Article Text

Abstract
Aim: To describe the epidemiology of congenital anomalies in Glasgow with special reference to secular trends.
Methods: The prevalence of congenital anomalies was determined retrospectively in 233 777 births using the Glasgow Register of Congenital Anomalies for the period 1980–97.
Results: The total prevalence of congenital anomalies was 324 per 10 000 births, declining by just over a third from 382 per 10 000 births in 1980 to 238 per 10 000 births in 1997. The categories of defects with the highest prevalence were congenital heart disease (50 per 10 000 births), anomalies of limbs (49 per 10 000 births), and digestive system anomalies (47 per 10 000 births). Prevalence in most categories of anomaly declined, including those of the ear (−88%), congenital heart disease (−69%), anomalies of integument (−67%), nervous system anomalies (−61%), anomalies of limb (−54%), and urogenital (including renal) anomalies (−31%). By contrast, there was a significant upward trend for chromosomal anomalies (+50%).
Conclusions: Despite the decline in the prevalence of many types of congenital anomaly, around 2.5% of all births in Glasgow were still associated with these disorders in 1997. In attempting to explain the prevalence and secular trend of congenital anomalies in Glasgow, underlying contributing factors require to be considered. These include changes in case ascertainment, antenatal screening, and diagnostic methods.
- congenital anomalies
- prevalence
- secular trend
- EUROCAT, European Register of Congenital Anomalies
- GRCA, Glasgow Register of Congenital Anomalies
Statistics from Altmetric.com
About 2–3% of births are associated with major congenital anomalies diagnosed at or soon after birth. Despite the fact that the birth prevalence of some types of congenital anomalies has been declining during the past two decades in some countries,1–6 they are still a major cause of perinatal mortality and childhood disability in Europe. With the control of infectious disease and malnutrition, particularly in developed countries, congenital anomalies are now making a proportionally greater contribution to ill health in childhood.7
The purpose of the present study was to provide a descriptive overview of the epidemiology of congenital anomalies in Glasgow and specifically to answer two questions: (1) What is the prevalence of congenital anomalies? (2) Has there been a recent secular change in the prevalence of congenital anomalies?
METHODS
Congenital anomalies were defined as structural defects, chromosomal abnormalities, inborn errors of metabolism, and hereditary disease diagnosed before, at, or after birth. The source of data was the Glasgow Register of Congenital Anomalies (GRCA), a population based registry covering all mothers resident within the boundaries of the Greater Glasgow Health Board, Glasgow, Scotland, UK. The GRCA has been systematically validated.8,9 In common with the other registries in the transnational EUROCAT (European Registration of Congenital Anomalies) network, the GRCA uses the ICD based coding system of the British Paediatric Association Classification of Disease.10 Cases comprised congenital anomalies identified in live births, stillbirths, and induced abortions following prenatal diagnosis. Spontaneous abortions were excluded. There was no formal time limit for registration of newly diagnosed cases. Multiple sources of ascertainment of cases were used. The main sources of ascertainment were hospital records, routine hospital discharge forms, postmortem reports, perinatal meetings, medical genetics records, paediatric discharge letters, health visitor notifications, and stillbirth and death registers. Whatever the source of ascertainment, cases were carefully reviewed both locally (by an experienced clerical officer) and at the EUROCAT central registry (by a paediatrician specialising in pathology and genetics) to validate the diagnostic information.
Total prevalence was calculated by dividing the numerator (registered cases of congenital anomalies) by the relevant denominator (total live and stillbirths)11 for the same period of time. An infant/fetus with more than one anomaly was counted once only based on the primary diagnosis.
We calculated 95% confidence intervals (CI) for each prevalence rate. Linear regression analysis was performed to assess the secular trend of congenital anomalies, where the dependent variable was the prevalence of defects and the predictor was the birth year from 1980 to 1997. Using the regression equation, the prevalence rate was predicted for all groups of congenital anomalies over time. The predicted rate in the first year of observation (1980) was subtracted from the rate at the end of the study period (1997) to give an estimate of the overall secular proportional change (in percent) in the frequency of anomalies.
All tables and graphs were generated using Microsoft Excel 1997. Linear regression analysis was performed in Minitab Release 10.51 Xtra.
RESULTS
Over the study period (1980–97), a total of 223 777 births were surveyed, of which 222 390 (99.4%) were live births and 1387 (0.6%) stillbirths. During this period, 7250 cases with a primary diagnosis of congenital anomaly were ascertained, representing an overall prevalence rate of 324 per 10 000 births (95% CI: 317 to 331).
Table 1 and fig 1 show the total prevalence and secular trend of all congenital anomalies in Glasgow between 1980 and 1997. The total prevalence of congenital anomalies declined by 38% from 382 per 10 000 births in 1980 (95% CI: 350 to 414) to 238 per 10 000 births in 1997 (95% CI: 210 to 266).
Total number and prevalence (rates per 10 000 live births and stillbirths) of congenital anomalies, Glasgow, 1980–97

Total prevalence (with 95% CI) of congenital anomalies by year in Glasgow, 1980–97.
Table 2 and fig 2 show the prevalence of the main categories of congenital anomalies. The categories with the highest rates were congenital heart disease (50 per 10 000 births, 95% CI: 47 to 53), anomalies of limb (49 per 10 000 births, 95% CI: 46 to 52), and digestive system anomalies (47 per 10 000 births, 95% CI: 44 to 50). By contrast, the prevalence rates of anomalies of the ear, respiratory system, and eye were all less than 5 per 10 000 births.
Prevalence (rates per 10 000 live births and stillbirths) of congenital anomalies, Glasgow, 1980–97

Prevalence (with 95% CI) of categories of congenital anomalies, Glasgow, 1980–97.
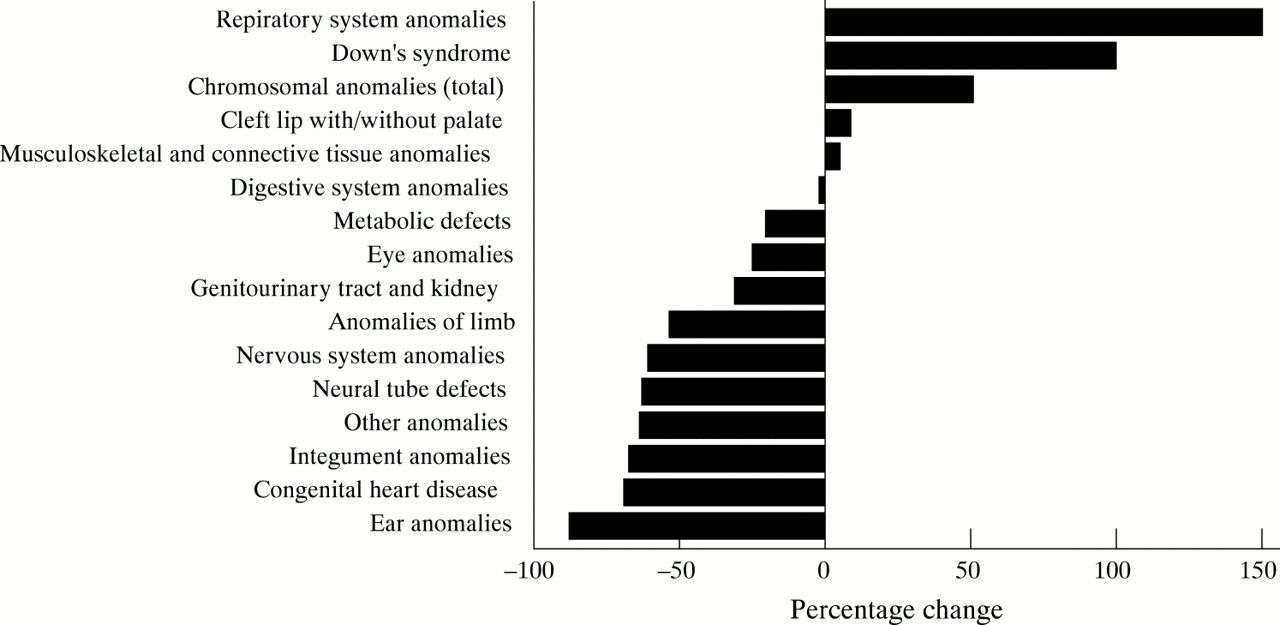
Figure 3 shows the secular trends for selected groups of anomalies. Table 3 and fig 4 show the percentage change (derived from the regression analyses) in the prevalence of congenital anomalies between 1980 and 1997. There was a statistically significant upward secular trend for Down's syndrome (+100%, p = 0.003) and chromosomal anomalies as a whole (+50%, p = 0.015). The upward trend for respiratory system anomalies (+150%), cleft lip with/without palate (+8%), and musculoskeletal and connective tissue anomalies (+4%) did not reach statistical significance. By contrast, there was a decrease in the prevalence of most other anomalies, notably ear anomalies (−88%, p = 0.015), congenital heart disease (−69%, p < 0.001), integument anomalies [defined as skin and its appendages, hair, nails, and sweat and sebaceous glands; according to the EUROCAT definition based on ICD-9, those anomalies comprise codes 7570-5, 7578-9, 6851, 2140, 2169, 2280-1] (−67%, p = 0.007), other anomalies (−64%, p = 0.002), neural tube defects (−63%, p < 0.001), nervous system anomalies (−61%, p < 0.001), anomalies of limb (−54%, p < 0.001), anomalies of external and internal genitals, and anomalies of the urinary tract and kidney (−31%, p = 0.013). The decline in the prevalence of eye anomalies (−25%), metabolic defects (−20%), and digestive system anomalies (−2%) was not statistically significant.
Change in the prevalence of congenital anomalies, Glasgow, 1980–97

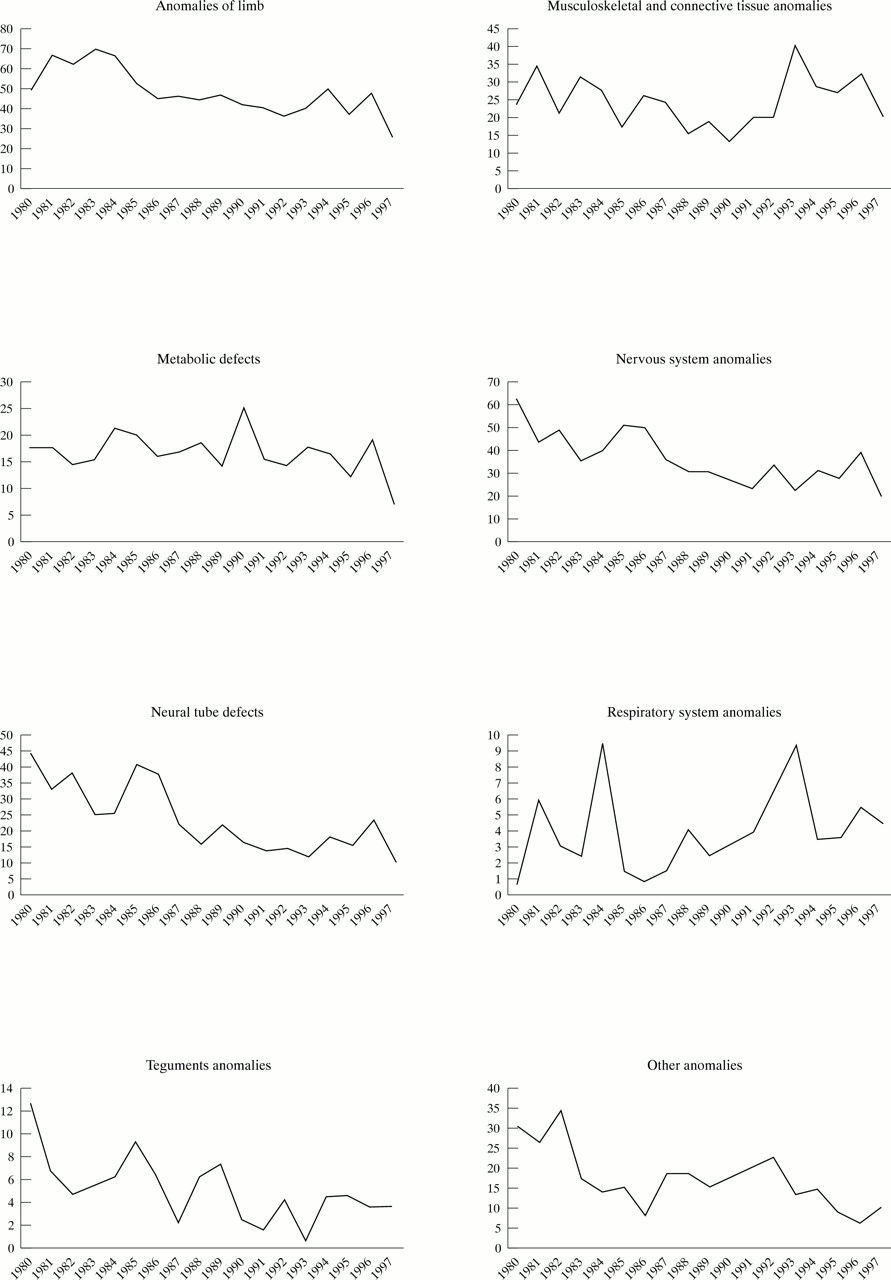
Secular trend in prevalence (rates per 10 000 births) for selected groups of congenital anomalies, Glasgow, 1980–97.

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Percentage change in the prevalance of congenital anomalies from 1980 to 1997, Glasgow.
DISCUSSION
Prevalence studies of congenital anomalies are useful to establish baseline rates, to document changes over time, and to identify clues to aetiology. They are also important for planning and evaluating antenatal screening for congenital anomalies, particularly in high risk populations.
The total prevalence of congenital anomalies in this study was 324 per 10 000 births, 27% higher than the average rate for all EUROCAT centres (236 per 10 000 births over 1980–94).12 The prevalence rates of congenital heart disease, total chromosomal anomalies, and Down's syndrome were slightly lower than the average EUROCAT rates (−12%, −16%, and −13%, respectively). The Glasgow rates were higher for cleft lip (+32%), digestive system anomalies (+73%), nervous system anomalies (+46%), and neural tube defects (+64%).
Although the overall prevalence of congenital anomalies for European centres in the EUROCAT network declined from 269 per 10 000 in 1980 to 234 per 10 000 in 1994, registries in France, Belgium, Malta, Switzerland, Spain, and Italy reported increasing rates over time. British (including Glasgow), Irish, Dutch, and Danish registers reported a declining trend.
The main finding of the present study was that Glasgow experienced an overall downward trend in the prevalence of congenital anomalies as a whole from 1980 to 1997. The pattern was not, however, consistent across all categories: there was a significant increase in the prevalence of chromosomal anomalies, notably Down's syndrome. The apparent upward secular trends in the prevalence of respiratory system anomalies, cleft lip with/without palate, and musculoskletal and connective tissue anomalies were not significant, possibly because of small numbers. All other groups of anomalies experienced an overall downward secular trend.
Neural tube defect is one of the most frequent types of defects and one of the leading causes of the fetal and infant mortality caused by congenital anomalies around the world. Historically, Glasgow had a relatively high prevalence compared to other parts of Europe,13 but the recent steep decline in prevalence suggests that this may no longer be the case.
In seeking to explain geographical and secular trends, potential underlying contributing factors should be considered. Case ascertainment methods, including data collection, sources of information, and type of notification of fetal death, may vary in place and time. Although we cannot rule out the impact of these factors in our data, we suspect they are of minor importance given the relative methodological consistency with which the Glasgow data were collected and analysed over time. Improving antenatal screening and prenatal diagnosis may, however, have increased the ascertainment rate and therefore the prevalence of some anomalies.
Demographic and environmental factors14,15 may influence the prevalence of anomalies. Maternal age is strongly associated with the prevalence of chromosomal anomalies, especially Down's syndrome, and the rising proportion of older mothers is likely to have contributed substantially to the upward trend in the prevalence of this anomaly in Glasgow. Of the environmental factors, much attention has recently focused on the role of preconceptional vitamin supplementation (especially folic acid) for the primary prevention of congenital anomalies, particularly neural tube defects. As yet, however, there is little evidence of any major change in secular trend of neural tube defects attributable to folate supplementation.16,17
Finally, the particular pattern of prevalence, and the increasing trend of some groups of anomalies in Glasgow, reported by a register with good ascertainment and validated data, may give rise to speculation that there may be some specific local risk or causal factors for those anomalies. Although some studies have investigated this possibility, there is little supportive evidence. Macdonell and colleagues,18 for example, reported no relation between high concentrations of lead in domestic water supplies and neural tube defects, and Eizaguirre-Garcia and colleagues19 found no correlation between soil pollution with chromium waste and an increased risk of congenital anomalies.
In conclusion, this descriptive epidemiological study of congenital anomalies in Glasgow suggests that, despite a considerable decline in the prevalence of some types of congenital anomaly, around 2.5% of all births are still associated with these disorders. The apparently contrasting risk of congenital anomaly in Glasgow compared to other European centres and the declining prevalence of most types of anomaly remain largely unexplained.
Acknowledgments
We thank Mrs H Jordan and colleagues at the Greater Glasgow Health Board for their assistance with data collection and processing. Saeed Dastgiri and Dr Chi Le-Ha were sponsored by Tabriz University of Medical Sciences, Iran and the Wellcome Trust (grant reference number 050375/Z/97/Z) respectively. The GRCA is funded by the Greater Glasgow Health Board.