Article Text

Abstract
AIM To compare the prevalence of childhood and adolescent behavioural problems in low birthweight infants with matched controls.
METHODS A cohort study of a geographically defined population of survivors of ⩽1500 g birthweight born in 1980 and 1981 and age, sex, and school matched controls was undertaken. Children with a clinical disability were excluded. Data from Rutter questionnaires, completed by parents and teachers when the children were aged 8 and again at age 14 years, were assessed.
RESULTS From an initial 40 321 births in 1980–81 there were 399 of birthweight ⩽1500 g, of whom 219 survived to age 8. After exclusion of the 42 children with clinical disability, 177 cases comprised the sample. Of these, 10 (6%) refused or could not be contacted, leaving 167 cases for each of whom a matched control was obtained. At age 14 years, both parent and teacher questionnaires showed an increased prevalence of behavioural problems in cases compared with controls. The presence of a pervasive behavioural problem, when the responses of parents and teachers were concordant, was present in 9% of cases and 3% of controls. There were 132 pairs where the cases and controls were the same at ages 8 and 14 years and provided longitudinal data. The parental questionnaire showed there was a significant decrease in the prevalence of behavioural problems for cases and controls between the ages of 8 and 14 years. There was almost no longitudinal change in the prevalence of behavioural problems as shown by the teacher questionnaires.
CONCLUSION Although low birthweight infants are at increased risk of behavioural problems, because they comprise only a small proportion of all births, their population attributable risk for behavioural disorder is around 2–3%.
- behavioural problems
- low birthweight
- Rutter questionnaires
Statistics from Altmetric.com
Survival rates among low birthweight infants have improved as neonatal intensive care has evolved.1-5 Although studies have found no evidence of an increased prevalence of severe disability,6-8 the quality of life of all survivors remains a cause for concern.
Most earlier outcome studies of very low birthweight (VLBW) infants have been limited to an assessment of the prevalence of clinical disabilities or to measures of cognitive and motor performance. More recently attention been given to behavioural issues, and reports have addressed aspects of behavioural problems in low birthweight infants, such as prevalence9 and the tools of measurement,10 patterns of neuropsychological function,11 neurodevelopmental outcome,12associations with IQ, language and other skills,13 and factors contributing to behavioural outcome, such as cerebral damage and social environment.14 15
A review of published reports between 1989 and 1992 on the long term prognosis of extremely low birthweight infants (ELBW) showed that, despite normal IQs, 60–70% experience problems at school. Many of the children have cognitive, perceptual, and motor deficits combined with behavioural problems, referred to as “the new morbidities.”16 These morbidities have been defined as the combination of psychosomatic symptoms, such as sleeping problems, lack of appetite, and headache, with psychomotor features, such as overactivity, poor concentration, tendency to tire easily, and behavioural disturbances.
Interest has been growing in identifying the prevalence of subtle longterm morbidities, or new morbidities. A review of follow up studies of VLBW and ELBW infants to school age included minor neurodevelopmental abnormalities, motor delay, and behavioural problems. To identify these morbidities, gross IQ measures may not be useful as most VLBW and ELBW infants are of average IQ.17The review concludes that there is a need for the more subtle difficulties to be defined and specifically assessed, and as these difficulties may not manifest themselves in infancy and early childhood, it becomes increasingly important to follow up prematurely born infants to school age and beyond.
A cohort of low birthweight infants born in 1979, 1980, and l981 was assessed for clinical disability at the age of 3 years. A subsample of this cohort was reassessed when aged 8 years.6 9 18Rutter behavioural questionnaires19-21 for parents and teachers were administered for those children whose birthweights were less than or equal to 1500 g (VLBW) and matched with controls at age 8 years.9 A longitudinal follow up of this cohort is reported here, along with the findings from Rutter questionnaires administered to parents and teachers for the same VLBW cases and controls at age 14 years.
Methods
Data from all infants weighing ⩽1500 g at birth, and born in 1980 and 1981 to mothers who resided at the time of the birth in the five health districts of the county of Merseyside, were obtained from birth notifications. The obstetric and neonatal records were abstracted for demographic and clinical details of the mother, and birthweight and head circumference of the child. The infants had been examined at the age of 3 years to determine the prevalence of disability and at 8 years to determine the prevalence of subclinical deficits of cognitive and motor function and of behavioural disorders.6 9 18
At the 8 year follow up, an age and sex matched control from the same school was also assessed, for those children attending normal schools. The birthweight of each control was obtained from a questionnaire completed by a parent. Matching for school was done because primary schools tend to draw children from socially homogenous areas, thus creating an effective match for important social variables. This premise was tested at the 8 year follow up, when cases and controls were compared for several socioeconomic variables, including social class, current employment status of the father, housing status of the family, parental education and income and the number of children in the family. All these indices were marginally in favour of better social circumstances for the controls, but none was significant. The only significant difference was that fewer cases than controls were living with both natural parents.18 The birthweight of each control was obtained by questioning the mother.
The children were re-assessed when aged 14 years with the same controls, when possible, as at the 8 year follow up. The children have since moved from primary to secondary schools and the controls were not always at the same school as the index child. If the original control was not available, a new control of the same sex, in the same class at secondary school and nearest in birth date to the index child was selected.
Children with a disability were excluded from the analysis. Disability was defined by clinical criteria and included those children with a diagnosis of cerebral palsy; hearing loss that necessitated the use of a hearing aid or admission to a school for the deaf; visual acuity of less than 6/12 in the better eye or a visual defect sufficient to necessitate special schooling; a learning disability requiring attendance at a special school; and epilepsy.
The behaviour of the children was assessed using Rutter screening questionnaires which were completed by parents and teachers. The index and control children were visited either at school or at home. If the child was seen at school, the Rutter teacher questionnaire was given to the child’s teacher to be completed and returned usually by post. The Rutter parent questionnaire was given either to the parent if present at the interview, or sent home with the child. If the child was seen at home, the parent completed the Rutter parent questionnaire and the Rutter teacher questionnaire was taken to school by the child for completion by the teacher.
The teacher component of the Rutter behaviour scale consists of 26 brief statements each of which is scored 0, 1, or 2, producing a total score within the range 0 to 52. A total score ⩾9 indicates a behavioural problem.19
The Rutter behaviour scale for parents comprises 32 statements concerning the child’s behaviour. The prevalence of the behaviour, or the degree of its severity, or the extent to which the statement applies to the child is scored 0,1, or 2, producing a total score within the range of 0–64. A total score ⩾13 indicates a behavioural problem.20 21
In some instances not all 32 items on the parent questionnaire or the 26 items on the teacher questionnaire were completed. Children were included in the analyses if at least 30 items on the parent, and 24 items on the teacher, questionnaire had been completed.
Three items (restlessness, fidgeting, not settling to activities) each on the teacher and the parent Rutter questionnaires enable the child to be categorised as hyperactive. A score of at least 3 out of 6 on both teacher and parent questionnaires is required for the child to be considered hyperactive.
In addition, the Conners scale,22 modified by Taylor and Sandberg,23 was used for the assessment of hyperactivity. The mean score is taken from eight questions, and, if over 1.5, hyperactivity is indicated.
The χ2 test with Yates’ correction for 2 × 2 contingency tables, Fisher’s exact test, McNemar’s test and thet test for the difference between two proportions were used
Results
There were 40 321 live births in Merseyside in 1980–81; 397 were of birthweight ⩽1500 g, of whom 219 survived to age 15 years. Of the 219 survivors, 12 (5%) refused assessment, were untraced, or had moved abroad. Twenty seven (12%) children with a disability and attending special schools and 13 (6%) with a disability attending mainstream schools were not included in the assessment of behavioural disorders. This report is of 167 children classified as having no disability (77% of the 219 survivors of birthweight <1500 g) and their matched controls.
A flow chart depicting the selection of the study sample and the proportions successfully followed up and assessed is shown in fig 1. An important feature of the study was the high (94%) follow up rate achieved.

Flow chart depicting selection of study sample and proportions successfully followed up and assessed.
The mean birthweight of the 167 non-disabled index cases was 1259 g (range 630–1500 g) and 3352 g (range 2098–4550 g) for the controls. The gestational age of the index cases ranged from 26 to 37 weeks, with a mean of 30.8 weeks. Data on the gestational age of the controls were not obtained, but the mean and range of birthweight indicated that most must have been term infants.
Thirty one (18.6%) of the 167 non-disabled cases were from twin pregnancies whereas all the controls were from singleton pregnancies. There were highly significant differences between the cases and their matched controls in height, weight, body mass index and head circumference, with the cases being smaller for all parameters. These data have been reported before.24
BEHAVIOURAL PROBLEMS IN CASES AND CONTROLS AT 14 YEARS OF AGE
The prevalence and the type of behavioural problem classified in two birthweight groups is shown in table 1. For the whole sample of birthweight ⩽1500 g, comparison of the case–control pairs at age 14 years showed that 40/166 (24%) cases and 16/160 (10%) controls had a behavioural problem on the parental questionnaire. On the teacher questionnaire the proportions were 37/164 (23%) and 16/164 (10%), respectively. These differences between cases and controls were highly significant (p<0.01). On the basis of this screening, both emotion and conduct disorders were more common among cases than controls.
Case control comparison of type of behaviour problem aged 14 years
In both the cases and controls the parent questionnaire was more likely than the teacher questionnaire to indicate the presence of a behavioural problem. The concordance between parent and teacher as to whether or not a behavioural problem was present was 71.4% for the cases and 86.4% for the controls.
Children with a pervasive problem are those who have a high score on both parent and teacher questionnaires. This was present in 9% of cases and 3% of controls.
HYPERACTIVITY
The differences in the proportion of hyperactive children among cases compared with controls on the Rutter assessment scale (cases 4.2% vs controls 2.4%) and the modified Conners scale (cases 4.8% vs controls 4.8%) were not significantly different.
PREVALENCE OF BEHAVIOURAL DISORDERS AT AGES 8 AND 14 YEARS
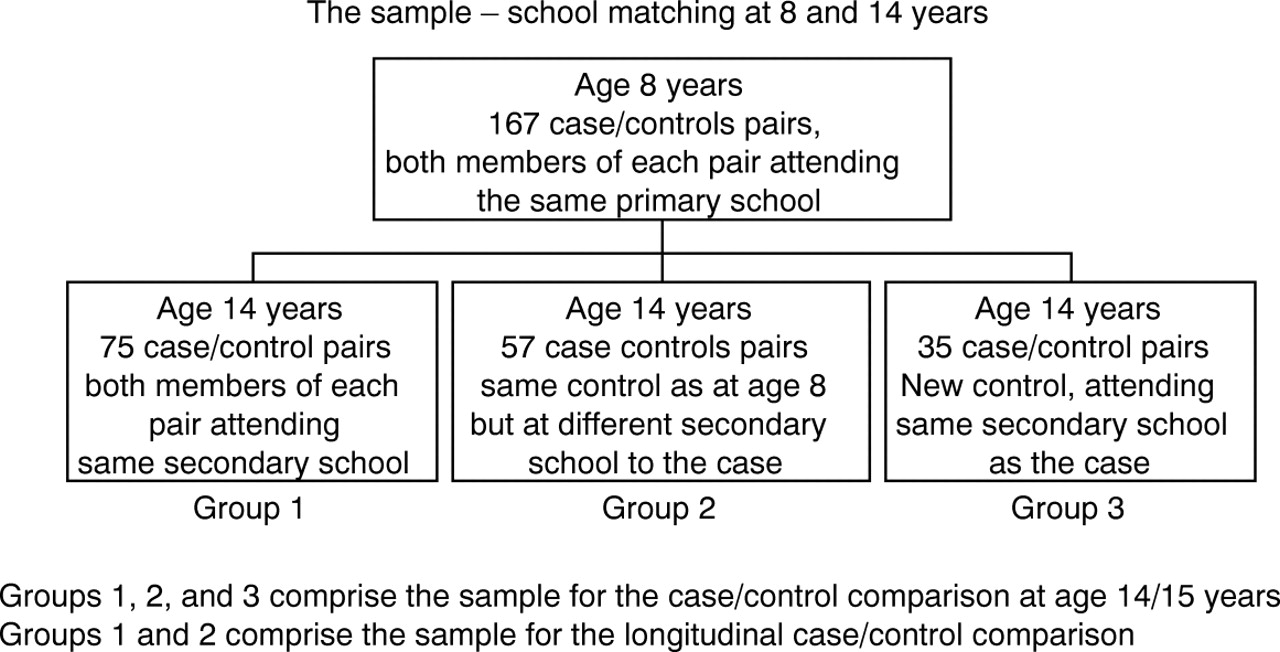
Figure 2 shows the school derivation of the pairs for whom longitudinal data were obtained. The longitudinal comparison is limited to groups 1 and 2 (fig 2)—that is, the pairs for whom the same control child was assessed at age 8 and at age 14 years. This longitudinal comparison was thus limited to 132 (79%) out of the original 167 matched case/control pairs.
{kind=link}
{kind=link}
School derivation of pairs for whom longitudinal data were available.
The longitudinal comparison of the parent and teacher assessments are shown in table 2. After excluding those with missing data, the parental assessment of both cases and controls shows a non-significant reduction in the prevalence of behavioural problems at age 14 compared with age 8 years. For the index cases, comparable data were 33% (38/114) at age 8 years reduced to 24% (28/116) at age 14 years. The controls showed a significant reduction from 20% (23/113) to 9% 10/111; p=0.03. In contrast, the teacher assessment shows almost no change in the prevalence of behavioural problems among cases or controls between the ages of 8 and 14 years; 28% (34/120) when aged 8 years to 25% (30/119) when aged 14 years for the cases and 9% (11/121) to 10% (12/126) for the controls.
Longitudinal change in behaviour problems in index cases and controls assessments at ages 8 and 14 years
Table 2 shows that, on the parental assessment, 12% (14/114) of the cases and 5% (5/111) of the controls had a behavioural problem at both 8 and 14 years of age. This difference was marginally significant; Fisher’s exact test, p=0.05. The teacher’s assessment showed that the behavioural problem was persistent in 12% (14/119) of the cases and in 2% (2/111) of the controls, a highly significant difference; p<0.01.
CHANGE IN THE PREVALENCE OF HYPERACTIVITY AT AGES 8 AND 14 YEARS
The longitudinal change in the prevalence of hyperactivity is shown in table 3. According to the Rutter criterion, there was a highly significant reduction in hyperactivity among the cases, from 18% (23/130) when aged 8 years, to 5% (6/130) at age 14 years; p<0.01. The controls also showed a reduction in hyperactivity from 8/131 (5%) to 2/131 (2%), but the difference did not quite reach significance; p=0.07.
Longitudinal change in prevalence of hyperactivity in cases and controls aged 8 and 14 years
Applying the Connors criterion for hyperactivity, neither the cases nor the controls showed a significant change in the prevalence of hyperactivity (table 3).
POPULATION ATTRIBUTABLE RISK OF LOW BIRTHWEIGHT INFANTS TO BEHAVIOURAL PROBLEMS
Based on the data from this study and national birthweight statistics, the population attributable risk made by low birthweight infants to behavioural problems can be estimated very approximately. In a birth cohort of 100 000 infants about 1000 (1%) will be of birthweight ⩽1500 g, 5000 (5%) will be of birthweight 1501–2500 g, and 94000 (6%) will weigh ⩾2500 g. At current birthweight specific mortalities, about 800 (80%) of the <1500 g group, 4500 (95%) of the 1501–2500 g group, and 90000 (95%) of the >2500 g group will survive to adolescence. Those of <1500 g birthweight will account for about 72 cases of behavioural problems (based on a prevalence of 9% from cases in this study where parents and teacher questionnaires were concordant for the presence of behavioural problems). Similarly, those of birthweight >2500 g will account for 2700 cases (based on a prevalence of 3% in controls in this study). Data on those of birthweight 1500–2499 g are not available, but assuming a prevalence between that of the very low and the normal birthweight groups, there will be about 5% or 225 cases. Although the infants of ⩽1500 g birthweight are at considerably increased relative risk of behavioural problems compared with those of normal birthweight, the population attributable risk of a behavioural problem is only about 2.5%. In terms of the overall prevention of behavioural problems, focusing on those adolescents who were of low birthweight is of limited value.
Discussion
The Rutter parent and teacher questionnaires are screening and not diagnostic instruments. Nevertheless, they have acceptable inter-rater and re-test reliabilities20 21 and have been used to assess the prevalence of psychiatric problems in children. The cutoff point of the Rutter questionnaire score has been validated using children attending psychiatric interviews as criterion standards.20 21 25
The main observation of the study is that, in early adolescence, low birthweight children have a significantly higher prevalence of behavioural problems, as determined by both parents and teachers, than their normal birthweight controls. Anecdotally, some mothers of the cases who had spent time in the neonatal intensive care unit commented that they had not achieved the same rapport with the case child as they had with siblings. A failure of mother–child bonding may, therefore, have contributed to the higher prevalence of behavioural problems in the low birthweight cohort.
Although the initial matching of cases and controls was by school, in order to minimise social and economic differences, those differences that were observed favoured the controls. It is possible, therefore, that the persisting socioeconomic inequalities could account for the difference in the prevalence of behavioural disorders in cases and controls. Alternatively, the cases made more frequent use of various medical services than the controls. Initially, most of the cases were admitted to neonatal intensive care and subsequently they were more frequent attenders at hospital as inpatients and outpatients and visited the family practitioner more often than did the control children. The increased parental anxiety associated with more frequent health service use may interact with the child’s psychological development—a cycle of parental anxiety leading to behavioural problems, producing further anxiety.
The increased prevalence of conduct and emotional problems in low birthweight children is clinically important. A recent long term follow up of a cohort of infants born in 1946 found that adolescent emotional instability and conduct problems were associated with various causes of premature death, specifically accidental and suicide deaths.26
Furthermore, the observation that the teachers’ perception of the prevalence of abnormal behaviour in the children, irrespective of whether they were cases or controls, was almost unchanged between the ages of 8 and 14 years. In contrast, parental perception was of a reduction in the prevalence of abnormal behaviour between the ages of 8 and 14 years. This was an unexpected observation as the teenage years are recognised as a time when parental–child tensions arise. Although the change did not reach significance and caution must be exercised in its interpretation, nevertheless, it may indicate a changing ability of the parent to cope with childhood behaviour. Alternatively, parental perception of a decrease in behavioural problems in both cases and controls in adolescence may reflect a shortcoming of the measuring instrument. The Rutter questionnaires were developed to identify behavioural problems in 11 year olds, and their validity for use among adolescents has not been established.
Acknowledgments
We thank the young participants, their parents, and school staff for excellent cooperation throughout the study, and the British Heart Foundation for funding.