Article Text

Abstract
BACKGROUND Monitoring oesophageal pH conventionally detects “acid reflux” (pH less than 4). The pH of the gastric contents determines whether or not reflux can be detected.
AIM To monitor gastric and oesophageal pH simultaneously in order to determine the effect of milk feeds on gastric pH and how this would influence interpretation of the oesophageal pH record.
METHODS Milk fed infants for whom oesophageal pH monitoring was requested underwent simultaneous gastric and oesophageal pH monitoring using a dual channel pH probe.
RESULTS Twenty of 24 records were technically satisfactory. Mean reflux index was 1.0%, range 0.0–4.0%. Gastric pH was less than 4 for 24.5% (range 0.6–69.1%) of the total time. The average time the gastric pH was greater than 4 after feeds was 130 minutes (range 29–212 minutes). The corrected reflux index (limited to the time the gastric pH was less than 4) was 2.6% (range 0.0–11.0%).
CONCLUSION The pH of the gastric contents may be greater than 4 for prolonged intervals, during which oesophageal pH monitoring using current criteria cannot detect reflux nor correlate it with clinical events. A low reflux index may reflect prolonged buffering of gastric acidity rather than the absence of reflux.
- gastro-oesophageal reflux
- oesophageal pH monitoring
- gastric pH
Statistics from Altmetric.com
Gastro-oesophageal reflux is common in both term and preterm infants.1 Reflux may be manifest as vomiting or be implicated as a “silent” cause of aspiration pneumonia, apnoea, bradycardia, and apparent life threatening events,2 and may be an aggravating factor in some cases of neonatal chronic lung disease.3
Twenty four hour lower oesophageal pH monitoring4 is widely used to investigate patients suspected of having reflux and is increasingly being used in neonatal units.5 Standardised protocols for oesophageal pH monitoring are well established.6 The pH data obtained are generally analysed by dedicated software packages, which define reflux as a fall in oesophageal pH below 4. Summary measures are calculated to quantify the severity of the reflux. The principal measure is the reflux index,7 which is the percentage of the total recording time that the oesophageal pH is less than 4. It is also often important to determine if there is a temporal correlation between individual episodes of reflux and clinical events such as apnoea or bradycardia which are potentially life threatening.
The conventional pH cut off of less than 4 limits oesophageal pH monitoring to detecting “acid reflux”. Milk is both of neutral pH and a buffer of acid,8 and the pH of the gastric contents following milk feeds is raised for one to two hours.9 ,10Infants in neonatal units receive frequent feeds, often two to four hourly throughout the day and night. The gastric pH may therefore be above 4 for prolonged periods, limiting the time during which reflux can be detected by oesophageal pH monitoring.
In this study gastric and oesophageal pH were monitored simultaneously using a dual channel pH probe in symptomatic infants for whom oesophageal pH monitoring was requested. The aims of the study were to determine the effect of milk feeds on the pH of the gastric contents and the influence of this on the interpretation of the oesophageal pH record.
Methods
PATIENTS
Infants in the neonatal units of the Jubilee and Royal Maternity Hospitals in Belfast were recruited when a consultant neonatologist requested oesophageal pH monitoring. Infants had significant recurrent or persistent problems, such as apnoea, bradycardia, pneumonia, or neonatal chronic lung disease, with gastro-oesophageal reflux considered a probable underlying cause. They underwent simultaneous monitoring of gastric and oesophageal pH. The procedure was explained to the parents and written consent obtained. Ethical approval was granted by the Queen's University of Belfast Research Ethics Committee.
Eight girls and 14 boys were recruited. Two infants were studied twice. All were exclusively milk fed, receiving bolus feeds by orogastric tube, bottle, or by a combination of both methods. The range of intake was 135–180 ml/kg/day. The median (range) birth weight was 1474 (590–3120) g, gestation at birth was 29 (25–37) completed weeks, age at time of study was 32 (17–121) days, and weight at time of study was 2129 (800–3526) g. The indications for pH monitoring were recurrent apnoea/bradycardia/desaturation (n = 17), neonatal chronic lung disease (n = 3), feeding difficulties (n = 2), and recurrent/persistent pneumonia (n = 2).
pH MONITORING
Simultaneous records of gastric and oesophageal pH were obtained using a dual channel pH probe with two antimony electrodes 5 cm apart and a single internal reference electrode (GERoFlex, Johnson & Johnson). The electrodes were calibrated at pH 4 and pH 7 before and after monitoring. The probe was passed nasally and advanced to a distance placing the proximal electrode at 0.87 × (0.252 × body length + 5) cm.11 A chest radiograph was taken to confirm positioning of the proximal electrode in the lower third of the oesophagus and the distal electrode in the body of the stomach. Alteration to position was made if necessary and the probe was carefully secured.
pH was recorded every six seconds by a Flexilog 2000 ambulatory pH monitor (Oakfield Instruments Ltd, Oxford, UK). Feeding and nursing routines were not changed during the recording. Clinically significant signs and symptoms were recorded in an event diary by nursing staff.
DATA ANALYSIS
The pH data were analysed using dedicated software (Flexisoft II, Oakfield Instruments) and additional calculations were carried out using a computer spreadsheet (Microsoft Excel). All records underwent operator review to identify artefact, which was excluded from analysis. Calibration before and after recording quantified drift at the pH 4 cut off; this was linearly corrected using H+ concentration for the calculations.
The following were calculated for each gastric record:
- (1)
- Percentage of total time that gastric pH was less than 4
- (2)
- Average length of time after feeds that gastric pH was above 4 (if gastric pH did not fall back below 4, the time between feeds was used).
The following were calculated for each oesophageal record:
- (1)
- Reflux index: percentage of total time that oesophageal pH was less than 4
- (2)
- Corrected reflux index: percentage of time when gastric pH was less than 4 that oesophageal pH was less than 4
- (3)
- Percentage of time when gastric pH was greater than 4 that oesophageal pH was less than 4.
Results
Twenty four consecutive recordings were carried out on 22 infants. Twenty records were technically satisfactory. Records were excluded from analysis because of absence of postrecording calibration at pH 4 in three cases and artefact in one. Seventeen of the analysed records lasted for 24 hours but three were shortened to 22, nine, and eight hours by displacement of the probe.
Gastric pH was less than 4 for a mean of 24.5% (SD 17.3%; range 0.6–69.1%) of the total recording time. Figure 1 shows the distribution of these results. There was no simple correlation with weight, age, and postconceptional age.

Frequency distribution of percentage of total time gastric pH was less than 4.
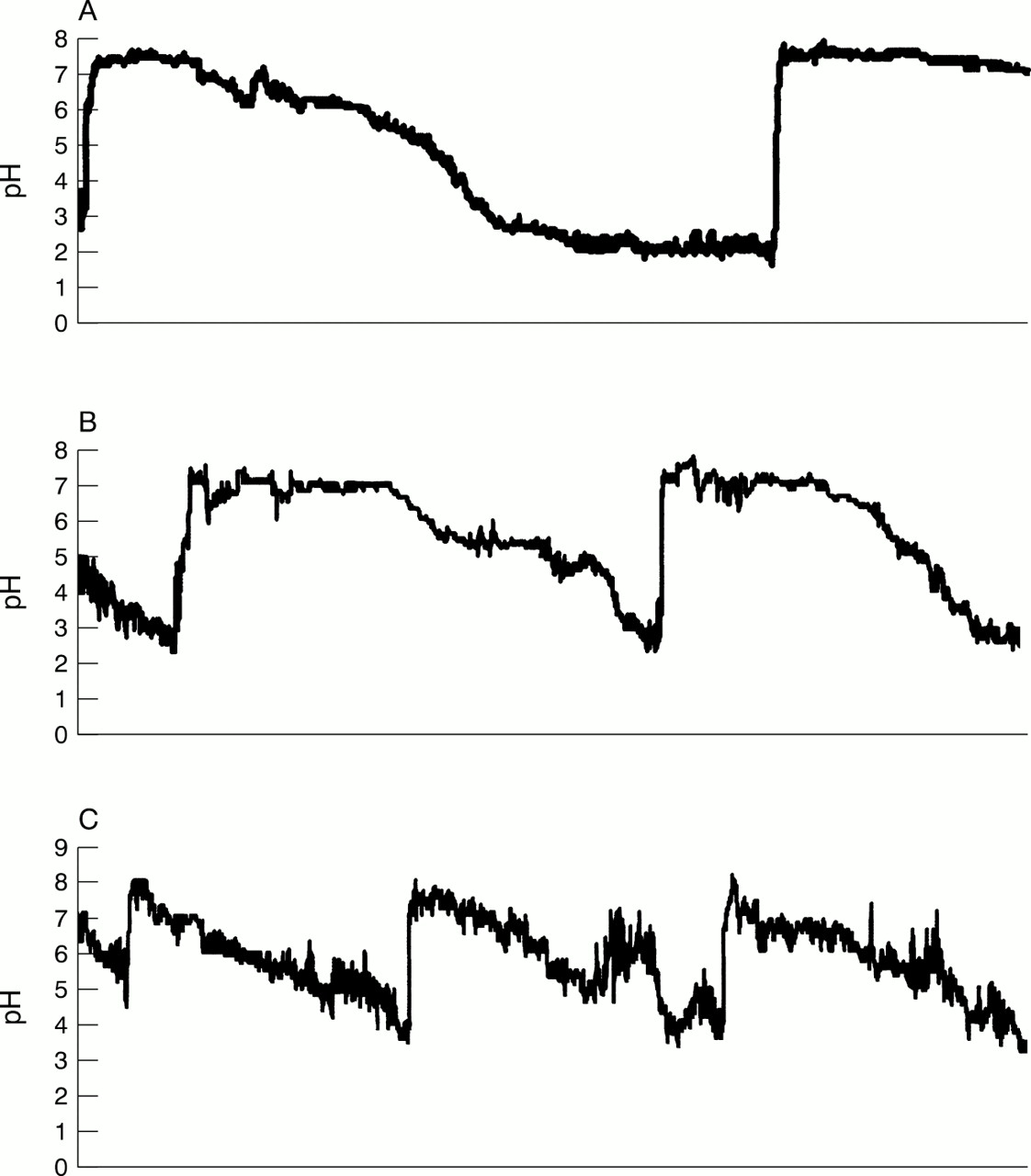
The average time gastric pH was greater than 4 after a feed was a mean of 130 minutes (SD 44 minutes; range 29–212 minutes). Figure 2 shows examples of gastric pH records.
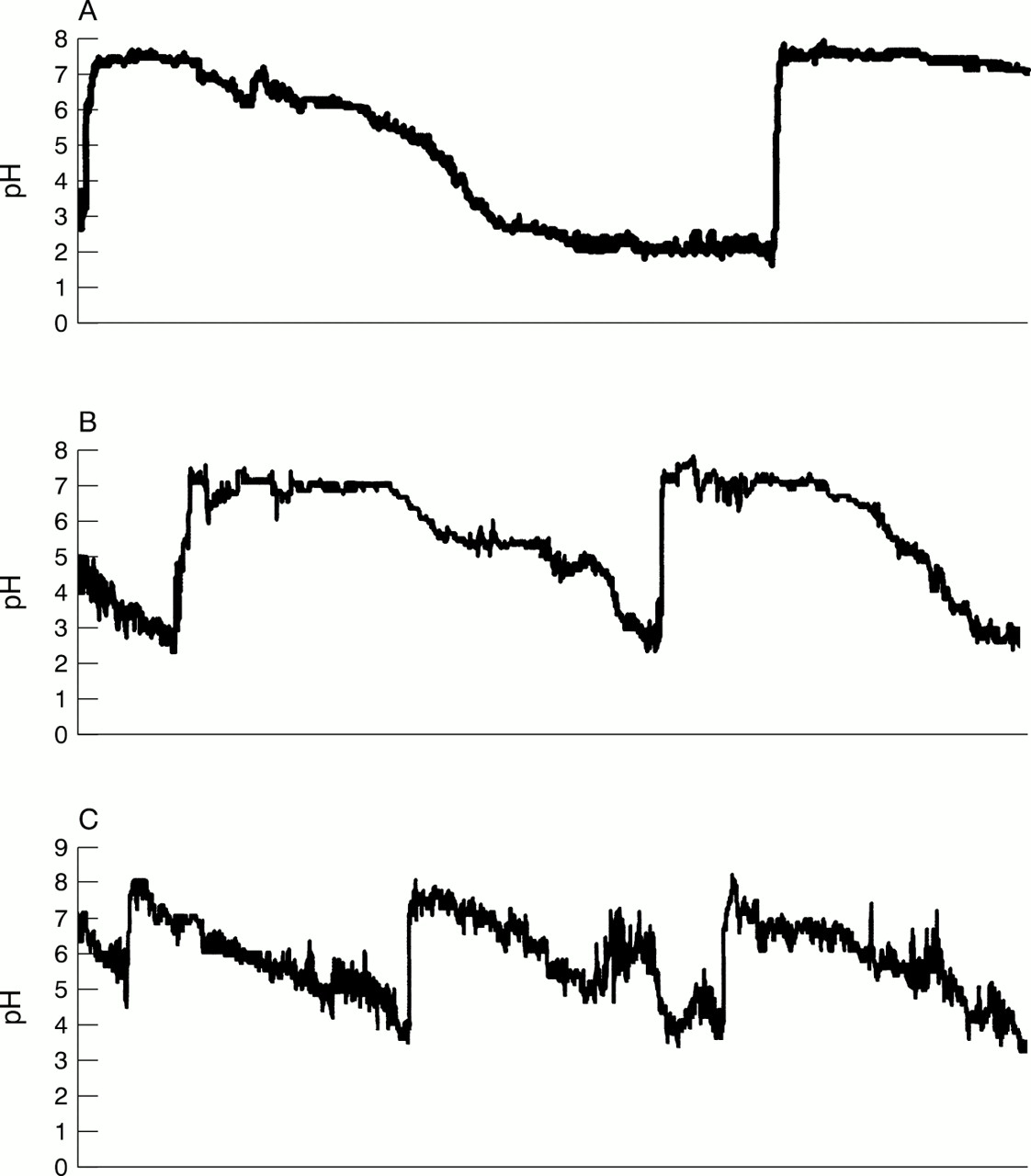
Examples of gastric pH records, six hour intervals: (A) four hourly feeds; (B) three hourly feeds; (C) two hourly feeds.
The reflux index was a mean of 1.0% (SD 1.4%; range 0.0–4.0%). The reflux index was recalculated as the percentage of time that the gastric pH was less than 4 that oesophageal pH was less than 4. This “corrected” reflux index was 2.6% (SD 3.3%; range 0.0–11.0%). Figure 3 shows the effect on individual results of this correction. No infants were categorised as having significant reflux by the reflux index and even when corrected to compensate for gastric buffering, only one infant was categorised as having moderate reflux (10–20%)12 and three as having mild reflux (5–10%).

Effect on individual results of correcting the reflux index by limiting it to apply to the time gastric pH was less than 4.
Acidification of the oesophagus when the gastric pH was greater than 4 was a mean of 0.3% (SD 0.3%; range 0.0–1.1%).
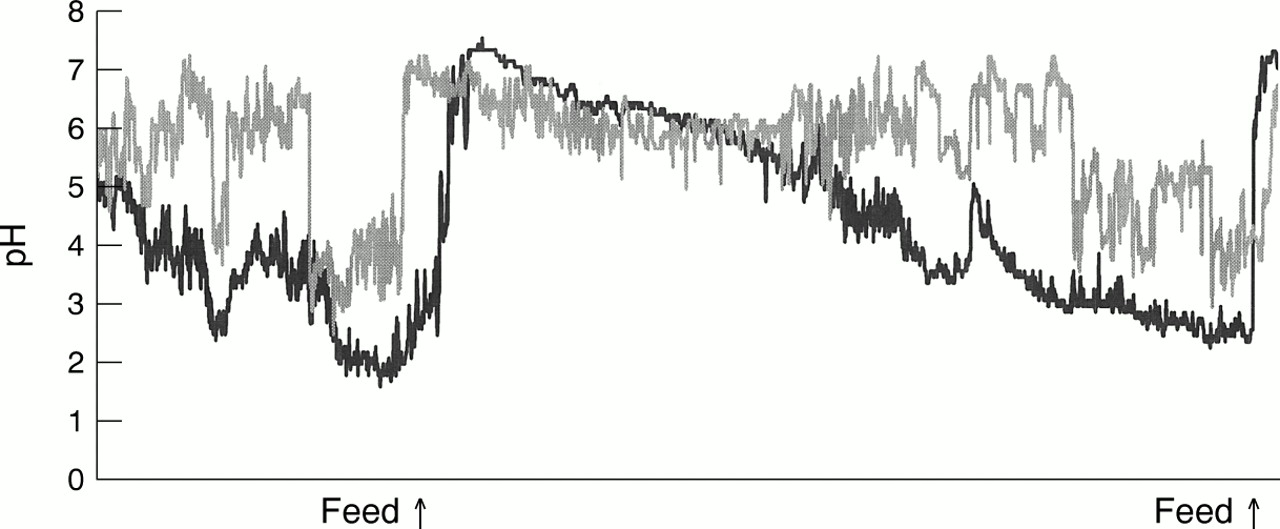
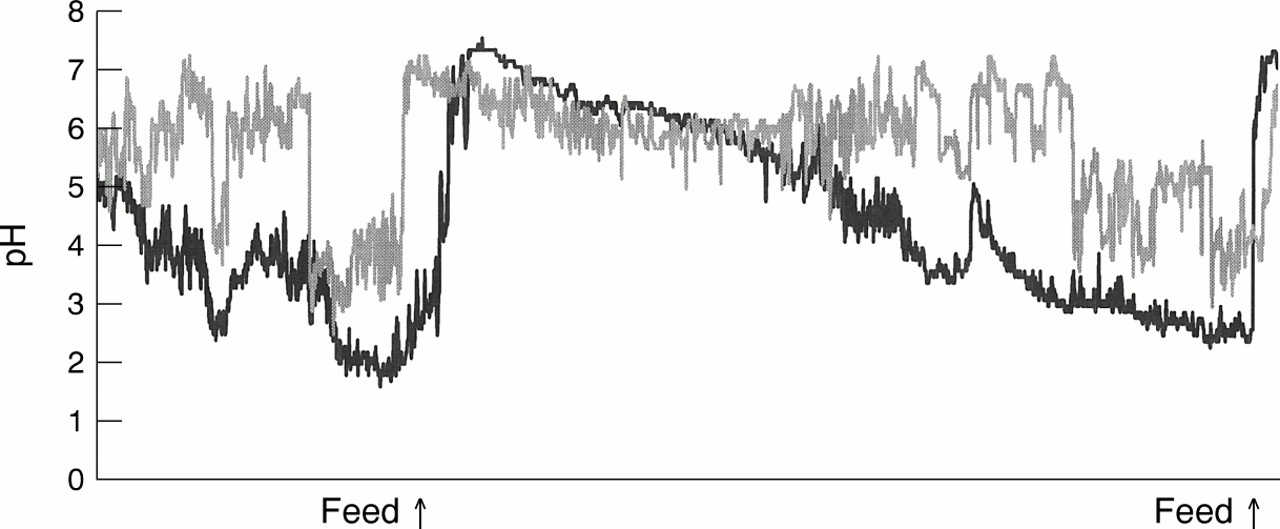
Operator review of the combined gastric and oesophageal records (fig 4) confirmed the prolonged periods of postprandial buffering during which reflux was not detectable. Oesophageal pH changes were also evident that may have indicated reflux but did not meet the criteria of a fall in oesophageal pH to less than 4.
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Simultaneous recording of gastric pH (black) and oesophageal pH (grey); four hour interval in an infant receiving three hourly tube feeds.
Discussion
The major indication for oesophageal pH monitoring in our neonatal units is to determine whether “silent” reflux may be the underlying cause of a range of problems such as apnoea, bradycardia, or pneumonia or whether it may be aggravating neonatal chronic lung disease.
Detection of reflux by oesophageal pH monitoring using conventional criteria requires that the gastric content be acid—that is, pH below 4. The buffering effect of milk on gastric acidity is known but its extent and the influence on the interpretation of oesophageal pH records had not been determined in neonates.
The gastric pH records of all infants showed buffering of gastric acidity following milk feeds. The average time that the gastric pH was greater than 4 after feeds was a mean of 130 (SD 45) minutes, and by definition any reflux that occurred during these periods of buffering could not be detected. The gastric pH was less than 4 for a mean of 24.5% (SD 17.3%) of the total time. This is less than that reported for older milk fed infants aged 1–17 months in whom the gastric pH was less than 4 for a mean of 42% (SEM 5%).8
Preterm and term infants in the early weeks of life have a weaker acid secretory response13 than older infants and adults despite higher gastrin levels.14 This, together with the frequent feeding of large volumes of milk, is the likely explanation for the often prolonged periods when gastric pH was greater than 4.
Our group of symptomatic infants had a reflux index of a mean of 1.0% (SD 1.4%), which is similar to values reported for asymptomatic term (1.20%, SD 0.91%)15 and preterm infants (0.7%, SD 1.1%).16 None of the infants in our study had a reflux index diagnostic of significant reflux.
The similarity of the reflux index of our symptomatic and the asymptomatic groups could arise either if reflux was not the cause of symptoms or if reflux could not be detected. A low reflux index should indicate that little reflux occurred, but our data reveal that an alternative explanation might be that buffering of gastric acidity prevented the detection of reflux. The gastric pH record allowed the distinction between a low reflux index reflecting the absence of reflux, or owing to buffering of gastric acidity.
A simultaneous record of gastric pH also allows the reflux index to be corrected by applying it only to the time when gastric pH was less than 4. This interval was, however, often short and excluded the postprandial period, which has been shown by scintigraphy,17 electrical impedance,18 and the use of apple juice feeds in older infants19 to be when the majority of reflux episodes occur. Correction of the reflux index in this way may therefore be a poor measure of the true severity of reflux.
The demonstration of a temporal relation between reflux episodes and clinical events is often a major goal in neonates, and requires that both be reliably identified and recorded. Reflux may occur during periods of buffering of gastric acidity and yet go undetected. Monitoring oesophageal pH alone may give the false impression that clinical events are not related to reflux. The gastric pH record allows the investigator to distinguish those intervals during which reflux could be detected and related to clinical events.
The wide variation in the time the gastric pH was less than 4, and the absence of a clear correlation with factors such as weight, age, and postconceptional age likely reflects the large number of factors that determine gastric acidity. These include feed composition, pH, and volume and gastric acid secretion and emptying. Many of these factors vary with both the maturity of and state of health of an infant. Changes in the reflux index may reflect changes in the gastric pH profile rather than a change in the amount of reflux.
In conclusion, we have shown limitations to monitoring oesophageal pH in milk fed infants. Gastric pH may be greater than 4 for long intervals during which oesophageal pH monitoring cannot detect reflux. This may prevent the identification of a temporal correlation between reflux episodes and clinical events. The reflux index may be low because of buffered gastric acidity rather than the absence of reflux. A record of gastric pH will reveal the extent of gastric buffering and alert an investigator to the possibility of false negative results of oesophageal pH monitoring.
Acknowledgments
Dr Mitchell was supported by a grant from the Research and Development Office for the Health and Personal Social Services in Northern Ireland.