes of hypoxia.6-9 In addition, such episodes in infants with CLD may reccur as a consequence of decreased sensitivity of peripheral chemoreceptors to hypoxia.26
Previous studies on the relation between CLD and neurological sequelae are contradictory.1 ,2 This may be because many very low birthweight infants with CLD also suffer from IVH and/or PVL. In addition, a direct comparison of infants with and without CLD is complicated by the fact that, in many studies, the infants with CLD had a shorter gestation and lower birth weights and thus suffered from a more complicated neonatal course.
To circumvent these problems, the infants with CLD included in this study did not have severe IVH/PVL, and they were compared with control infants chosen with respect to gestational age at birth, even though a perfect match was difficult to obtain (see the Methods section).
As the occurrence of a simple correlation between a specific hazard and developmental deviation is unlikely, we included additional risk factors that may affect development. We analysed the prevalence of maternal infections leading to premature rupture of the membranes, a low Apgar score at five minutes after birth27, small for gestational age, IVH/PVL 1–2, patent ductus arteriosus requiring ligation, and infections before the psychomotor examinations. The prevalence of chorioamnionitis, premature rupture of the membranes, and patent ductus arteriosus requiring ligation were almost the same in the group with CLD and the control group. The only difference between the groups was represented by the Apgar score. An Apgar score ⩽ 5 had a negative effect on motor development, but the association was temporary and was no longer observed at 10 months of age.
Whether the early developmental impairment observed in infants with CLD is a predictor of later neurodevelopmental abnormalities remains unclear. A review of the literature discloses that developmental differences between infants with and without CLD are only observed at certain ages. Neither examination at 40 weeks of postconceptional age using the Dubovitz scale28 nor the five month assessments in the present study showed any differences in the neuromotor development of these two infant groups. However, the examinations performed at 10 months of age in this study showed the negative influence of CLD on specific functions as well as on the total sum of the Griffiths' test. More infants with bronchopulmonary dysplasia were reported to be poor performers at 2 years of age (the Bayley scales) than infants with only mild or no bronchopulmonary dysplasia.29 Finally, a long term follow up at 9 years of age showed no difference in the IQ scores of infants born before term with and without bronchopulmonary dysplasia, and the deviations observed in this study were ascribed to prematurity and perinatal events rather than to lung disease itself.30
There was a high level of correlation between motor skills as evaluated by the MAI scale and psychomotor development measured by the Griffiths' developmental test. As known from earlier studies,3 ,22 the Griffiths' test exhibits high specificity in a group of healthy full term infants but much lower specificity in preterm infants with neonatal complications. Still, within the general motor-perceptive-mental capacity shown in this study, some developmental traits may be discerned at an early age.
CONCLUSIONS
CLD has a deleterious effect on early development of certain psychomotor functions such as hand and eye coordination, and on perception and intelligence. The results from this study re-emphasise the necessity for careful follow up, including assessment of the possible need for referral to early childhood intervention programmes.
Acknowledgments
The authors wish to express their sincere gratitude to Carin Allert, Christina Eriksson, and Britt-Marie Bergström for their skilful motor assessments. This study was supported by the Bank of Sweden Tercentenary Foundation and the Queen Silvia's Jubilee Fund for Research on Children and Handicaps.