Article Text

Abstract
Background Survival following cardiac transplantation in infancy has improved substantially. There is a growing shortage of donors, the impact of which may be offset by increase in ABO-incompatible transplants, size-mismatching and mechanical support. The authors reviewed their results and outcomes following infant listing for cardiac transplantation over 22 years.
Methods Children <12 months at time of listing for cardiac transplant in 1987–2008 were identified using the departmental cardiopulmonary transplant database. Details were obtained from databases and hospital medical records and subdivided into two eras, 1987–1997 and 1998–2008.
Results In 1987–2008, 49 infants were listed, and 28 (57%) underwent cardiac transplantation (12 in 1987–1997 and 16 in 1998–2008). 15 patients (31%) died on the waiting list, 6 patients were delisted (5 of these because of recovery of cardiac function). There was a decrease in suitable donor offers from a mean of 36 per year in 1996–2000 to 11 per year in 2001–2006 (p=0.008). In 1998–2008, nine listed infants were on mechanical support; there were seven ABO-incompatible transplants, and all transplants were size-mismatched with donors on average 2.7 times heavier than recipients. Waiting times decreased from median 83 to 47 days. Six (21%) of the transplanted patients died, the majority in 1987–1997 and perioperatively.
Conclusions There has been a fall in suitable donors for infant cardiac transplants over time despite increased demand. However, the introduction of size-mismatching, ABO-incompatible transplants and mechanical support has enabled an increase in the number of transplants to be carried out despite this fall in donor numbers. Outcomes following transplantation have improved over time.
Statistics from Altmetric.com
Heart transplantation in infancy is now an accepted option for the management of end-stage cardiac failure1 2 and is usually performed either for cardiomyopathy or for congenital heart disease not thought to be amenable to surgical management or where palliation has failed. Survival has improved substantially over the last 20 years and especially over the last 10 years.1 3
In the UK, there remains a shortage of donors4 with numbers falling over recent years, especially for small infants. The reasons for this are unclear and likely to be multifactorial. To try and offset the lack of donors, changes have been made in transplant strategies. Unlike in previous eras where patients were restricted to compatible blood groups, transplanting across ABO-incompatible blood groups5,–,7 means that most donors of a suitable size are acceptable, and there is a reduced likelihood of organs not being utilised; however, this practice is usually only practical in the infant population due to their relatively immature immune systems and low anti-A and anti-B isohaemagluttinin titres. The use of size-mismatched hearts further increases the donor pool, with donor organs from individuals three times as large as recipients able to be used for transplant.2 8 Smaller patients are now also able to be supported mechanically, by the use of extracorporeal membrane oxygenation (ECMO) and ventricular assist devices (VADs) such as the Berlin Heart Excor VAD (Berlin Heart AG, Germany) which allow for longer support times and potentially increases the number of infants surviving until a donor organ becomes available.9,–,13
What is already known on this topic
▶ Survival following cardiac transplantation in infancy has improved.
▶ Mechanical support is increasingly used as a “bridge to transplant” in paediatric patients.
What this study adds
▶ Number of donor offers has fallen in recent years, especially for infants.
▶ ABO-incompatible transplantation, size-mismatching and mechanical support are among the strategies which have allowed transplant numbers to be maintained or increased.
Freeman Hospital is one of two centres for paediatric cardiothoracic transplantation in the UK. Over a 22-year period from 1987 to 2008, a total of 178 transplants were carried out in children <18 years of age. The first successful infant heart transplant in the UK was in this institution in October 1987, and we have now undertaken 28 cardiac transplants (16% of paediatric cardiac transplants) in infants aged <12 months at the time of listing. We report our results following listing for cardiac transplantation in this group and determined the effect of introducing factors such as mechanical support and ABO-incompatible transplantation into an infant transplant program.
Methods
Children <12 months of age at the time of listing for cardiac transplantation were identified using the institution's cardiothoracic transplant database and hospital medical records and data collected about their outcomes. Results were subdivided into two eras, 1987–1997 and 1998–2008 based on the availability of mechanical support, the practice of ABO-incompatibility and size-mismatched transplants from 1998 onwards.
We looked at the factors important in the changing practice of paediatric cardiac transplantation. The first ABO-incompatible transplant was performed in this institution in 2000, mechanical support is now used as a bridge to transplantation (the program started with ECMO in 1998 but the Berlin Heart Excor pulsatile ventricular assist device has also been in use since 2005), and there is increased use of size-mismatched hearts. There was no change in the catchment area of this institution during the course of the study with patients being referred for assessment from the northern half of England, Scotland and Northern Ireland (an area with a population of around 15 million) as well as occasional patients from out of region.
Patients
Between June 1987 and December 2008, 49 infants (<12 months of age) were listed, and 28 (57%) subsequently underwent cardiac transplantation.
Immunosuppressive regime
Immunosuppression protocols were identical for both ABO-compatible and ABO-incompatible transplants. Preoperative therapy was with ciclosporin and azathioprine, and methylprednisolone was given intraoperatively at the time of cross-clamp release. Postoperatively, antithymocyte globulin was given for up to 1 week and monitored with CD3 levels. Three daily doses of steroids were given following which patients were maintained on a steroid free regime with a calcineurin inhibitor and in selected cases an antimetabolite drug in addition. Routine cardiac biopsies and coronary angiography were not performed in children <5 years of age unless there were clinical or echocardiographic concerns.
Statistical analysis
Kaplan-Meier curves were used to assess survival. Unpaired t tests for independent samples were used to compare results for the two eras with statistical significance taken as p<0.05.
Results
Donor availability
Accurate data on donor availability and total number of offers of organs was available from 1996. Offers suitable for infant recipients for the purposes of analysis were taken as those from donors with weights of <30 kg allowing for a size-mismatch of 3:1 for infants ≤10 kg. There has been a significant decrease in the total number of offers per year (fig 1) from a mean of 36 offers per year (range 11–60) for the fiscal years 1996–2000 to a mean of 11 offers per year (range 9–22) for the fiscal years 2001–2006 (p=0.008).

Number of donor offers <30 kg by fiscal year.
Assessments
The number of infants formally assessed for cardiac transplantation increased over time from 15 in 1987–1997 to 44 in 1998–2008. The outcomes of these patients are shown in table 1.
Number of assessments and outcomes
Listed patients
Forty-nine infants were listed for cardiac transplantation. The breakdown between eras and demographic details are shown in table 2.
Demographic details of listed patients, overall and by era
Thirty-four patients (69%) had cardiomyopathy (30 dilated cardiomyopathy, 3 hypertrophic cardiomyopathy, 1 ischaemic cardiomyopathy due to neonatal myocardial infarction). Fourteen patients (29%) had congenital heart disease, with hypoplastic left heart syndrome (n=7) as the biggest diagnostic group. Twelve patients had univentricular physiology (of whom 10 had previously undergone palliative procedures), two had biventricular circulations. One patient was listed for severe rhabdomyomas obstructing both left ventricular inflow and outflow. The proportion of patients listed for cardiomyopathy in infancy increased from 57% in 1987–1997 to 74% in 1998–2008. There was no significant difference in weight or age at listing or duration of symptoms from onset to listing between the two eras.
Outcomes following listing
Overall, 28 of the 49 listed patients (57%) were transplanted. Median time on the waiting list was 57 (range 1–813) days and decreased significantly from 83 (19–198) days in era one to 47 (1–813) days in era two (p<0.001). Mean age at listing for patients that were transplanted was 133 (4–349) days and mean age at transplantation 203 (34–437) days.
Fifteen patients (31%) died while on the waiting list with an increase in pretransplant deaths over time. In the first era, two patients (14% of those listed in that time period) died, whereas in the second era, there were 13 deaths while waiting (37% of those listed). Six patients were delisted, all in era 2. One of these patients had severe infantile Pompe's disease and was delisted when the diagnosis was confirmed whereas the remaining five delisted patients all recovered and remain well. Diagnosis in all five of these patients was dilated cardiomyopathy or myocarditis.
Outcomes following listing overall and for the two eras are shown in fig 2.
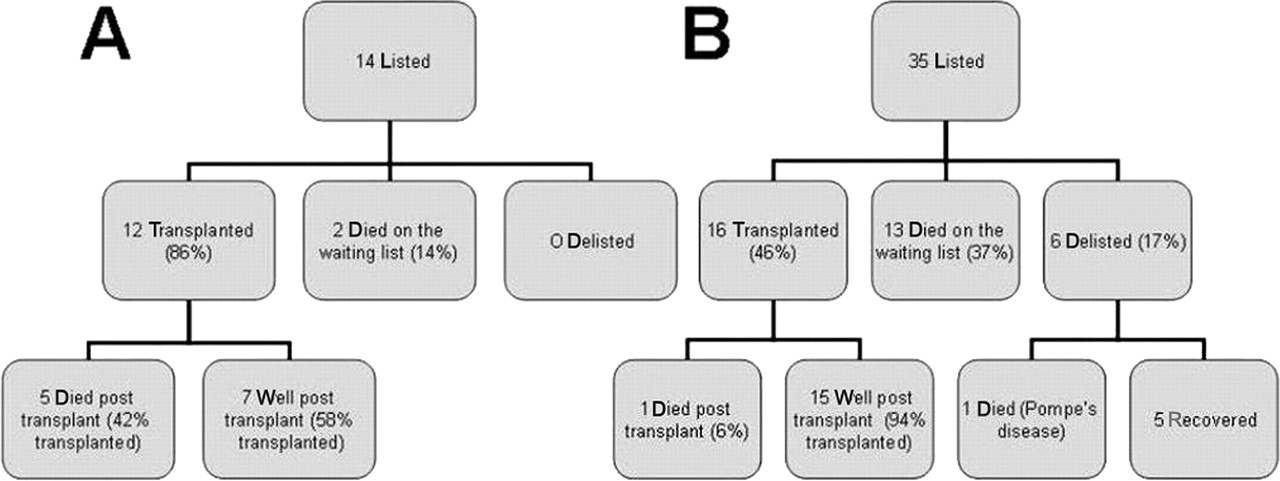
Outcomes following infant assessment for cardiac transplantation: (A) era 1, 1987–1997, (B) era 2, 1998–2008.
For the overall group, at 3 months post-listing, 20 patients (41%) had been transplanted, 3 (6%) were delisted, 14 (29%) had died while listed and 17 (35%) remained listed (fig 3).

{kind=link}
{kind=link}
{kind=link}
Competing risks for outcomes after listing.
Newer strategies introduced in the second era (1998–2008)
ABO-incompatible transplantation
The first ABO-incompatible transplant in our institution was performed in 2000. Seven infants with acceptable antibody titres have received ABO-incompatible grafts (table 3).
Blood groups of donor and recipients with isohaemogluttinin levels pretransplant in ABO-incompatible grafts
Two patients received plasma exchange in theatre in order to reduce their antibody titres. There has been no increased incidence of rejection in this group.
Size-mismatching
The first size-mismatched transplant in this institution was in 2000. Since then, donors have been a median of 2.7 times heavier than recipients (range 1.8–3.8 times).
Mechanical support
Mechanical support (ECMO and VAD support) has been used as a bridge to transplant since 1998. The Berlin Heart Excor ventricular assist device was introduced to our institution in 2005, before which ECMO was the means of support in infancy. Since 1998, 9 (26%) of the 35 infants listed for cardiac transplantation were on mechanical support (five ECMO, four VAD). Of these nine patients, five died (four on ECMO and one on VAD); the remaining patient on ECMO was weaned off support before the transplant, and two patients were transplanted from VAD support. One infant on VAD recovered myocardial function sufficiently to tolerate explantation of the device and was delisted. The smallest child supported by the Berlin Heart in this series was a 4-month-old, 6-kg infant.
In 1987–1997, two (14%) patients were ventilated and on inotropic support at listing, five (36%) on inotropes but not ventilated and seven (50%) on oral antifailure treatment alone. In 1998–2008, 17 (49%) patients were ventilated and on inotropic support at listing, 7 (20%) were on inotropes but not ventilated and 11 (31%) on oral antifailure treatment alone.
Survival following transplantation
Six (21%) of the 28 transplanted patients have died. In 1987–1997, 5 (42%) of the 12 transplanted patients died, 4 within 30 days post-transplant and 1 late death at 4.9 years due to rejection. In 1998–2008, 1 (6%) of the 16 transplanted patients died at 7 days post-transplant. Mean follow-up time from transplant is now 9.8 (range 0.1–21.7) years. Five-year survival increased from 58% in 1987–1997 to 94% in 1998–2008 (p<0.05). No patient transplanted in infancy has undergone re-transplantation to date.
Discussion
Over the last 22 years, there has been a progressive decrease in the number of donor hearts suitable for infant recipients in the UK. However, despite the fact that in recent years, there have been only one third the number of donors as previously, the number of transplants performed is largely unchanged and has even increased slightly from 12 in the first decade studied to 16 in the more recent era in keeping with increased demand. Therefore, the overall strategy in this field to increase the probability of successful transplantation for infants in end-stage cardiac failure has succeeded despite the reduction in suitable donors. We have seen a progressively large decrease in the number of potential donors per year since 2000 with now on average less than 10 suitably sized organs available for infant heart transplants per year. The reasons for this fall in donor numbers are unclear but may be related to a number of factors. A welcome reason is the significant decrease in the number of deaths resulting from road traffic accidents due to implementation of seat belt and car seat legislation as well as more stringent speed controls.4 Negative media publicity in the UK around that time surrounding surgical outcomes and the unauthorised retention of human tissue14 15 could also be postulated to have had an effect. There is currently a move towards increasing public awareness of the need for donor organs through the use of the media, the impact of which remains to be seen.
Referrals for assessment and subsequent listing for cardiac transplantation in infancy have increased substantially in recent years with improved awareness of results of transplantation among affected families and the paediatric cardiologists looking after these patients. In our experience, the majority of cardiac transplants in infancy are performed for cardiomyopathy with patients with congenital heart disease rarely being listed for transplant without previous surgical palliation. Improved results of palliation for single ventricle conditions such as hypoplastic left heart syndrome has led to a delay in these patients requiring consideration for transplant.16
The increased demand on transplant services and the fall in donor numbers in the last decade has required a change in strategy—we are now performing more ABO-incompatible and size-mismatched transplants in order to increase the available donor pool and infants are able to be placed on mechanical support while awaiting transplant. For this reason, despite the fall in donors, the number of transplants carried out in this group has remained relatively steady and even increased over time.
In the infant group, there is the possibility of performing up to a 3:1 size-mismatch transplant without a significant increase in postoperative complications.8 17 The use of larger donors potentially increases the available donor pool, and in our cohort of patients, donors have weighed an average of almost three times as much as recipients in recent years.
Initial work from the Hospital for Sick Children in Toronto in the late 1990s demonstrated the feasibility of ABO blood group incompatible transplantation in infants and showed that this is well tolerated in infants with relatively immature immune systems and low isohaemagluttinin titres.5 6 18 This procedure has now become increasingly adopted outside of Canada and between February 2000 and November 2006; 21 ABO-incompatible cardiac transplants were performed in the UK in children aged 2–40 (median 10) months.7 Seven infants in our institution received ABO-incompatible transplants during the study period, with no episodes of humoural rejection. This practice further widens the available donor pool for smaller infants and younger children and is likely to have a significant effect on waiting times for transplantation both on and off mechanical support.
There is now increasing experience and improved results with mechanical support in the paediatric age group,9 13 and between 1998 and 2008, 48 children were supported in our institution. Veno-arterial ECMO10 19 is a widely accepted means of supporting infants once traditional therapies have failed, although often with high mortality, and has been used in our institution since 1998. Complications on ECMO especially related to anticoagulation, infection and neurological events increase exponentially with time,10 and for this reason, it is no longer looked at as long-term support for infants on the waiting list for cardiac transplantation.
The introduction of the pulsatile VADs, in particular the Excor Berlin Heart, has enabled us to support infants more safely and for longer periods than with ECMO.9 11 12 The incidence of neurological complications on mechanical support varies from 15% to 40% in some series9 20 most often in the form of cerebral infarction due to systemic embolisation. Anticoagulation, especially with warfarin, remains a challenge for smaller infants but has proven to be feasible long-term especially in older children.9 12 In our experience, we have been able to manage selected patients outside of the intensive care setting. One of our listed infants was supported with a biventricular assist device but was able to be explanted and delisted after 120 days of support. Only two patients have died while listed since 2005, and the current mechanical support strategies employed may have led to this decrease in waiting list mortality.
In our experience, there has been a decrease in time spent on the waiting list for those infants successfully transplanted which may not mirror the trend in other age groups. This suggests that the use of ABO and size-mismatched transplants have had a bigger influence on waiting times than the potentially increased support times allowed by the use of mechanical devices. The percentage of patients who died while on the waiting list, however, has increased almost threefold. ECMO is time-limited due to complications of bleeding and infection as outlined above, but there is greater hope for improved outcomes and reduced mortality with the Berlin Heart especially in the infant group. Results in infants <1 year of age with the Berlin Heart in our institution are comparable with results in children aged 1-5 years with no excess respiratory or neurological morbidity.9 International results and in particular those of the Berlin Heart Institute support this with survival of over 70% in infants.
There were a substantial number of patients delisted in the second era of our study. This may reflect a trend towards earlier listing for cardiac transplantation in the context of improved long-term outcomes post-transplant or change in the listing criteria with more infants listed earlier in the course of their disease. There has been a decrease in time from onset of symptoms to listing, and although numbers are relatively small and this was not statistically significant, it may reflect current practice. One does, however, also need to consider whether or not it was appropriate to list these infants in the first place. Five of the six delisted patients in our series had an acute dilated cardiomyopathy, and it is known that in patients who improve, complete recovery of left ventricular systolic function is often delayed to more than a year from presentation.21 This, therefore, has implications for timing of transplantation, and an argument could be made that if waiting times are dramatically reduced, we run the risk of transplanting patients who may otherwise have recovered.
Results of cardiac transplantation continue to improve, with the majority of infants now surviving long term.1 22 23 There has been a significant reduction in postoperative mortality in all series1 2 24 which is mirrored in our results. The significant decrease in post-transplant deaths, especially early, due to improved surgical results, is related to increasing experience, especially with transplantation for congenital heart disease. The International Society for Heart and Lung Transplantation Registry Eleventh Annual Paediatric Report has shown a high 1-year survival of 87% in the years 2000–2006 (improved from 71% in the years 1982–1989) with an overall calculated graft half-life of 15.8 years for patients transplanted in infancy.1 In this age group, there appears to be a higher early mortality post-transplantation but lower late mortality as well as a relative sparing from episodes of rejection and coronary artery vasculopathy.24 One of the problems seen in this group is poor development of the immune system; therefore, these patients are prone to recurrent, often respiratory, infections.25 There does not, however, appear to be an increase in post-transplant lymphoproliferative disease in patients transplanted during infancy.1 2
In conclusion, time spent on the waiting list has decreased in the infant group, but there remains a shortage of donors of smaller organs and mortality while waiting for transplant has gone up significantly. The reduction of donor offers is of major concern, but its effect to date appears to have been partly circumvented by the introduction of ABO-incompatible transplants, size-mismatching and improving results with mechanical support of smaller patients. The significant advances in these strategies has, therefore, enabled service levels to be maintained leading to relatively constant or increasing numbers of successful infant transplants.
Acknowledgments
Data on donor offers was provided by UK Transplant from the National Transplant Database which is maintained on behalf of the UK transplant community.
References
Footnotes
-
Competing interests None.
-
Provenance and peer review Not commissioned; externally peer reviewed.