Article Text

Abstract
Aims: To determine whether the risk factors for SIDS occurring at night were different from those occurring during the day.
Methods: Large, nationwide case-control study, with data for 369 cases and 1558 controls in New Zealand.
Results: Two thirds of SIDS deaths occurred at night (between 10 pm and 7 30 am). The odds ratio (95% CI) for prone sleep position was 3.86 (2.67 to 5.59) for deaths occurring at night and 7.25 (4.52 to 11.63) for deaths occurring during the day; the difference was significant. The odds ratio for maternal smoking for deaths occurring at night was 2.28 (1.52 to 3.42) and that for the day 1.27 (0.79 to 2.03); that for the mother being single was 2.69 (1.29 to 3.99) for a night time death and 1.25 (0.76 to 2.04) for a daytime death. Both interactions were significant. The interactions between time of death and bed sharing, not sleeping in a cot or bassinet, Maori ethnicity, late timing of antenatal care, binge drinking, cannabis use, and illness in the baby were also significant, or almost so. All were more strongly associated with SIDS occurring at night.
Conclusions: Prone sleep position was more strongly associated with SIDS occurring during the day, whereas night time deaths were more strongly associated with maternal smoking and measures of social deprivation.
- SIDS
- night
- day
- prone sleep position
- social deprivation
- smoking
Statistics from Altmetric.com
Sudden infant death syndrome (SIDS) is known to occur more frequently at night, and various physiological theories have been advanced to explain this phenomenon. These include altered circadian rhythm patterns,1,2 or patterns which could be associated with an increased susceptibility to inflammatory responses caused by a drop in the night time cortisol concentrations.3 REM (rapid eye movement) sleep abnormalities,4 diminished melatonin production,5,6 and the effect of toxins produced by growing bacteria7 are also possible explanations. Although epidemiological studies examining differences in risk factors do not appear to have been reported, some hypotheses can be suggested. Deaths could occur more commonly at night in older infants because sleep is increasingly concentrated into the night. Prone sleep position could work through a thermal mechanism, so that the variables related to bedding and environmental temperature would be more important at night. Finally, as different arousal responses in either the babies or their parents are a potential mechanism leading to the death of the baby, it could be hypothesised that the arousal stimuli are reduced at night, making prone sleep position more dangerous.
Data from the New Zealand Cot Death Study,8,9 a large nationwide case-control study, were used to examine differences in risk factors between infants dying during the day and those dying at night. As well as testing the possible hypotheses, variables relating to the four modifiable risk factors (sleep position, maternal smoking, bed sharing, and breast feeding9), variables used to adjust for confounding, those related to illness in the infants, and those related to the mother’s use of alcohol and cannabis since the birth of the baby were also considered.
METHODS
The New Zealand Cot Death Study was a case-control study carried out between 1 November 1987 and 31 October 1990. It involved a sample of infants drawn from health districts in Auckland, the central North Island, southern North Island, Christchurch, and southern South Island in which 78% of all New Zealand live births occurred. Infants dying between the age of 28 days and 1 year (the postneonatal period) were enrolled in the study if the regional pathologist, in consultation with a local paediatrician, made a diagnosis of SIDS, with or without other abnormalities. The agreed protocol has been described previously, and cases were reviewed by the study pathologist if there was uncertainty. The controls were randomly selected from all births, except home births (less than 1%) in the study area. The protocol by which the cases were identified and how the control group was selected has been described in full elsewhere.8,9
The parents of both cases and controls were interviewed on a wide range of topics, including child care practices and minor illnesses. As the period before death for the cases was of particular interest, the controls were asked about a time on a nominated day. This was randomly assigned so that the distribution of the age of the controls and the time of day about which information was sought reflected the estimated distribution of the age and time of death of the cases. Information about the mother’s consumption of beer, wine, and spirits in the past month and about the occasion when most was drunk was also obtained, as well as the use of cannabis since the birth of the baby.
During the three year period, 485 SIDS occurred, a rate of 3.53 per 1000 live births. Obstetric records were examined for 465 (95.9%) of the cases and 1762 (97.9%) of the controls. Interviews with the parents were carried out for 393 (81.0%) of the cases and 1592 (89.6%) of the controls.
Age of death was taken as the mid point between the time the infant was last seen alive and the time he or she was found dead. The controls were assigned a time based on the beginning and end of the “last sleep”. For the purposes of this study, night was defined as the period between 10 pm and 7 30 am, a time that both parents and infants were likely to be asleep.
The daily minimum temperature obtained from meteorological offices in each region was used to estimate bedroom temperature, which was then used in a model to predict the appropriate insulation for the lower critical temperature or the temperature below which the metabolic rate of an infant would be likely to increase.10 As a comparison between deaths occurring during the day and at night was of particular interest, an allowance based on half the difference between the maximum and minimum temperature was made for the daytime deaths. Both cases and controls were divided into three groups: those whose bedding and clothing provided 2 tog too little insulation; those whose bedding and clothing was within 2 tog of the lower critical value; and those who had more than 2 tog extra.
A score representing illness based on the Baby Check System11,12 was obtained from data collected during the interview. As the cut off points were similar to those described in the original score, the infants were classified as having either mild or no symptoms, or requiring advice from or to be seen by a medical practitioner. Questions were asked about the frequency of sweating. The parents were also asked whether their baby was awake more, the same, or less than usual in the past two days. A similar question was asked about how easy it was for the baby to settle.
Logistic regression was used to compute the adjusted odds ratios for the multiplicative interactions between night/day and the other variables. The interactions were considered statistically significant if the change of deviance brought about by including a term for them in the logistic regression model was more than the critical value of the χ2 distribution using the appropriate degrees of freedom. The models were adjusted for variables that have been used in other reports from this study. These include: (a) sociodemographic factors: occupation, marital status, school leaving age, and mother’s age at birth of infant; (b) pregnancy factors: antenatal education class attended, months pregnancy when mother started attending antenatal clinic, number of previous pregnancies, and mother’s age at first pregnancy; (c) infant factors: sex of baby, ethnicity, birth weight, and gestation; and (d) postnatal factors: region, season, baby’s age, sleeping position, maternal smoking, breast feeding, and infant sharing bed with another person. Each effect was examined individually in the context of the multivariate model.
Ethical approval for this study was obtained from local ethics committees.
RESULTS
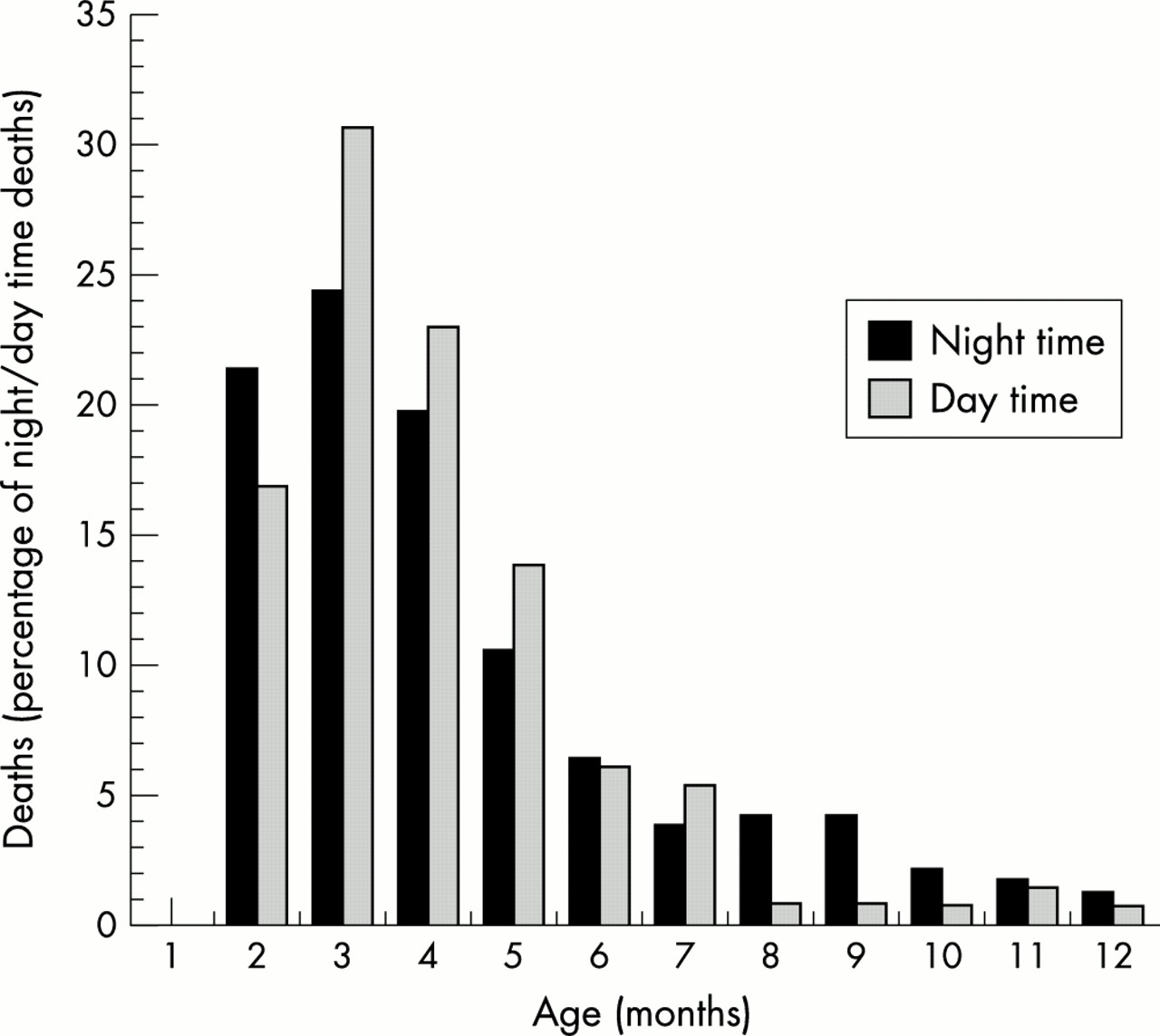
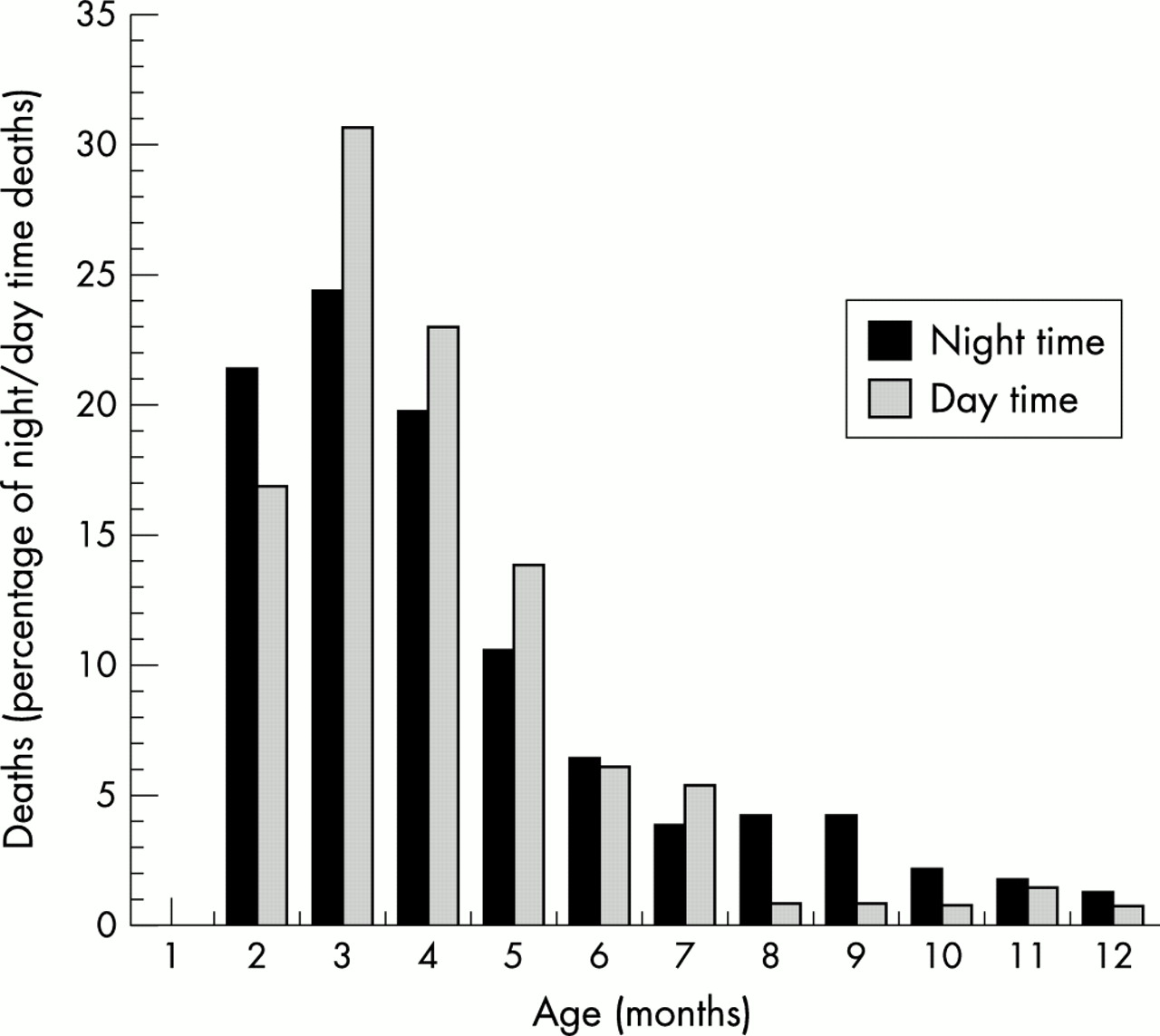
This report is based on 369 cases (of whom 238 (64.5%) died at night), and 1558 controls (822 (52.8%) of whose parents were interviewed about a night time sleep). The difference between the cases and controls was significant (χ2 = 16.60, df = 1, p = 0.001). Figure 1 shows the distribution for the time of death and the time of the nominated sleep for the controls. Figure 2 shows the distribution of the age of death for those dying at night and during the day. The median age for those dying at night was 12.9 weeks, and for those dying during the day 12.1 weeks. The difference between the medians was 0.8 (95% CI −1.1 to 2.9).

Distribution of the time of death for the cases and the equivalent nominated time for controls.
{kind=link}
{kind=link}
Distribution of the age of death for the cases.
Too little thermal insulation for the lower critical temperature was associated with an increased risk of SIDS at night (OR = 1.73; 95% CI 0.81 to 3.69) and during the day (OR = 2.46; 95% CI 1.02 to 5.89). The OR for too much thermal insulation was 1.26 (0.85 to 1.87) at night and 1.04 (0.64 to 1.69). The interaction effect was not significant (change in deviance = 1.12, df = 1, p = 0.57).
Table 1 shows the odds ratios and 95% confidence intervals for the four modifiable risk factors. The odds ratio for prone sleep position was 3.86 (2.67 to 5.59) at night and 7.25 (4.52 to 11.63) during the day. In this case the interaction effect was significant (change in deviance = 4.59, df = 1, p = 0.03). The difference between the odds ratios for breast feeding in the past two days for deaths occurring at night or in the daytime was not significant. The odds ratios for maternal smoking and bed sharing show that they were associated with an increased risk of SIDS at night. Because there was a significant interaction for prone sleep position and bed sharing, the sleeping arrangements for the last sleep were also examined (see table 1). Sleeping in a carry cot or a cocoon, and a variety of other arrangements, which included car seats and a separate mattress, were associated with an increased risk of SIDS during the night. The results for sleeping in the parents’ bed were consistent with those for bed sharing.
Odds ratios and 95% confidence intervals for four modifiable, sleeping arrangements and ethnicity risk factors for SIDS for night and daytime periods
Table 1 also shows the results for whether or not the mother was married, and ethnic group. Deaths were more likely to occur at night if the mother was not married, OR = 2.48 (1.62 to 3.78) compared with 1.25 (0.76 to 2.04) for the day. Being Maori was a risk factor for death at night, and being of Pacific Island origin was protective during the day. The results for attending antenatal clinics are also shown in the table; infants of mothers who did not receive antenatal care until they were at least 4 months pregnant were more likely to die at night, though the interaction was of borderline significance.
Table 2 shows the results for alcohol use, binge drinking, and cannabis use. Although the interaction effect for binge drinking was not quite statistically significant (p = 0.052), the risks associated with binge drinking and cannabis use were higher for babies dying at night.
Odds ratios and 95% confidence intervals for alcohol and cannabis use for night and daytime periods
Table 3 presents odds ratios for a trend across the three categories for illness and sweating. In each case the interaction effect was significant, increase in risk being higher for the night time period. Table 3 also shows the results for questions about how awake or how difficult the baby was to settle in the past two days. The interaction effects were significant, with the risk being higher at night if the baby was either more or less wakeful than usual, or more or less difficult to settle than usual.
Odds ratios and 95% confidence intervals for illness and symptom risk factors for night and daytime periods
The interaction effects between time of death and the other demographic, pregnancy, infant, and postnatal factors were not significant.
DISCUSSION
In this sample almost two thirds of SIDS deaths occurred at night. Although the period described as “at night” in this study was defined from the parents’ perspective, it was arbitrary. The definition was decided on before the analysis was carried out. It is possible that this has led to some misclassification, but as can be seen from fig 1, making night time earlier would transfer a similar proportion of cases and controls from one category to the other. The distribution of the time of death differed from the nominated times for the “last sleep”, which matched the expected distribution for the cases derived from an earlier study,13 so a smaller proportion of controls were interviewed about a night time sleep. However, as there is no reason to believe that there were differences between the controls interviewed about night and daytime sleeps, the results should not be affected. We should, of course, be cautious about the interpretation of the results, because the analysis was not based on hypotheses drawn from earlier studies.
Because the cases and controls were frequency matched for age as part of the design of the study, the hypothesis related to sleep in the night time period was tested within the cases. Although fig 1 suggests that night time deaths were more common in older children, the estimate of the difference was 0.8 (−1.1 to 2.9) weeks. Thus, our results do not support the hypothesis that night time deaths were more common in older children because their sleep becomes more concentrated at night.
Our second hypothesis, which suggested that prone sleep position could operate through a thermal mechanism, making insulation from bedding and clothing more important at night, must also be rejected. The patterns for both too few togs and too many togs for the lower critical temperature were similar for both day and night. Our third hypothesis was that different arousal responses because of fewer stimuli at night could account for an increased risk for prone sleep position at night. Our data show that infants who were less awake and less difficult to settle than usual, which could result in them being less responsive than usual to external stimuli, were at greater risk of SIDS. However, this does not support our hypothesis that prone sleep position would be a stronger risk factor at night. Finally, we examined sleeping arrangements. Interestingly, only about half the cases slept in their own cot or bassinet either at night or during the day. Carry cots or cocoons and a range of other arrangements increased the risk of SIDS at night, but do not explain the increased risk of prone sleep position during the day.
On their own bed sharing, maternal smoking, and being a single mother were associated with an increased risk of SIDS at night but not in the daytime. All have been identified as risk factors in earlier reports from this study,8,9,14 and smoking is still regarded as a modifiable risk factor and a major contributor to SIDS.15 A combination of smoking and bed sharing has already been shown to increase the risk of SIDS above that of either smoking or bed sharing alone.16 While accepting that smoking is harmful to babies, it has been argued that its strong relation with deprivation makes the association difficult to interpret.17 There is also evidence that both taking up and stopping smoking are influenced by material circumstances.17 Single motherhood has been shown to be associated with being Maori, having a lower family income, having a lower educational status, and coming from socially deprived areas.18 Table 1 shows that both maternal smoking and being an unmarried mother were more common for babies who died at night, with only 21% having neither risk factor. The comparable figure for cases dying during the day was 34%. The figures for the controls were 57% and 58%. More of the mothers whose babies died at night had not received antenatal care in early pregnancy. It also seems that many infants do not have their own bed. This, together with the results for binge drinking and cannabis use, is consistent with the notion that babies who die at night come from a more socially deprived or more disorganised section of society. Thus, the concomitants of social deprivation may be as important as maternal smoking itself.
The results of this study also show that the risk of SIDS associated with illness or sweating is higher at night. It is possible that factors such as being a single mother, or not being accustomed to seek appropriate medical care, made looking after a new baby more difficult. Parental inexperience, tiredness, and the responsibility of caring for a new baby, on the other hand, may make it harder to respond to signs of illnes.
This study, which was designed to have sufficient power to detect interaction effects, some of which have been reported before,10,16 has found important differences between risk factors for SIDS occurring at night and during the day. Where the interactions were significant or almost so, the difference was in the order of twofold. Prone sleep position was strongly associated with SIDS at night, so the increased risk during the day is particularly noteworthy. Night time deaths were more strongly related to markers of social deprivation, some of which were not associated, or only weakly associated with deaths occuring during the day. The combination of factors that increase the risk SIDS at night suggests that the degree of detailed attentiveness or observation of the baby may be of special importance in nocturnal deaths.
Acknowledgments
The study was funded by the Health Research Council of New Zealand (HRCNZ) and the Hawkes Bay Medical Research Foundation. The authors thank the research interviewers who undertook interviews and the various Plunket Society branches who paid their travelling expenses. They also acknowledge the contributions of the New Zealand Cot Death Study group: EM Allen, DMO Becroft, RPK Ford, IB Hassall, R Scragg, AW Stewart, and J Thompson.
REFERENCES
Linked Articles
- Miscellaneous