Article Text

Abstract
AIM To audit the prevalence of retinopathy of prematurity (ROP) in a level 2 status neonatal unit.
METHODS Data were collected prospectively over 9 years from September 1989 to September 1998. Preterm infants were examined according to the Royal College of Ophthalmologists' guidelines and retinopathy graded following the International Classification of ROP. ROP 3–5 was analysed using logistic regression in relation to time, and to gestational age and birth weight.
RESULTS 383 babies were examined. Mean gestational age fell over the 9 year period (p=0.051) as did mean birth weight (p<0.001). There was a decrease in the number of infants with ROP grades 3–5 over the 9 years (p=0.045 and, when adjusted for gestational age and birth weight, the decrease in ROP 3–5 was significant (p=0.03).
CONCLUSIONS This study found a significant reduction in the incidence of ROP during the 9 years of the study period, despite a decrease in mean gestational age of and birth weight. The reduced incidence of ROP is attributed to improvements in ventilation techniques and overall care of the neonate, in particular the use of prenatal steroids and surfactant.
- retinopathy of prematurity
- audit
- infants
Statistics from Altmetric.com
Recent advances in neonatal care have improved the survival rates for premature infants1 and this has been accompanied by an increase in the incidence of retinopathy of prematurity (ROP).2-4 ROP is a leading cause of childhood blindness56 and accounts for up to 10% of childhood blindness in developed countries.7-9 To analyse our experience of the changing incidence of ROP an audit was undertaken.
Materials and methods
Infants were examined on the neonatal unit (NNU) at the Whittington Hospital between September 1989 and September 1998. The NNU has 23 cots, receives 250 babies a year, and has level 2 status. The infants were examined according to the Royal College of Ophthalmologists' guidelines that were published in 1995.1011 Preterm infants were referred by the neonatologists according to (1) birth weight equal to or less than 1500 g, (2) post-menstrual age equal to or less than 31 weeks, and (3) paediatrician's concern—for example, prolonged exposure to oxygen. Pupils were dilated using phenylephrine 2.5% and cyclopentolate 0.5% eye drops instilled 1 hour and 30 minutes before examination. Indirect ophthalmoscopy was performed using a 30 dioptre lens. Neither a lid speculum nor scleral depressor were routinely used. The examinations were performed mainly on a weekly basis and continued until vascularisation had reached zone 3. Those with ROP were screened at intervals indicated by the severity of the disease.
Data were recorded prospectively and the presence of retinopathy was graded following the International Classification of ROP.1213 Co-existing medical problems were identified at the time of examination from the medical case notes.
Results
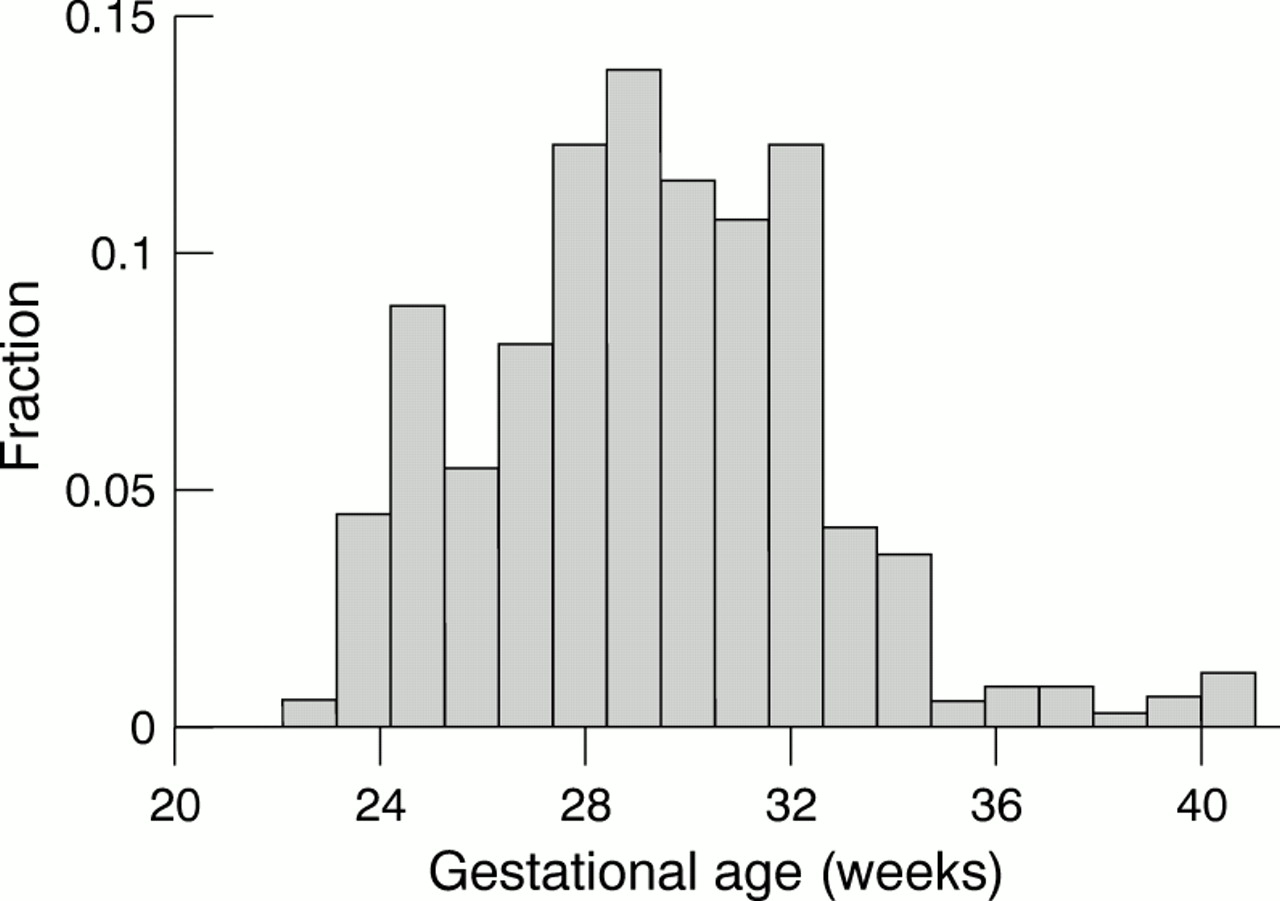
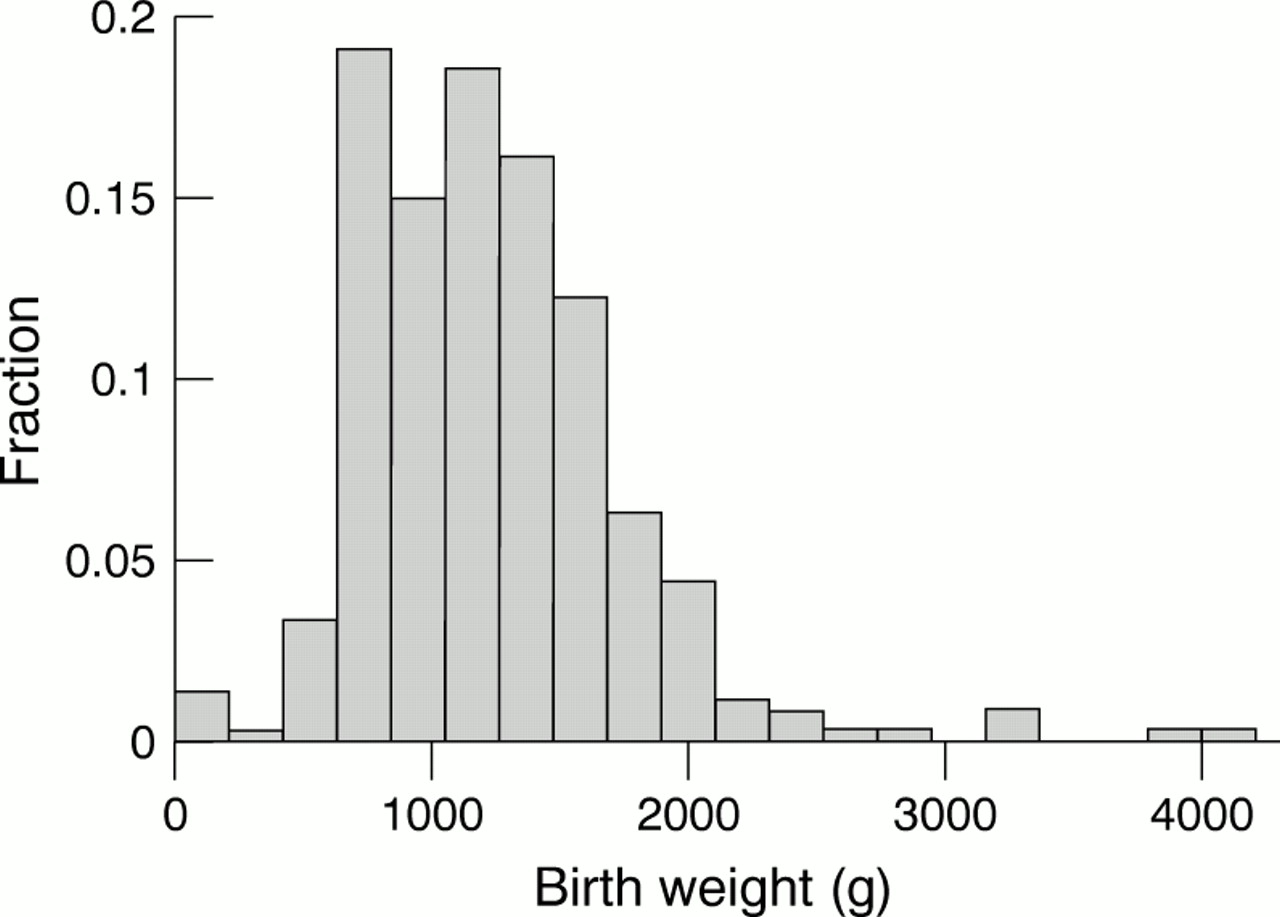
A total of 383 babies were screened during the 9 year study period. Gestational age had been recorded in 378 babies and birth weight had been recorded in 364 babies. The mean gestational age of all infants over the study period was 29.3 weeks (SD 3.2, range 23–41). The mean birth weight of all infants over the study period was 1229 g (507 g, 110–4190). For purposes of data analysis the infants were divided into three groups (groups 1, 2, and 3) of consecutive 3 year periods of birth, 1989–91, 1992–4, and 1995–7. Mean gestational ages in weeks of the groups were 29.8 (SD 3.7), 29.2 (3.0), and 29.0 (2.8) respectively. The decrease was of borderline statistical significance when considered as a trend over the three groups (p=0.051). The mean birth weights of the three groups were 1361 g (SD 632 g), 1207 g (472 g), and 1134 g (372 g) respectively (Table 1, Fig 1 and 2), there being strong evidence for a decreasing trend over the year groups (p<0.001).
Mean birth weight and gestational age of three groups

Distribution of gestational age.

{kind=link}
{kind=link}
Distribution of birth weight.
Over the 9 year period, 10 babies had ROP grades 3–5; eight had stage 3, one had stage 4, and one had stage 5 (Table 2). When the trend over the three birth year groups was estimated the decrease in ROP of grades 3–5 did not quite reach statistical significance (logistic regression p=0.051). However, there was a lower incidence in the later two groups than the earlier (odds ratio 0.20, p=0.02). Adjusting for gestational age and birth weight, the incidence of ROP 3–5 decreased significantly (p=0.03). The odds ratio per 100 g increase in birth weight was 0.82 (p=0.14) and the odds ratio per 1 week increase in gestational age was 0.676 (p=0.045). This indicates that gestational age was more closely linked to ROP 3–5. The decrease of ROP 3–5 over the three groups was significant (p=0.04) when adjusted for gestational age alone and for birth weight alone (p=0.03). The decrease in ROP 3–5 was even more marked when groups 2 and 3 combined were compared with group 1 (odds ratio 0.20, p=0.02). With adjustment for gestational age alone, the decrease in ROP 3–5 between group 1 and groups 2 and 3 combined was also greater (odds ratio 0.16, p=0.01).
Grades of retinopathy of prematurity (ROP) in three groups
The mean age of infants with no ROP, ROP grade 1 and 2 was 29.4 weeks (SD 3.2). The mean age of infants with ROP 3–5 was 25.8 weeks (SD 1.6).
Discussion
There have been reports of improved survival rates for premature infants resulting in claims of an “epidemic” of ROP.7In this study, despite a borderline decrease in the mean gestational age and a significant decrease in the mean birth weight, the incidence of ROP fell significantly. There was no reduction in the number of infants referred for ROP screening per year and there was a unified set of referral criteria and examination technique over the study period.
This study screened 383 infants over a 9 year period at an average rate of 43 infants per year. This is similar to data published from other units. Goble et al reviewed data from six neonatal units in Birmingham (UK), over a 6 year period and screened a total of 1611 babies8 at a rate of 44.7 babies per neonatal unit per year. Severe ROP is seen predominantly in infants weighing less than 1000 g,1415 and the average birth weight of the screened population in the study by Gobleet al was 1199 g, similar to the average birth weights seen in this study (1229 g). The mean gestational age of the screened population in Goble's study was 29.1 weeks which again, is similar to the mean gestational age seen in this study which was 29.3 weeks.
The reduced incidence of grades ROP 1 and 2 (13%) may relate to the examination technique. A lid speculum and scleral indentation were not routinely used and it is possible that some lower grades of ROP in the periphery were underdiagnosed. The examination technique would not, however, affect the diagnosis of ROP 3–5 and therefore not account for the decreased incidence of ROP 3–5. It is recognised that many factors may contribute to differences in the incidence of ROP between centres, such as neonatal survival and ethnic mix.1617 The diagnoses by individual clinicians may also vary,18 but less so for severe disease. Although these factors may be relevant concerning studies comparing different centres, this study describes a trend within a single centre.
A decrease in the incidence of ROP has been reported from other centres. A Danish study found a decrease in the incidence of ROP for infants with birth weights between 1251 g and 1750 g although there was no decrease in incidence for the infants weighing less than 1251 g.1920 A multicentre UK study looking at neonates less than 1251 g found an increase in ROP in only one of five centres studied, suggesting that although there is increased survival of high risk neonates, this is not associated with a universal increase in severe ROP.21 A study from the United States found a decreased rate of progression from prethreshold to threshold ROP in infants studied between the years 1990–3 (7%) compared to 1985–9 (37%). Bullard et al found a decrease in the incidence of all levels of ROP across all birth weights at the Vanderbilt University Medical Centre in Tennessee. Their study compared infants born over a 12 month period between 1 July 1995 and 30 June 1996 with those born over a 23 month period between 1 January 1986 and 30 November 1987. They suggest that the decrease in both the incidence and severity of ROP may be attributed to the use of surfactant, continuous pulse oximetry, improved neonatal nutritional support, and the use of maternal antenatal steroids.22 However, Reynolds rejects the conclusions of Bullard et al stating that the single centre findings from the Vanderbilt University represent regression towards the mean and that this centre is now resembling the national mean.23 Furthermore, Reynolds goes on to state that controlled trials have shown no benefit from surfactant and that the multicentre LIGHT-ROP study showed no reduction in the incidence of ROP.24
There are many risk factors associated with the development of ROP.25-29 Apart from improvements in the general paediatric care of the infants, there were no other changes to the neonatal environment or the screened population during the study period that would alter the risks of developing ROP.
In conclusion, although this study is from a single centre and the number of patients (383) relatively small, it reflects a decreasing incidence and severity of ROP that is beginning to be found by other centres. This may reflect a regression towards the mean although if many centres are starting to have similar findings then this is unlikely. There is no single change in neonatal management to account for this and it may be that the improved general care of the neonate by the paediatricians (at this unit as well as nationally), combined with advances in prenatal management, have given rise to this trend.