Article Text

Abstract
Aim: A cross sectional (prevalence) study was performed to assess the usefulness and sensitivity of commonly employed criteria to identify infants for routine ophthalmoscopic screening for retinopathy of prematurity (ROP).
Methods: At a tertiary care centre between 1 January 1992 and 30 June 1998, experienced vitreoretinal specialists screened 438 premature infants for ROP. Retinal maturity and the presence of ROP were determined by indirect ophthalmoscopic examinations.
Results: Of the eligible infants surviving 28 days, 276 (91.7%) of 301 infants with birth weights ≤1500 g and 162 (52.3%) of 310 infants with birth weights between 1501 and 2500 g were screened for ROP. 10 (3.9%) of the 310 infants with larger birth weights developed stage 1 or 2 ROP. Two (0.6%) of the 310 infants with larger birth weights developed stage 3 ROP. These two infants progressed to threshold ROP and required treatment.
Conclusions: Relatively restrictive criteria to identify premature infants eligible for routine ophthalmoscopic screening for ROP may be the cause for some infants going unexamined and their ROP undetected.
- retinopathy
- premature infants
- low birth weight
- blindness
- visual impairment
Statistics from Altmetric.com
Blindness and poor visual acuity due to retinopathy of prematurity (ROP) are serious morbidities of premature birth. The CRYO-ROP trial has demonstrated that cryotherapy decreases the risk of blindness by 33% once threshold ROP is reached.1,2 Threshold disease is defined as 5 or more contiguous or 8 cumulative clock hours of stage 3 ROP in either zone 1 or 2, in the presence of so called “plus” disease. Threshold disease occurs on average at 37 weeks’ postmenstrual age in some infants with birth weights less than 1250 g. Because the risk of blindness or visual impairment can be decreased with therapy, many infants are screened with serial retinal examinations to identify the few infants with threshold ROP.
Screening examinations are not without problems, however.3 They are uncomfortable for the infants, anxiety provoking for parents, and in some cases may lead to an extended stay at the tertiary care centre when an infant might otherwise be transferred to a hospital closer to home. Screening programmes at busy centres are time consuming and labour intensive. These issues must be weighed against the risk of missing a case of threshold ROP and the opportunity to intervene with treatment that would lower the risk of severe visual impairment.
As our understanding of ROP increases, screening guidelines are altered (Table 1). In 1992, the American Academy of Pediatrics (AAP) and the American College of Obstetricians and Gynecologists published ROP screening guidelines.4 In 1997 and again in 2001, the AAP, the American Association for Pediatric Ophthalmology and Strabismus, and the American Academy of Ophthalmology issued new screening guidelines.5,6 The 1997 and 2001 guidelines, compared with the 1992 guidelines, recommend that examinations be limited to infants born more prematurely but expands the criteria to include infants with higher birth weights regardless of clinical course. The discretionary category in all these guidelines has been altered in the 1997 and 2001 guidelines to include instability in the clinical course rather than oxygen use. In 1998, Wright et al7 argued against the use of the AAP’s discretionary category and favoured the more liberal use of screening a larger number of less premature and higher birthweight neonates. Wright et al cited a 9% false negative rate for the detection of severe ROP when the 1997 AAP screening guidelines were employed without using the discretionary category. Wright’s results would be unchanged with the 2001 AAP screening guidelines.
Retinopathy of prematurity screening criteria
This study was undertaken in an effort to evaluate the 1997 and 2001 AAP screening criteria5 and Wright’s proposed criteria7 in a population of neonatal intensive care unit (NICU) admissions previously screened under criteria that are more liberal. Our hypothesis was that the rate of identification of ROP ≥ stage 3 would not be affected by using more restrictive screening guidelines. Our hypothesis does not include infants with birth weights ≤1500 g. The results for infants ≤1500 g are reported for completeness.
METHODS
A retrospective review of all infants admitted to Fletcher Allen Health Care (FAHC) with birth dates between 1 January 1992 and 30 June 1998 and birth weights ≤2500 g was performed. FAHC, a tertiary care teaching institution affiliated to the University of Vermont College of Medicine, is located in rural New England with admissions primarily from northern Vermont and New York. A single vitreoretinal group screened all of the neonatal inpatients and the vast majority of outpatients. Binocular indirect ophthalmoscopy with external, trans-scleral depression was used for each examination.
Inpatient charts of all infants admitted to the FAHC NICU with birth weights ≤2500 g were reviewed. The local outpatient ophthalmology charts were reviewed for infants with birth weights ≤2500 g. An infant was excluded if he or she had an eye examination for a diagnosis other than ROP (for example, chorioretinitis, congenital anomalies) and did not meet screening criteria. The data obtained from the inpatient and outpatient charts are listed in Table 2. Early ultrasound or menstrual dating determined postmenstrual age. Ballard scoring was used if this information was equivocal. The use of supplemental oxygen was defined as more than 4 hours of supplemental oxygen at any concentration.
Data collected from inpatient and outpatient medical records
Local screening guidelines in 1992 and 1993 included screening for all infants ≤1750 g regardless of supplemental oxygen use, and all infants between 1750 g and 2500 g with supplemental oxygen use (Table 1). From January 1994 to the end of June 1998, the local screening guidelines were altered to include screening for all infants ≤1500 g regardless of supplemental oxygen use, and all infants between 1501 g and 2500 g who required supplemental oxygen. For all infants who were screened for ROP, the date of each examination, and the stage and zone of disease for each eye were recorded. Data collection was considered complete once the retinas reached maturity or threshold disease requiring treatment. Infants not followed to retinal maturity or threshold disease were considered to have complete data if nasal maturity was documented bilaterally and the remaining areas of retina were immature and without ROP.3 Patients were excluded if the examination was obtained for reasons other than ROP screening and the infant did not meet local screening criteria used at the time.
Data were tabulated and stored in a Microsoft Office `97 Excel spreadsheet. Data were analysed with sas (Version 8.0, SAS Institute, Cary NC) and prophet (Prophet 21,Yardley, PA) software programs.
RESULTS
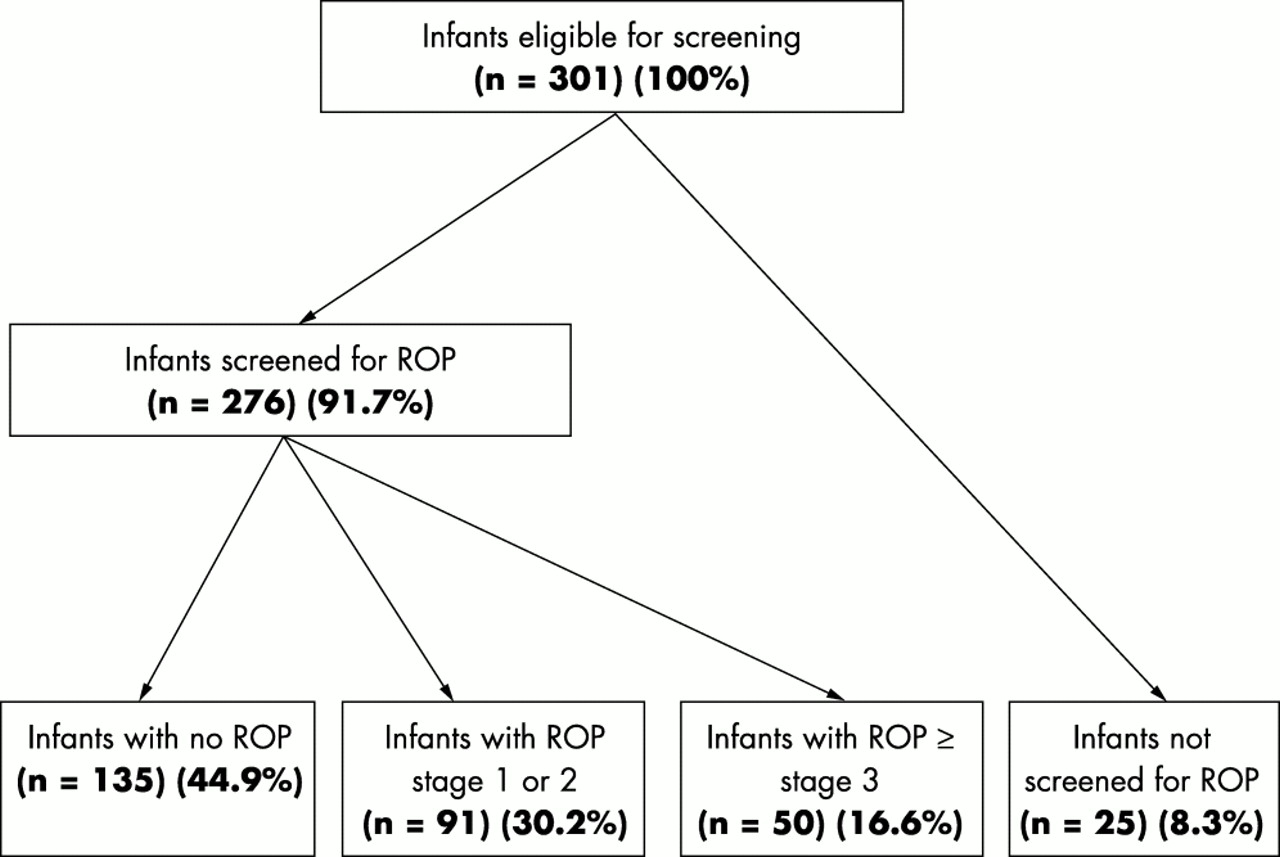
Between 1 January 1992 and 30 June 1998, 1195 infants with birth weights less than 2500 g were admitted to the FAHC NICU. Eight infants (0.007%) were excluded from the database because chart access was not available. Of the remaining 1187 infants, 330 (27.8%) were ≤1500 g and 857 (72.2%) were 1500–2499 g. Of the smaller infants, all were eligible for screening and 301 (91.2%) survived > 28 days. Of the larger infants, 327 (38.2%) were eligible for screening and 310 of these (94.8%) survived > 28 days (Fig 1). Of the 301 surviving smaller infants, 276 (91.7%) were screened for ROP (Fig 2). Of the 310 surviving larger infants, 162 (52.3%) were screened for ROP (Fig 3).

Infant screening eligibility.

Number of infants screened and stages of retinopathy of prematurity (ROP) in infants with birth weights ≤1500 g.

{kind=link}
{kind=link}
{kind=link}
Number of infants screened and stages of retinopathy of prematurity (ROP) in infants with birth weights 1500–2499 g.
Fifty (16.6%) of the 301 smaller infants developed ROP ≥ stage 3. Ten (3.2%) of the 310 infants with larger birth weights developed stage 1 or 2 ROP. Two (0.6%) of the 310 infants with larger birth weights developed stage 3 ROP. These two infants progressed to threshold ROP and required therapy.
One of the two larger infants who progressed to threshold ROP was an identical twin (whose brother never developed ROP). He was delivered by caesarean section at 31 weeks’ corrected gestational age following a pregnancy complicated by polyhydramnios. He had bilateral pleural effusions, ascites and pericardial effusion at birth, and required prolonged pulmonary intubation with assisted ventilation and high concentrations of oxygen. He also required treatment for bacterial sepsis and inferior vena caval thrombosis, both complicating an indwelling central venous catheter. Although the stage 2 ROP in the right eye regressed spontaneously, that in the left eye progressed, and treatment for threshold ROP in the left eye was performed 8 weeks after birth. The last follow up was performed when this child was 5 years old. He is hyperopic with stable accommodative esotropia, and best corrected acuities are 20/25 in the right eye and 20/20 in the left eye. No untoward long term retinal sequelae of either the ROP or the laser have occurred.
The second of the two larger infants in our series who progressed to threshold ROP was delivered by caesarean section at 30 weeks’ corrected gestational age after a pregnancy complicated by fetomaternal haemorrhage. The baby’s haematocrit at birth was 7.0, following several fetal transfusions of erythrocytes, and additional transfusions followed over the next 2 weeks. The haematocrit eventually climbed to 17.1. The child also required treatment with surfactant for respiratory distress syndrome, but the pulmonary status improved rapidly, and the child was extubated 1 week after birth. Stage 2 ROP in both eyes progressed to threshold 8 weeks after birth, and bilateral laser retinopexy was performed. Now 4 years old, this child has no long term ill sequelae from either the ROP or the laser, and the visual acuity is 20/30 in each eye.
Our local guidelines selected 611 infants for screening and 438 (71.7%) infants were actually screened. Wright’s guidelines7 would have selected 390 infants for screening (Table 3), and 337 of those infants were actually screened. All infants identified as having ROP ≥ stage 3 using local guidelines were identified with Wright’s guidelines. The 1997 and 2001 AAP guidelines5,6 would have selected 302 infants for screening (Table 4), and 278 of those infants were actually screened. However, 12 infants with ROP, two of whom developed threshold disease, might have been excluded from screening under the 1997 and 2001 AAP guidelines.
Sensitivity and negative predictive value of Wright’s guidelines6 for retinopathy of prematurity (ROP) screening
Sensitivity and negative predictive value of American Academy of Pediatrics 1997 guidelines5 for retinopathy of prematurity (ROP) screening
The timing of examinations was analysed. Except for infants with a postmenstrual age at birth greater than 34 weeks, the mean age for first examination was between 6 and 7 weeks. Of 229 infants with birth weights less than 1500 g and born at less than 32 weeks of postmenstrual age, three (1.3%) had ROP ≥ stage 3 (one threshold) on first examination. This information supports the 1997 and 2001 AAP guidelines5,6 to perform the first examination between 4 and 6 weeks.
DISCUSSION
The information obtained from this review of ROP screening examinations did not support the hypothesis that a more restrictive set of guidelines, the 1997 and 2001 AAP guidelines,5 would not affect the rate of identification of ROP ≥ stage 3. However, it does support Wright’s guidelines7 of examining all infants born at ≤32 weeks’ postmenstrual age or ≤1500 g regardless of the supplemental oxygen requirement. Further study is needed to define the characteristics that put the older and larger infant at risk for severe ROP.
The incidence of ROP has been well established for infants with birth weights ≤1250 g. Eighteen per cent reach stage 3 and another 6% reach threshold disease. The incidence in the less premature, higher birthweight infants is not as well defined. Wright et al7 published a study in 1998 that focused on the incidence of ROP in larger infants. In that study, no infant with a birth weight ≥1200 g or with a postmenstrual age ≥30 weeks developed threshold ROP. Furthermore, no infant with a birth weight ≥1500 g or with a postmenstrual age ≥32 weeks developed ROP ≥ stage 3. However, if the 1997 and 2001 AAP guidelines5,6 were followed, 9% (6/67 infants) of infants with ROP ≥ stage 3 would have been missed if the discretionary category were not invoked. Given these findings, Wright et al recommended that screening examinations should be performed in all infants born at ≤32 weeks’ postmenstrual age or with birth weights ≤1500 g.
The large number of unscreened, surviving, eligible infants affects the precision of our data. Many of the missed examinations were out of our control (cancelled or no show appointments, and appointments with ophthalmologists out of the area). Although 47.7% of the eligible, surviving infants with birth weights >1500 g were not screened, only 8.8% of the infants with birth weights ≤1500 g were not screened. Use of oxygen was used to decide which infants in the latter group were screened, but these criteria were not used to screen the smaller infants. The definitions of significant oxygen use (duration and FiO2) and “unstable course” vary among clinicians. These data indicate that when discretion is required examinations may be relatively less likely to be scheduled and performed. We believe guidelines that are more definitive rather than ones that are more discretionary are needed to limit the number of infants at risk who are not screened for ROP.